My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Is defined as persistent or newly identified locoregional or distant metastases on imaging:
Usually in conjunction with elevated thyroglobulin (Tg) and / or anti-thyroglobulin antibody (TgAb) levels
It is one of four response-to-therapy categories in the ATA dynamic risk stratification system:
Alongside excellent, indeterminate, and biochemical incomplete responses
Criteria by Treatment Context:
The definition of SIR is consistent regardless of surgical extent:
Structural evidence of disease confirmed by suspicious imaging or biopsy-proven local or distant metastatic disease
The TSH goal for patients with SIR:
Is maintained below the normal reference range
Prevalence and Outcomes:
SIR occurs in approximately 2.8% to 10% of DTC patients after initial therapy
In a cohort of 501 patients treated with total thyroidectomy and RAI:
2.8% had SIR at initial assessment:
By last follow-up, 10.2% had structurally incomplete responses
Key outcome data include:
Patients with an initial SIR:
Had an 83.9% rate of continued structural disease over long-term follow-up (mean 10.3 years)
All patients categorized as SIR after total thyroidectomy without RAI:
Experienced continued presence of disease
SIR requires multidisciplinary management tailored to disease status (regional vs. distant metastases, iodine-avid vs. non-iodine-avid disease)
Management:
Management of SIR depends on:
Disease location, RAI avidity, resectability, and rate of progression
Locoregional disease:
Surgery is preferred for resectable locoregional recurrence:
With formal compartmental dissection for previously undissected basins
RAI therapy:
If radioiodine imaging is positive
Active surveillance:
Is appropriate for non-progressive disease that is stable and distant from critical structures:
Small-volume lymph node recurrences often show little progression over years
Local therapies (ethanol ablation, RFA, cryoablation):
May be considered for limited-burden nodal disease
RAI-refractory or progressive disease:
Somatic molecular testing for actionable mutations (BRAF, RET, NTRK, ALK fusions; dMMR/MSI/TMB) is recommended for advanced, progressive, or threatening disease
Systemic therapy for progressive and/or symptomatic disease:
Lenvatinib (preferred; PFS 18.3 vs. 3.6 months, ORR 65%)
Sorafenib (PFS 10.8 vs. 5.8 months)
Cabozantinib after prior VEGFR TKI (PFS 11.0 vs. 1.9 months)
Targeted therapies:
Dabrafenib / trametinib (BRAF V600E)
Selpercatinib / pralsetinib (RET fusion)
Larotrectinib / entrectinib (NTRK fusion)
Pembrolizumab (MSI-H/dMMR or TMB-H)
Disease monitoring is often appropriate for asymptomatic patients with indolent, non-progressive disease and no brain metastases:
TKI therapy may not be appropriate for stable or slowly progressive disease
TSH suppression should be maintained with TSH
References:
2025 American Thyroid Association Management Guidelines for Adult Patients With Differentiated Thyroid Cancer. Ringel MD, Sosa JA, Baloch Z, et al. Thyroid : Official Journal of the American Thyroid Association. 2025;35(8):841-985. doi:10.1177/10507256251363120.
SNMMI Procedure Standard/Eanm Practice Guideline for Nuclear Medicine Evaluation and Therapy of Differentiated Thyroid Cancer: Abbreviated Version. Avram AM, Giovanella L, Greenspan B, et al. Journal of Nuclear Medicine : Official Publication, Society of Nuclear Medicine. 2022;63(6):15N-35N.
Thyroid Carcinoma. National Comprehensive Cancer Network. Updated 2025-03-27. Thyroid Cancer. Chen DW, Lang BHH, McLeod DSA, Newbold K, Haymart MR. Lancet (London, England). 2023;401(10387):1531-1544. doi:10.1016/S0140-6736(23)00020-X.
