My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
🧬 Interesting biology Good responders showed reduction in FOXP3+ Tregs, suggesting immune-microenvironment modulation.
⚠️ Safety Grade ≥3 toxicity: 14.7% No treatment-related deaths.
💡 Why this matters
Borderline OSCC often fails surgery after standard NACT. This low-dose IO + metronomic + chemo strategy may offer an affordable outpatient approach in LMIC settings.
But this is single-arm Phase II → randomized validation needed.
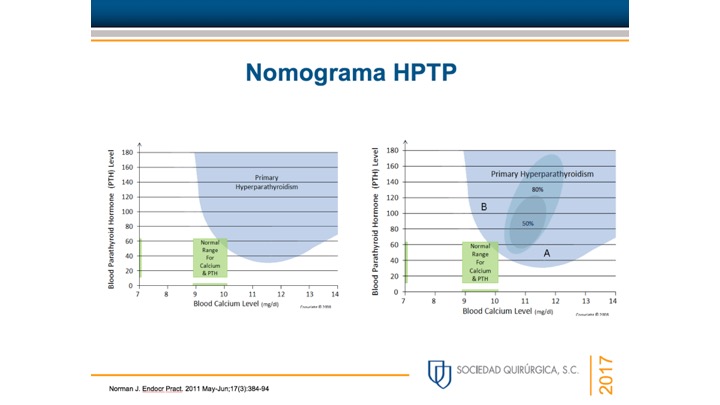
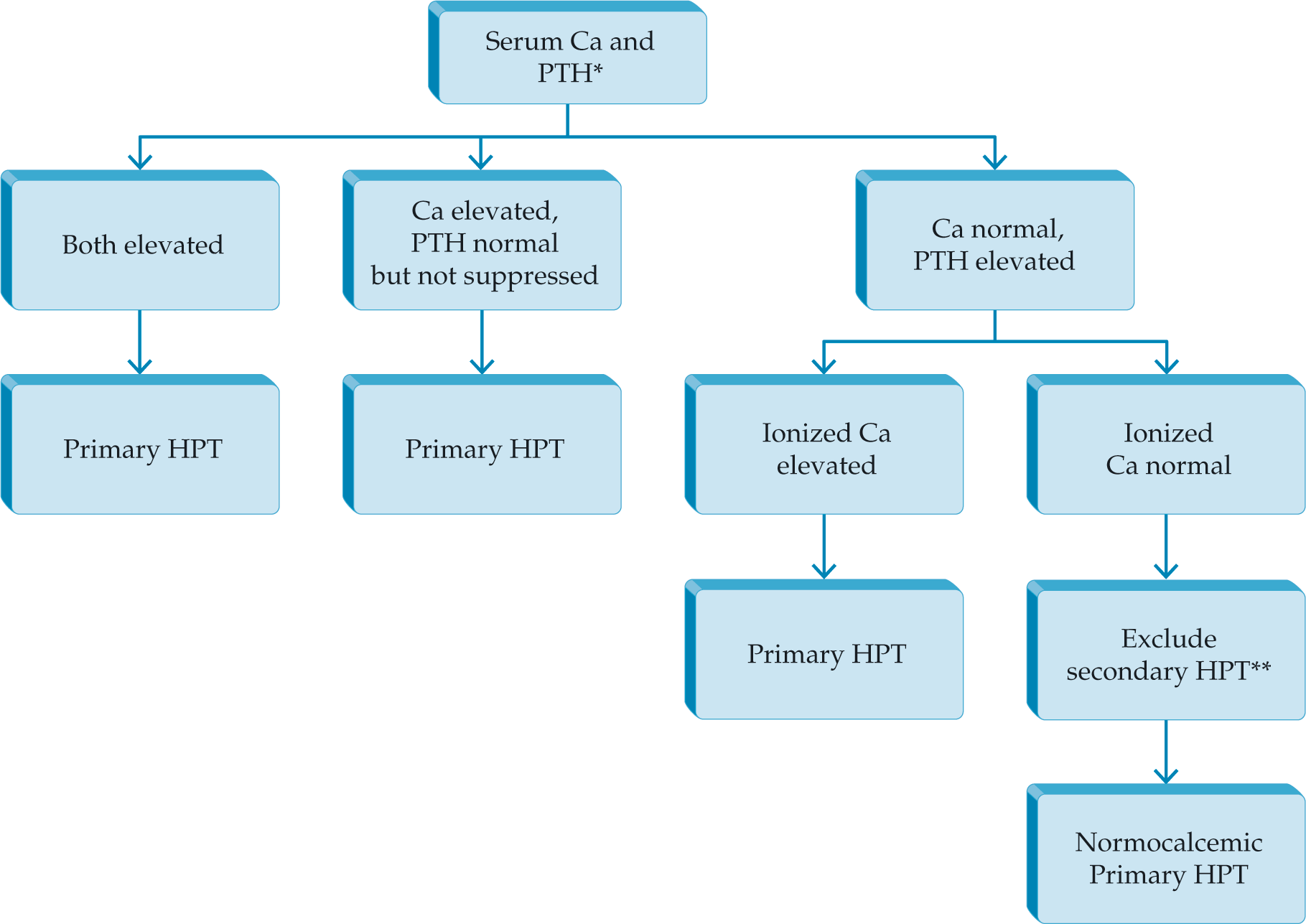
Context: Patients with elevated parathyroid hormone (PTH) and consistently normal serum calcium levels, in whom secondary causes of hyperparathyroidism have been excluded, may represent the earliest presentation of primary hyperparathyroidism (PHPT).