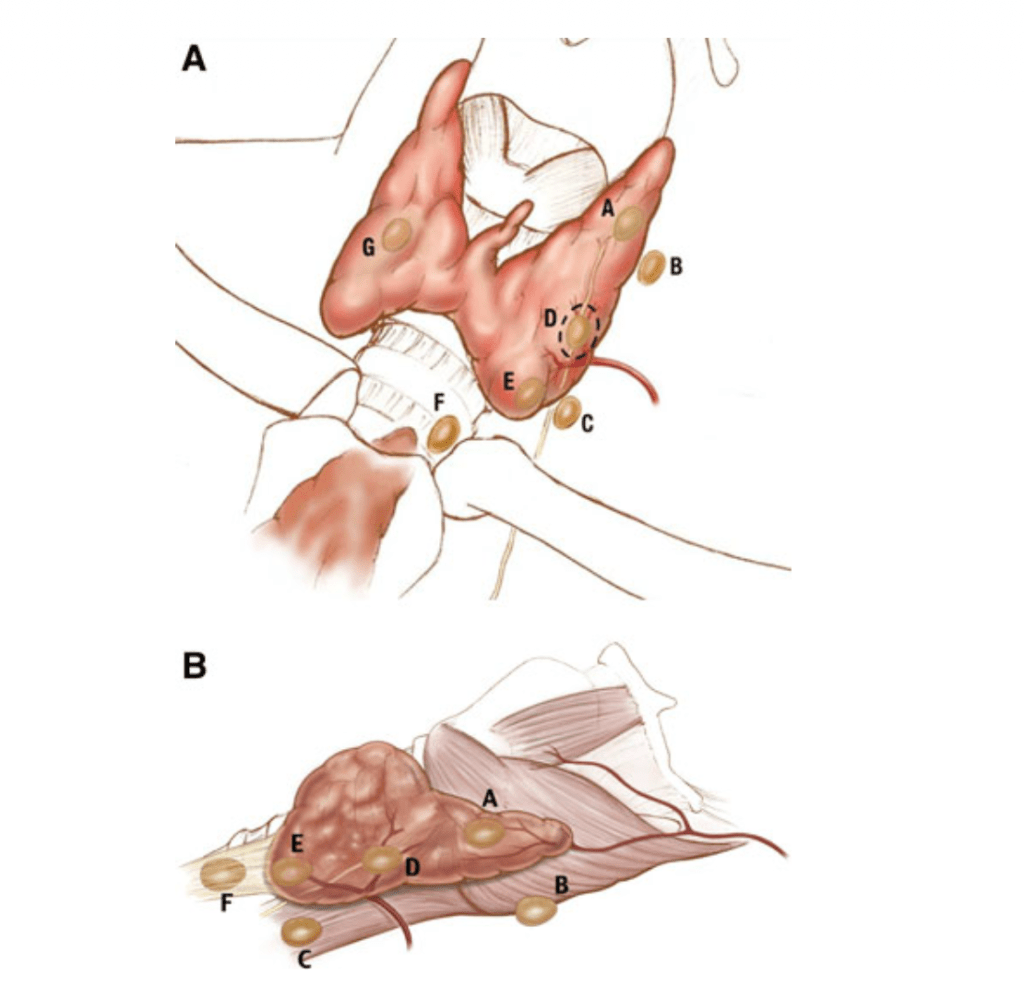
Type A glands are in the accepted, expected location of a normal parathyroid gland
Type B:
Behind the thyroid parenchyma
Type B glands are exophytic to the thyroid parenchyma and lie in the tracheoesophageal groove:
This category includes adenomas in:
Retroesophageal, retropharyngeal, high lateral pharyngeal, and carotid sheath locations
A ‘‘B+’’ subcategory can be used to document the location of adenomas above the level of the hyoid bone:
The ‘‘+’’ is meant to reflect cranial elevation
Type C:
Caudal to the thyroid parenchyma:
In the tracheoesophageal groove
A type C gland is more inferior than a type B gland on lateral images:
Located inferior to the inferior pole of the thyroid:
Closer to the clavicle
Type D:
Directly over the recurrent laryngeal nerve:
At the level of the inferior thyroid vessels
The dissection may be difficult:
Because a type D gland is dangerously close to the recurrent laryngeal nerve
Type E:
Located in the external aspect of the inferior pole of the thyroid
A type E gland is in a location that is:
More superficial in an anterior–posterior plane than the recurrent laryngeal nerve:
It is the easiest to resect
Type F:
‘‘Fallen’’ into the thyrothymic ligament:
Below the inferior pole of the thyroid in a pretracheal plane
A type F gland is frequently referred to as an ectopic gland:
Its resection usually involves:
Transcervical delivery of the thyrothymic ligament or superior portion of the thymus
Type G:
A gauge, true intrathyroidal gland location
Schematic representation of the nomenclature system for localization of parathyroid adenomas. Anterior view (a); right lateral view (b) of the superior thyroid pole is oriented to the left. The dotted circle depicts the region where the recurrent laryngeal nerve is most at risk
This nomenclature system has been designed that takes into account the pathologic position of the parathyroid glands (Figure):
Superior and inferior glands:
Are defined by the location of the gland’s pedicle and its relationship to the RLN:
Superior parathyroid glands:
Anatomically have a vascular pedicle superior and lateral to the RLN (type A through D glands)
Inferior parathyroid glands:
Anatomically have a vascular pedicle inferior and medial to the RLN (type D through F glands)
Type G glands:
Represent intrathyroidal parathyroid lesions
This information not only helps radiologists communicate potential parathyroid lesions of interest to surgeons:
But also helps surgeons direct their dissection in relation to the RLN
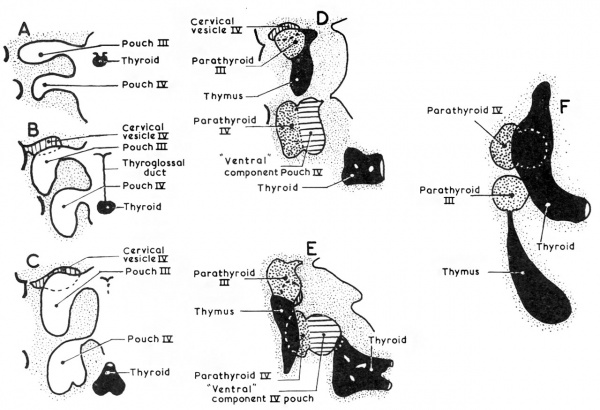
Develop as epithelial thickenings of the dorsal endoderm of the:
Third and fourth branchial pouches
The superior parathyroid glands:
Are derived from the fourth branchial pouch:
Which also gives rise to the ultimobranchial bodies:
The ventral aspect of these pouches is believed to fuse with the rudimentary fifth branchial pouches:
To from the ultimobranchial bodies
The superior parathyroid glands follow the migration of the ultimobranchial bodies:
Which descend a relative limited path toward the lateral thyroid region:
Ultimately giving rise to the parafollicular cells of the thyroid
The superior parathyroid glands separate from the ultimobranchial bodies:
As the median and lateral thyroid anlages fuse and incorporate the ultimobranchial bodies:
This separation event determines the final anatomic position of the superior parathyroid glands relative to the thyroid (Type A gland)
The inferior parathyroid glands:
Are derived from the third branchial pouch (dorsal aspect):
Along with the thymus (derived from the ventral aspect of the third branchial pouch)
The parathyroid glands:
Remain intimately connected with their respective branchial pouch derivatives
The normal anatomic location of the superior parathyroid glands:
Is more constant than the inferior parathyroid glands:
With 80% of the superior glands being found near the posterior aspect of the thyroid gland:
At the junction of the upper and middle portion of the thyroid lobes:
At the level of the cricoid cartilage:
Each gland with its own capsule of connective tissue:
Type A gland
Roughly one percent (1%) of the superior parathyroid glands:
May be found in the paraesophageal or retroesophageal space, retrolaryngeal space, high lateral pharyngeal, and carotid shealth locations:
Type B glands:
Behind the thyroid parenchyma:
Type B glands are exophytic to the thyroid parenchyma:
Lie in the tracheoesophageal groove
Type C glands:
Caudal to the thyroid parenchyma:
In the tracheoesophageal groove
A type C gland is more inferior than a type B gland on lateral images and located inferior to the inferior pole of the thyroid (closer to the clavicle)
Enlarged superior parathyroid glands:
May descend in the tracheoesophageal groove and come to lie below the inferior parathyroid glands (Type C gland)
Truly ectopic superior parathyroid glands:
Are extremely rare:
But may be localized to the middle or posterior mediastinum or in the aortopulmonary window
During intrauterine development:
The thymus and the inferior parathyroid glands:
Migrate caudally in the neck
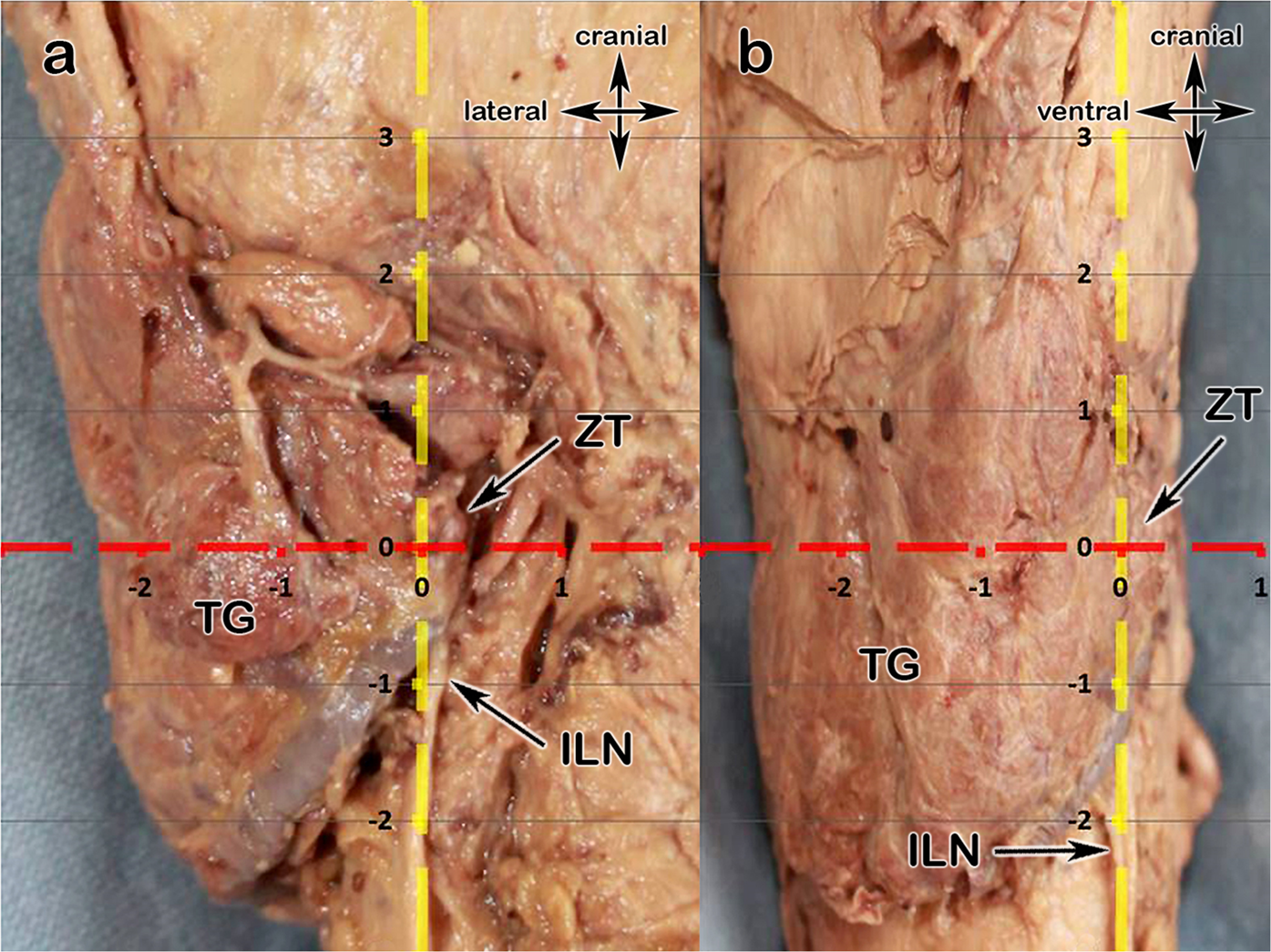
The most common location for the inferior parathyroid glands:
Is within 1 cm from a point centered where the inferior thyroid artery and the recurrent laryngeal nerve (RLN) cross
In roughly 50% of the cases:
The inferior parathyroid gland is located at the level of the inferior thyroid lobe:
Anterior of the posterolateral surface:
Type E:
Located in the external aspect of the inferior pole of the thyroid
A type E gland is in a location that is more superficial in an anterior-posterior plane than the recurrent laryngeal nerve
It is the easiest to resect
Approximately 15% to 50% of the inferior glands:
Are found in the thyrothymic ligament or the thymus
The inferior parathyroid gland is typically situated within a pocket of thymic derived fatty tissue:
But may be closely adherent to the thyroid capsule
The position of the inferior parathyroid glands:
However, tends to be more variable due to their longer migratory route:
Undescended inferior glands may be found near the:
Skull base, angle of the mandible, or above the superior parathyroid glands:
Along with an undescended thymus
The frequency of intrathyroidal glands:
Is approximately 2%
Superior parathyroid glands (4th branchial pouch):
Short migration
More constant location
Posterior to RLN, near cricothyroid joint
Inferior glands (3rd branchial pouch):
Long migration with thymus
Highly variable
Can be anywhere from angle of mandible → mediastinum
The classification is built on this predictable vs variable descent pattern
The Perrier Classification System
The authors propose categorizing adenomas based on their relationship to key anatomic landmarks, especially:
Thyroid gland
Recurrent laryngeal nerve (RLN)
Thymus
Carotid sheath
📍 Four Main Categories
Type A — Orthotopic (Normal Position)
Located in expected anatomical position
Adjacent to thyroid gland
Most common
👉 Clinical relevance:
Ideal for minimally invasive parathyroidectomy (MIP)
High concordance with sestamibi + ultrasound
Type B — Ectopic but Cervical
Includes:
Retroesophageal
Carotid sheath
Intrathyroidal
High cervical (undescended)
👉 Key point: Still in the neck but outside usual location
👉 Surgical implication:
May require focused but modified approach
Intrathyroidal → partial thyroid resection
Type C — Thymic / Thyrothymic
Along thymic descent pathway
Thyrothymic ligament
Within cervical thymus or upper mediastinum
👉 Most common ectopic site for inferior glands
👉 Surgical implication:
Cervical thymectomy often required
Important in failed initial exploration
Type D — Mediastinal
Below thoracic inlet
Aortopulmonary window, pericardium, deep thymus
👉 Rare but critical
👉 Surgical implication:
May require:
VATS
Sternotomy
Interventional radiology localization
📊 Key Findings from Perrier et al.
Majority of adenomas are Type A (orthotopic)
Ectopic locations (Types B to D) account for:
~15% to 20% of cases
Inferior glands → disproportionately represented in ectopic group
👉 The classification correlates strongly with:
Embryology
Preoperative imaging success
Surgical difficulty
🎯 Clinical Impact
1. Improves Communication