Objective: The objective of the study was to characterize patients with normocalcemic PHPT referred to a bone disease unit.
Design: This was a longitudinal cohort study.
Setting: Ambulatory patients were referred to the metabolic bone disease unit.
Patients: The study population included 37 patients [aged 58 yr, range 32–78; 95% female; serum calcium, 9.4 ± 0.1 (SEM) mg/dl (2.3 ± 0.02 mmol/liter), reference range, 8.5–10.4 (2.1–2.6 mmol/liter); PTH, 93 ± 5 pg/ml].
Interventions: Interventions included yearly (median 3 yr; range 1–8 yr) physical examination, biochemical indices, and bone mineral density (BMD).
Main Outcome Measures: We measured the development of features of PHPT.
Results: Evaluation for classical features of PHPT revealed a history of kidney stones in five (14%), fragility fractures in four (11%), and osteoporosis in 57% [spine (34%), hip (38%), and/or distal one third radius (28%)]. BMD did not show preferential bone loss at the distal one third radius (T scores: spine, −2.00 ± 0.25; hip, −1.84 ± 0.18; one third radius, −1.74 ± 0.22). Further signs of PHPT developed in 40% (seven hypercalcemia; one kidney stone; one fracture; two marked hypercalciuria; six had >10% BMD loss at one or more site(s) including four patients developing World Health Organization criteria for osteoporosis). Seven patients (three hypercalcemic, four persistently normocalcemic) underwent successful parathyroidectomy.
Conclusions: Patients seen in a referral center with normocalcemic hyperparathyroidism have more substantial skeletal involvement than is typical in PHPT and develop more features and complications over time. These patients may represent the earliest form of symptomatic, rather than asymptomatic, PHPT.
Lowe, Hyesoo et al. “Normocalcemic primary hyperparathyroidism: further characterization of a new clinical phenotype.” The Journal of clinical endocrinology and metabolism 92 8 (2007): 3001-5 .
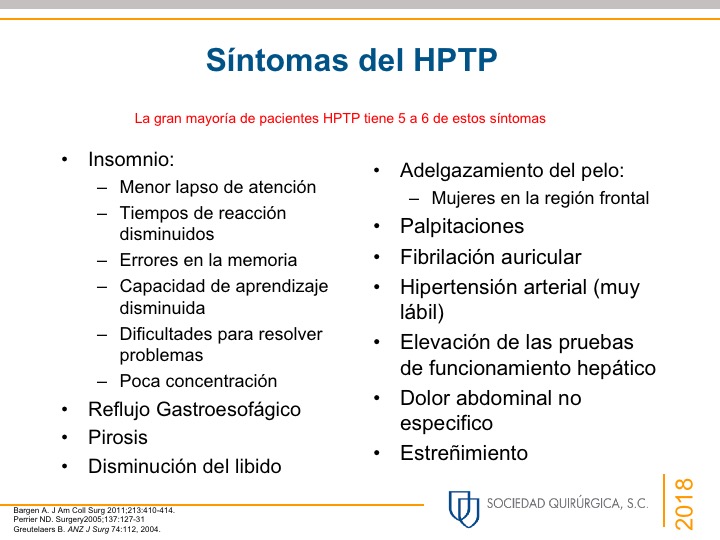
Thinning of the hair (specially in women in the frontal region)
Pruritus
Patients with PHPT also tend to score lower than healthy controls when evaluated by general multidimensional health assessment tools such as the Medical Outcomes Study Short-Form Health Survey(SF-36) and other specific questionnaires.
PHPT that is truly “asymptomatic” is a rare occurrence:
Seen in less than five percent of patients:
This is important when talking about management based on current guidelines
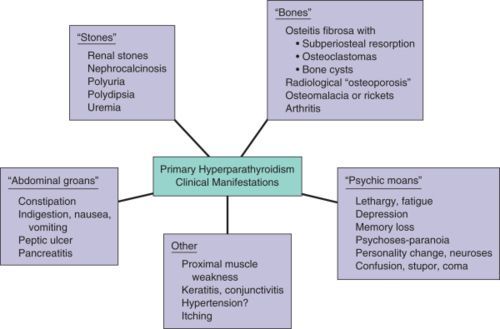
Patients with PHPT have some degree of renal dysfunction or symptoms:
In approximately 80% of the cases:
The renal manifestations implicated with PHPT are:
Decreased glomerular filtration rate
Hypercalciuria
Nephrolithiasis:
Nephrolithiasis was previously reported in approximately 40% to 80% of patients but now occur only in about 20% to 25% of the cases:
The pathophysiology is thought to be related to the filtered load of calcium in the glomerulus that increases proportionately with the degree of hypercalcaemia
Most renal stones in patients with PHPT are composed of calcium oxalate, although slightly alkaline urine may favor the precipitation of calcium phosphate stones:
Stone formers are more likely to be hypercalciuric, but less than one-third of the hypercalciuric patients with PHPT actually develop renal stones
Hypercalciuria is not a predictor of nephrolithiasis in patients with PHPT and is no longer considered as an indication for surgery
Nephrocalcinosis