Standard language across:
Surgeons
Radiologists
Endocrinologists
2. Enhances Preoperative Planning
Predicts:
Likelihood of MIP vs BNE
Need for extended exploration
3. Reduces Failed Explorations
Particularly valuable in:
Reoperative cases
Discordant imaging
4. Facilitates Research Standardization
Enables:
Comparable outcome reporting
Better stratification in studies
🧠 Surgical Algorithm Integration
Imaging Result
Likely Type
Strategy
Concordant US + Sestamibi
Type A
Focused MIP
Discordant imaging
Type B / C
Extended cervical exploration
Negative imaging
Type C / D
Consider 4D-CT, PET, BNE
Prior failed surgery
Any (often B to D)
Systematic re-exploration
⚠️ Limitations of the Study
Retrospective classification
Single-institution experience (MD Anderson)
No direct comparison with alternative systems
Does not incorporate modern imaging (e.g., 4D-CT, PET)
📚 Key References
Perrier ND et al. World J Surg. 2009;33:412–416
Akerström G et al. Anatomy and embryology of parathyroid glands. World J Surg. 1984
Wang C. Parathyroid gland location study (645 cases). Ann Surg. 1976
You now need to identify patients who may benefit before finalizing adjuvant plan:
Candidates to flag early:
Stage II (even N0) with:
High grade
High Ki-67
Genomic high risk
Any Stage III HR+ disease
Impacts surgical-pathologic reporting priorities:
Surgeons should ensure:
Accurate nodal staging
Grade
Ki-67
Genomic assay (if used) integrated early
These directly influence eligibility for CDK4/6 therapy
Reinforces importance of recurrence biology:
Luminal cancers:
Long natural history
Late relapse risk
Ribociclib addresses micrometastatic dormancy → shifts mindset from: “Local control + endocrine therapy” → to “Extended systemic control strategy”
Treatment duration considerations:
Ribociclib:
3 years
Endocrine therapy:
≥ 5 years
Implication:
Long-term adherence planning begins at surgical consultation
Safety Profile (surgeon-relevant highlights):
Common:
Neutropenia (non-febrile)
LFT elevation
QT prolongation
No new long-term safety signals at 5 years
Clinical takeaway:
Manageable → supports use in early-stage curative setting
Key Takeaways for Surgical Practice:
Ribociclib is now a standard adjuvant option in HR+/HER2− EBC:
Especially stage II to III and biologically high-risk disease
5-year data confirms durability:
Benefit persists beyond treatment window:
Increasing absolute benefit over time
Expands eligible population:
Includes node-negative high-risk patients
Multidisciplinary coordination is critical:
Surgeons play a role in:
Early identification
Pathologic risk stratification
Timely referral to medical oncology
Bottom line (surgeon-focused):