Impaired urinary concentrating ability sometimes leading to polyuria, polydipsia, and nocturia
Reduced fractional phosphate reabsorption leading to hypophosphatemia
Increased urinary exertion of magnesium
Rodrigo Arrangoiz MS, MD, FACS, FSSO head and neck surgeon that specializes in parathyroid diseases that is a member of Mount Sinai Medical Center
Rodrigo Arrangoiz MS, MD, FACS, FSSO is a member of the American Thyroid Association:
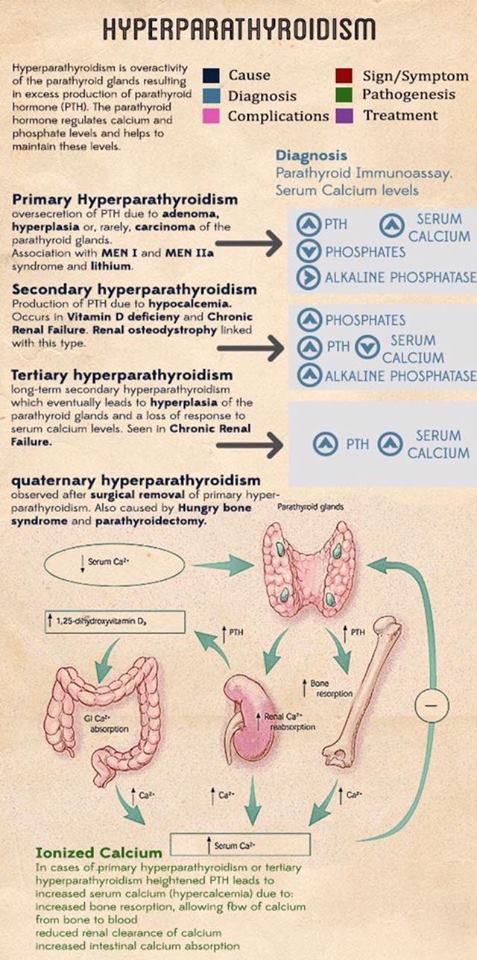
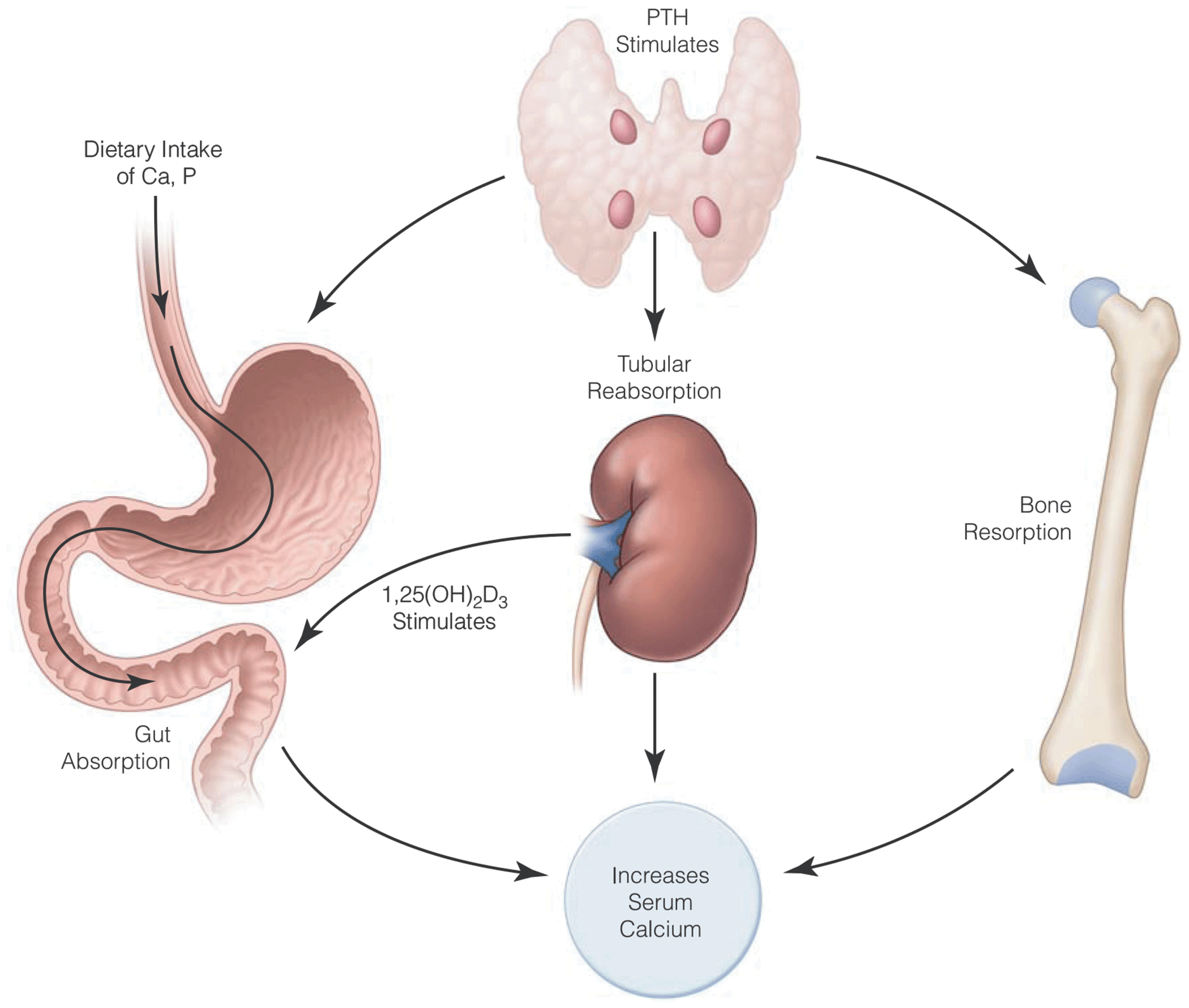
Is caused by an inappropriate, autonomous secretion of parathyroid hormone (PTH) by the parathyroid gland(s):
Which leads to an elevated serum calcium concentration or wide variations of the serum calcium concentration
Single gland disease:
Caused by a single, enlarged, overactive gland, is found in 85% to 90% of cases
Multiple gland disease occurs in 10% to 15% of the cases:
Multiple gland disease may consist of:
Double adenomas (6% to 9% of the cases)
Four-gland hyperplasia (3% of the cases)
Three enlarged and one normal appearing gland (0.3% of the cases).
Because asymmetric hyperplasia is common, it is difficult to distinguish between multiple adenomas and hyperplasia and the term multiple gland disease is preferred
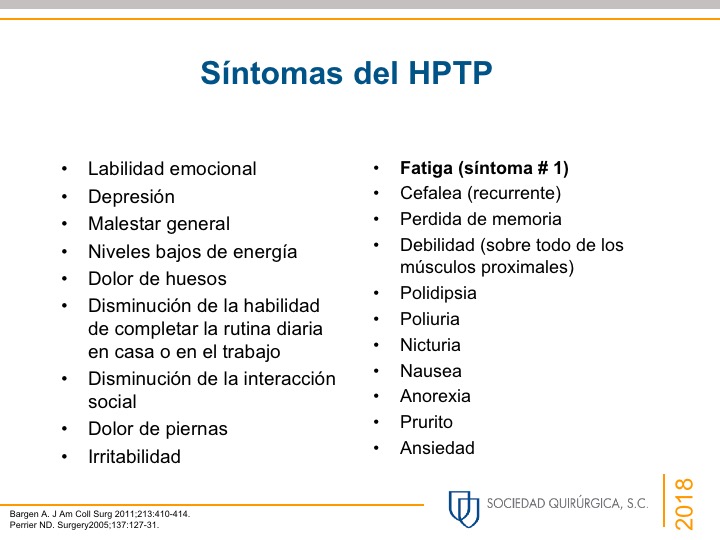
PHPT in the United States usually presents quite early:
Often when hypercalcemia is noted during routine laboratory testing
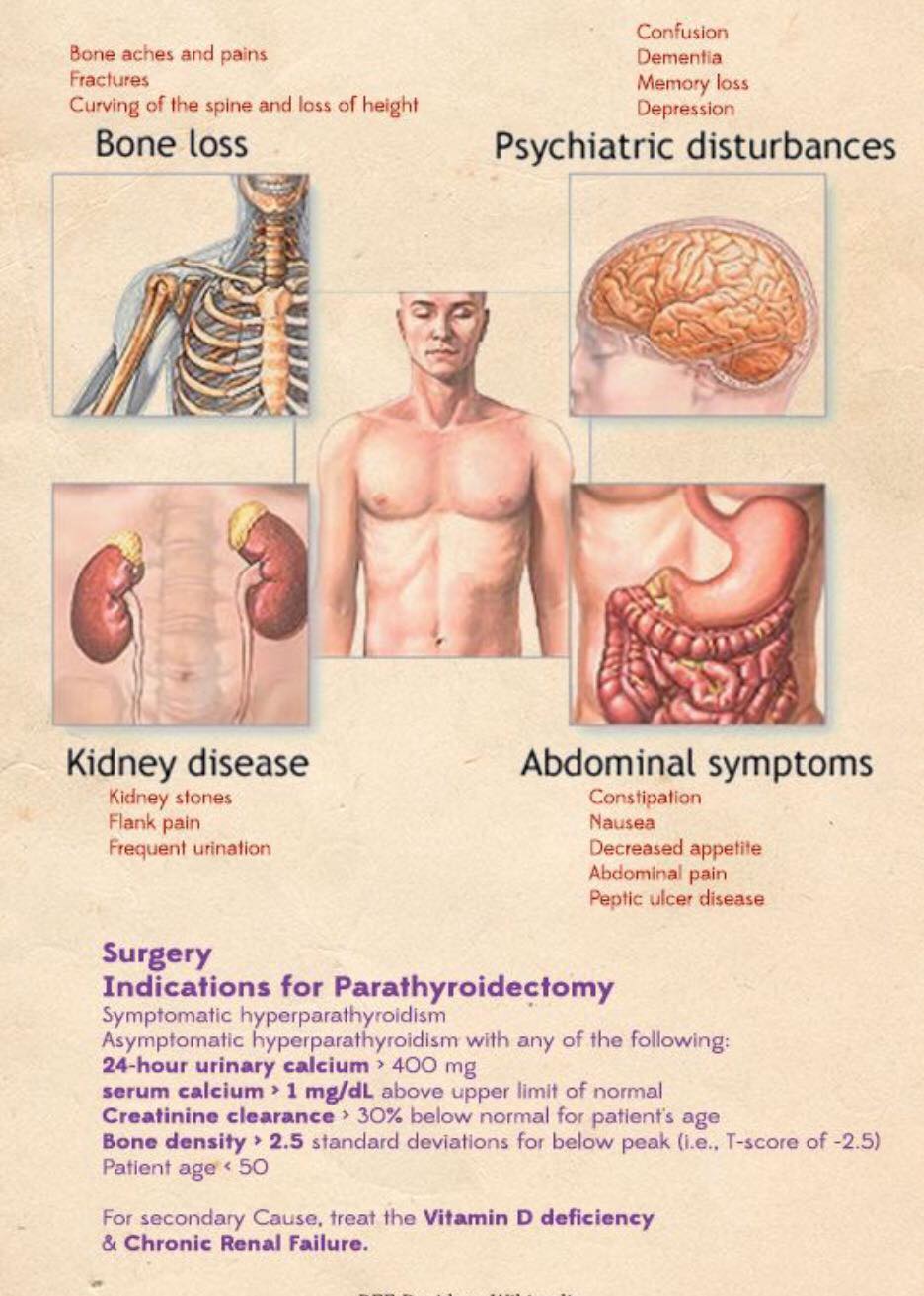
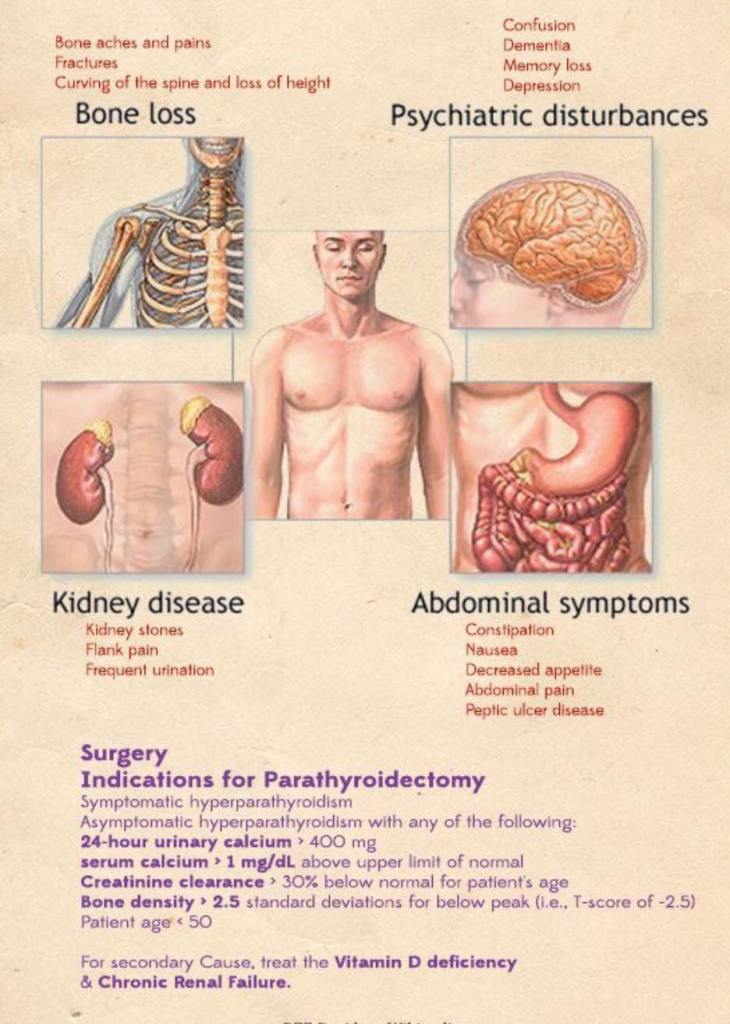
Signs may include:
Nephrolithiasis, decreased bone density, and fragility fractures, and subjective symptoms may include fatigue, cognitive changes, depression, constipation and other gastrointestinal complaints, musculoskeletal pain, nocturia, and rarely pruritus:
Many patients may appear asymptomatic:
A detailed history often uncovers symptoms:
95% of the cases have symptoms when appropriate history is taken:
The recently revised guidelines for asymptomatic PHPT include a more extensive evaluation of the skeletal and renal systems
A family history of endocrine disorders should be investigated:
As hyperparathyroidism alone can be familial or can present as a component of multiple endocrine neoplasia (MEN) types 1 and 2A
Rodrigo Arrangoiz MS, MD, FACS cirujano de tumores de cabeza y cuello / cirugia endocrina miembro del equipo de Mount Sinai Medical Center experto en el manejo del hiperparatiroidismo primario.