Ribociclib from NATALEE represents a shift toward proactive systemic prevention of recurrence in luminal breast cancer, with durable 5-year benefit and broader eligibility than prior CDK4/6 strategies—making early risk identification at the surgical stage increasingly important
The Phase III LEAP-10 trial represents a major collaborative effort between Merck & Co. and Eisai, addressing a persistent unmet need in recurrent /metastatic head and neck squamous cell carcinoma (R/M HNSCC).
In patients with PD-L1 CPS ≥1 disease, the combination of lenvatinib + pembrolizumab demonstrated:
Improved objective response rate (ORR)
Prolonged progression-free survival (PFS)
However, these gains did not translate into an overall survival (OS) benefit compared with pembrolizumab monotherapy, which remains the backbone of first-line treatment.
Clinical Context: Why OS Remains Elusive
Despite encouraging activity, the absence of OS improvement reinforces the durability of the current standard established by KEYNOTE-048 trial, where:
Pembrolizumab ± chemotherapy continues as standard of care
Survival benefit is tightly linked to PD-L1 expression and patient selection
The LEAP-10 findings highlight a recurring challenge in HNSCC:
Early efficacy signals (ORR, PFS) do not reliably predict survival benefit, particularly in an immunotherapy-sensitive disease where post-progression treatments and tumor biology heavily influence OS.
Biologic Interpretation
The addition of lenvatinib, a multi-kinase inhibitor targeting VEGFR, FGFR, and others, likely:
Enhances tumor microenvironment modulation
Improves initial tumor shrinkage and disease control
However, potential limitations include:
Lack of deep, durable immune reprogramming
Emergence of resistance mechanisms
Possible toxicity-related treatment discontinuation
These factors may blunt long-term survival impact despite improved early endpoints.
Where the Field Is Heading: EGFR and Beyond
Attention is now shifting toward next-generation EGFR-targeted strategies, with the hypothesis that:
More precise targeting of EGFR-driven signaling
Coupled with immune engagement mechanisms
may yield more durable survival benefits.
Key players advancing this space include:
Dana-Farber Cancer Institute
Genmab
Bicara Therapeutics
Johnson & Johnson
Merus N.V.
Harvard Medical School
Emerging modalities include:
Bispecific antibodies (EGFR × immune targets)
Antibody-drug conjugates (ADCs)
Combination immunotherapy strategies
These approaches aim to:
Overcome primary and acquired resistance
Deliver more sustained immune activation
Ultimately shift the OS curve, not just early endpoints
Key Takeaway for Clinical Practice
While lenvatinib + pembrolizumab shows meaningful biologic and clinical activity, it does not currently challenge pembrolizumab-based regimens as standard of care in PD-L1–positive R/M HNSCC.