Entrenamiento:
Cirugia general y gastrointestinal:
• Michigan State University:
• 2004 al 2010
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Maestria en ciencias (Clinical research for healthprofessionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• IFHNOS / Memorial Sloan Kettering Cancer Center:
Intraoperative rapid PTH does not itself define cure:
It is an intraoperative predictor of adequacy of resection
Formal cure after parathyroidectomy:
Is still biochemical eucalcemia lasting at least 6 months
Rapid PTH works:
Because intact PTH has a short half-life:
Roughly 3 to 5 minutes:
So levels should fall quickly after all hyperfunctioning tissue is removed
The AAES guidelines:
Recommend intraoperative PTH monitoring with a reliable protocol for minimally invasive parathyroidectomy:
They note cure rates of about 97% to 99% in selected patients when adjunctive IPM is used
Core concept:
The practical question in the OR is:
“Has all hypersecreting parathyroid tissue been removed?”
Rapid PTH helps answer that in real time
Most protocols use a baseline sample before incision and / or immediately before excision:
Then a post-excision level at 10 minutes, with an additional 20-minute sample when the decline is borderline or delayed
The most common reason the curve is misleading:
Is a PTH spike from gland manipulation:
Which is why many surgeons rely on the highest pre-incision or pre-excision value rather than only the pre-incision sample
Main intraoperative PTH protocols
The classic comparative study of 260 patients with concordant imaging:
Found overall accuracy of:
97.3% for Miami, 92.3% for Vienna, 83.8% for Rome, and 65% for Halle criteria
In that same study:
Miami criteria was the best-balanced criterion for predicting cure:
Whereas Rome and Halle were somewhat better for detecting multigland disease but at the cost of more negative conversions to bilateral exploration
The Miami criterion:
Is the most widely used:
A > 50% fall from the highestpre-incision or pre-excision PTH level, measured 10 minutes after excision of the abnormal gland
In the major Miami experience and subsequent reviews:
This approach achieved about 97% to 98% sensitivity, 97% specificity, ~99% PPV, and ~97% to 98% overall accuracy for postoperative eucalcemia
Long-term follow-up from the Miami group also showed durable outcomes with very low recurrence after focused surgery guided by intraoperative rapid PTH
This is why, in everyday endocrine surgery practice, the Miami criterion is usually the most useful protocol:
It is easy to remember, fast, reproducible, and has the best overall balance between avoiding persistent disease and avoiding unnecessary wider exploration
A 2024 network meta-analysis including 72 studies and 19,072 patients found that among conventional criteria:
The Miami criterion had the best diagnostic properties overall
Vienna criterion:
The Vienna criterion also uses a > 50% drop at 10 minutes:
But the reference is the defined pre-incision baseline rather than the highest pre-excision value
It was designed to standardize interpretation and improve identification of multigland disease
In the comparative dataset above:
Vienna performed well, with 92.3% overall accuracy:
But still not as well as Miami for routine prediction of cure
In practical terms, Vienna is reasonable if your team insists on a strict, fixed baseline, but it is less forgiving when pre-excision manipulation creates a spike:
That is one reason many high-volume groups prefer Miami’s use of the highest available baseline
Halle criterion:
Is much stricter:
Success is called only when PTH drops into the low-normal range:
Classically around 35 pg/mL:
Shortly after excision
This gives excellent specificity, but it performs poorly as a routine stopping rule because many successfully treated patients still have PTH levels above that threshold intraoperatively:
Especially if starting levels are high or clearance is delayed
In the Barczyński comparison, Halle had 100% specificity but only 65% overall accuracy:
Meaning it would trigger many unnecessary further explorations
For that reason, Halle is usually not the best default criterion for standard sporadic PHPT with concordant imaging:
It is too strict for routine use
Rome criterion:
Is a more complex, stricter protocol
In one description, it requires a > 50% fall from the highest pre-excision level and / or a value within the normal range and / or an additional fall by 20 minutes
The point of Rome is to improve detection of persistence and multigland disease:
Especially when the early curve is ambiguous
A 2022 study evaluating the Rome approach found that the 20-minute / baseline ratio:
Had the highest diagnostic significance and suggested the 20-minute sample is particularly informative
Rome can be useful when the 10-minute value is borderline, when preoperative localization is less reliable, or when multigland disease is a real concern:
But as a standard protocol for all focused cases, it adds complexity and tends to increase exploration without clearly outperforming Miami for overall cure prediction
What do meta-analyses say about using ioPTH at all?
Beyond comparing criteria, the broader question is whether using ioPTH improves outcomes
A 2021 systematic review / meta-analysis of 28 studies and 13,323 patients found operative failure rates of 3.2% with ioPTH versus 5.8% without ioPTH:
With a significant reduction in persistent / recurrent PHPT when ioPTH was used
Another 2021 systematic review / meta-analysis focused on minimally invasive parathyroidectomy included 12 studies and 2,290 patients and found that ioPTH use was associated with higher cure rates (OR 3.88, 95% CI 2.12–7.10) and a lower need for reoperation:
It did increase conversion to bilateral exploration, but without higher morbidity
So the evidence supports the value of ioPTH, especially when doing focused or minimally invasive surgery and when multigland disease is a concern
Are stricter cutoffs better?
Usually, not enough to justify routine adoption
Newer work continues to test stricter thresholds:
A 2025 ROC analysis found that a 60% drop gave the best balance of sensitivity and specificity in that cohort, outperforming 50% and 70% on AUC, but the authors also cautioned that stricter thresholds may cause overtreatment and unnecessary exploration
Similarly, a 2025 two-center study suggested that combining the Miami rule with normalization to the reference range may help in selected cases, but the overall literature still favors the Miami criterion as the best general-purpose rule, which is consistent with the large network meta-analysis
Practical interpretation in the OR
A resident-friendly approach is:
Draw pre-incision and pre-excision PTH
Remove the suspected gland
Check 10-minute PTH
If > 50% drop from the highest baseline → likely cure, stop if anatomy and clinical context fit
If borderline or not adequate → wait for 20-minute level and continue exploration if still not satisfactory
That approach handles the common real-life issues:
Manipulation spikes, delayed clearance, and occult multigland disease
When rapid PTH is especially helpful:
Rapid PTH is most helpful in:
Focused / minimally invasive parathyroidectomy
Discordant or equivocal localization
Suspicion for multigland disease
Reoperative surgery
Cases where confirmation of adequacy of excision will determine whether you stop or proceed to wider exploration
Bottom line: which protocol is most useful?
For most sporadic PHPT cases, especially with focused surgery:
The Miami criterion is the most useful protocol:
It has the best combination of simplicity, speed, evidence base, and diagnostic performance, and it remains the most widely adopted and best-supported criterion in comparative studies and network meta-analysis
Key references:
Wilhelm SM, et al. AAES Guidelines for Definitive Management of Primary Hyperparathyroidism. JAMA Surg. 2016.
Barczyński M, et al. Evaluation of Halle, Miami, Rome, and Vienna intraoperative iPTH assay criteria. Langenbecks Arch Surg. 2009.
Khan ZF, et al. Intraoperative Parathyroid Hormone Monitoring in the Surgical Management of Sporadic PHPT. Endocrinol Metab. 2019.
Quinn AJ, et al. Systematic review/meta-analysis of ioPTH in MIP. JAMA Otolaryngol Head Neck Surg. 2021.
Medas F, et al. Systematic review/meta-analysis of rapid ioPTH. Int J Surg. 2021.
Staibano P, et al. Network meta-analysis of diagnostic test accuracy. JAMA Otolaryngol Head Neck Surg. 2024/2025 indexing.