The central question remains:
What therapeutic strategy will meaningfully and reproducibly improve overall survival in first-line HNSCC?
The next wave of EGFR-targeted and immune-engaging therapies may be the most promising path forward.
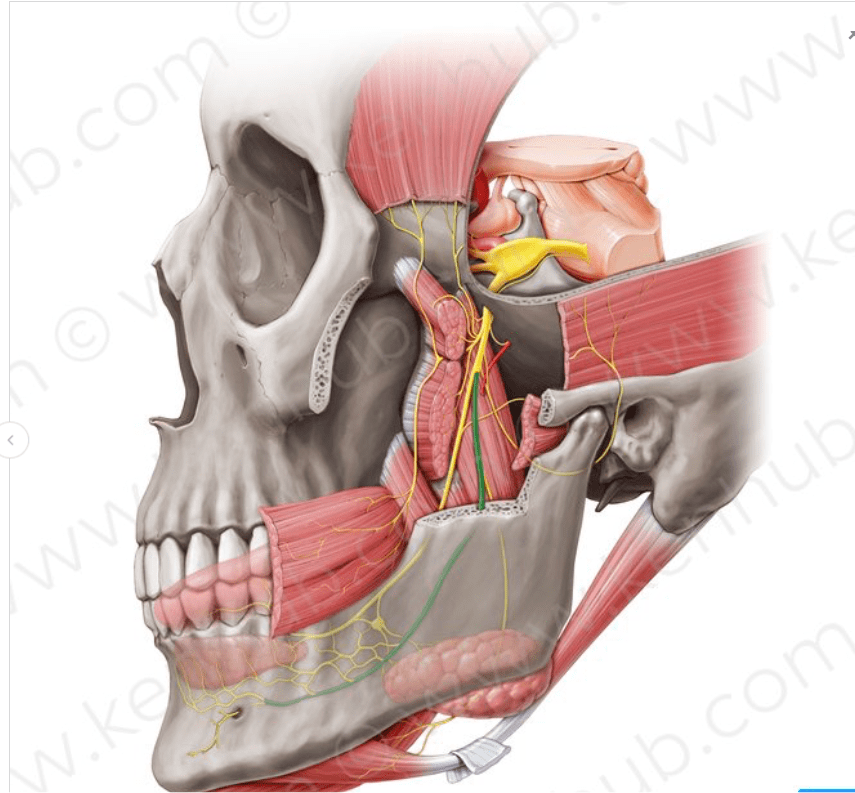
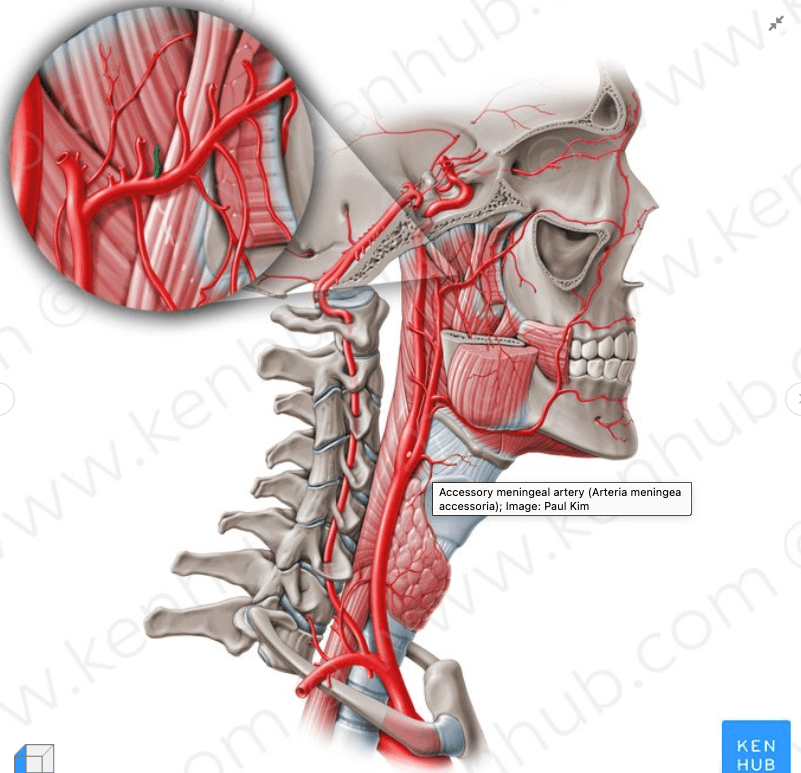
The maxillary artery supplies deep structures of the face.