PHPT during pregnancy may have serious consequences to the mother and to the fetus:
If it remains unrecognized or untreated:
In up to 80% of patients, it is not recognized due to physiological changes during pregnancy that mask gestational PHPT, such as:
Hemodilution:
Related to intravascular fluid expansion
Hypoalbuminemia
Increased glomerular filtration rate:
Resulting in hypercalciuria
Transplacental transfer of calcium
Clinical presentation of PHPT durign pregnagncy may range from:
Hyperemesis, lethargy, hypertension, thirst, abdominal pain, depression, constipation, bone fracture, maternal heart rhythm disorders, maternal hypertension to preeclampsia, nephrolithiasis, pancreatitis, hyperemesis gravidarum, and hypercalcemic crisis:
Because the understanding of this concept and standard monitoring of all pregnant patients in developed countries:
The presentation of PHPT during pregnancy is very mild:
It is diagnosed in earlier stages
Sestamibi scan is contraindicated during pregnancy:
Due to radiation exposure risk to the fetus:
Ultrasound is the only diagnostic option since it carries no risk of radiation exposure and is easy to perform
Management of PHPT during pregnancy:
Should be individualized based on symptoms and severity of hypercalcemia:
Parathyroidectomy is indicated in symptomatic patients and patients with severe hypercalcemia:
When calcium level is elevated above 11 mg/dL (2.74 mmol/L)
Parathyroidectomy should be performed only in the second trimester:
To prevent miscarriage and anesthetic drugs exposure in the first trimester or spontaneous delivery in the third trimester
Mild form of PHPT causes low risk of maternal and obstetrical complications:
Therefore the patients can be managed conservatively, and parathyroidectomy can be deferred until after the delivery
Some medications, such as bisphosphonates, are contraindicated during pregnancy
Calcitonin:
Showed limited data and poor effectiveness:
But it does not cross the placenta and appears to be safe
Cinacalcet:
Has shown good results in several studies:
Although safety data are limited
Recent paper published by Rigg et al. retrospectively reviewed data of 28 pregnant patients with PHPT (22 managed medically and 6 surgically by elective parathyroidectomies):
Showed that 30% of those who were managed medically developed preeclampsia, and 66% managed medically had preterm deliveries
What was the primary research question of the INSEMA trial?
Answer:
To determine whether sentinel lymph node biopsy (SLNB) can be safely omitted in patients with clinically node-negative early-stage breast cancer undergoing breast-conserving surgery and whole breast radiation, without compromising invasive disease-free survival (iDFS)
What type of study was this, and how was it designed?
Answer:
It was a prospective, randomized, multicenter, non-inferiority trial conducted in Germany and Austria
Patients were randomized in a 4:1 ratio to no SLNB vs. SLNB
What were the eligibility criteria for patients to be included in the trial?
Answer:
Female patients
Clinically node-negative (cN0) invasive breast cancer
Tumor size cT1 to cT2 (≤ 5 cm)
Candidates for breast-conserving surgery and whole-breast irradiation
No prior axillary surgery, neoadjuvant therapy, or mastectomy
What was the primary endpoint, and what was the non-inferiority margin?
Answer:
Primary endpoint:
5-year invasive disease-free survival (iDFS)
Non-inferiority margin:
Hazard Ratio upper limit of 1.271 and ≥ 85% iDFS in the no-SLNB arm
What were the main results regarding iDFS
Answer:
iDFS: 91.9% (no-SLNB) vs. 91.7% (SLNB)
HR: 0.91 (95% CI, 0.73–1.14) → Non-inferiority was met
Was there a difference in overall survival (OS)
Answer:
Yes, but it favored no-SLNB slightly:
5-year OS: 98.2% (no-SLNB) vs. 96.9% (SLNB):
Difference was not statistically significant
What was the axillary recurrence rate in both groups?
Answer:
No-SLNB: 1.0%
SLNB: 0.3%
While slightly higher in the no-SLNB group:
Both rates were very low and clinically acceptable
What secondary outcomes were assessed?
Answer:
Lymphedema incidence
Arm / shoulder function and pain
Quality of life
All significantly favored the no-SLNB group
What are the main clinical implications of this study?
Answer:
In selected low-risk patients:
SLNB may be safely omitted:
Reducing surgical morbidity and improving quality of life without compromising survival
Which subgroup of patients benefits most from SLNB omission based on this trial?
Answer:
Women ≥ 50 years old with T1, grade 1 to grade 2, hormone receptor-positive, HER2-negative tumors undergoing lumpectomy with whole breast radiation
Can we apply the findings of this trial to patients undergoing mastectomy or partial-breast irradiation?
Answer:
No:
Those patients were excluded, so the results cannot be extrapolated to those scenarios
How might omitting SLNB affect adjuvant therapy decisions?
Answer:
Without nodal staging, decisions about chemotherapy or genomic testing might become more challenging:
Multidisciplinary evaluation is essential
How do these findings compare to axillary de-escalation trends seen in trials like ACOSOG Z0011 or SOUND?
Answer:
Similar direction:
All support less axillary surgery in low-risk, clinically node-negative patients
INSEMA takes it a step further by testing omission of SLNB itself
What are some limitations of the INSEMA trial
Answer:
Limited generalizability:
Mostly postmenopausal, low-risk tumors
Exclusion of higher-risk patients:
HER2+, triple-negative, T2 > 3 cm
Lack of data in mastectomy or neoadjuvant settings
If one of your patients meets criteria from this trial, how would you counsel them on omitting SLNB?
Answer:
Explain that in select low-risk early-stage breast cancer, omitting SLNB does not affect survival, reduces the risk of complications like lymphedema, and improves quality of life:
However, thorough discussion with oncology and radiation teams is important to individualize care