It branches from the external carotid artery just deep to the neck of the mandible.
Structure:
The maxillary artery, the larger of the two terminal branches of the external carotid artery:
Arises behind the neck of the mandible, and is at first imbedded in the substance of the parotid gland.
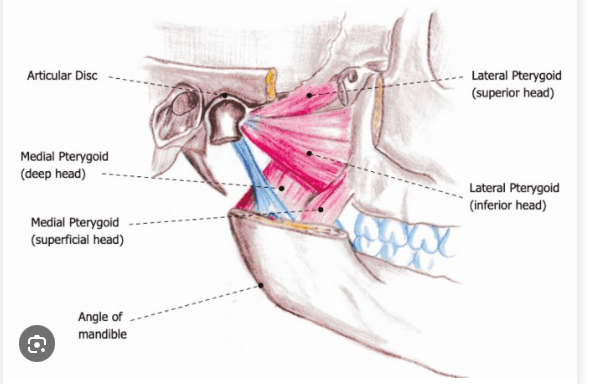
It passes forward between the ramus of the mandible and the sphenomandibular ligament, and then runs, either superficial or deep to the lateral pterygoid muscle, to the pterygopalatine fossa.
It supplies the deep structures of the face.
May be divided into:
Mandibular portion (first part / bony part)
Pterygoid portion (second part / muscular part)
Pterygopalatine portions (third part).
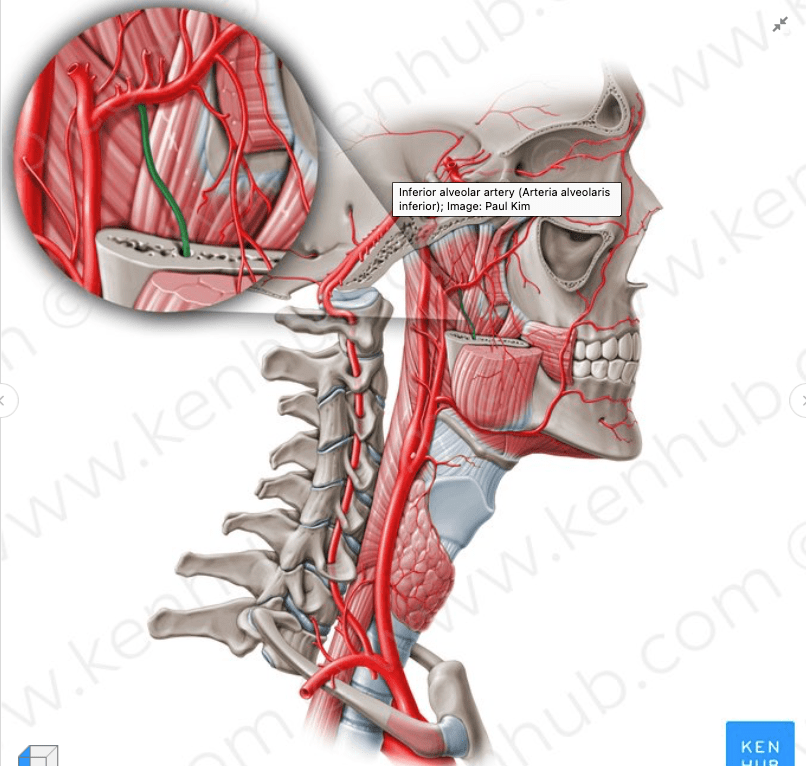
Mandibular portion (first part / bony part):
The first or mandibular portion (or bony portion) passes horizontally forward, between the neck of the mandible and the sphenomandibular ligament:
Where it lies parallel to and a little below the auriculotemporal nerve.
It crosses the inferior alveolar nerve, and runs along the lower border of the lateral pterygoid muscle.
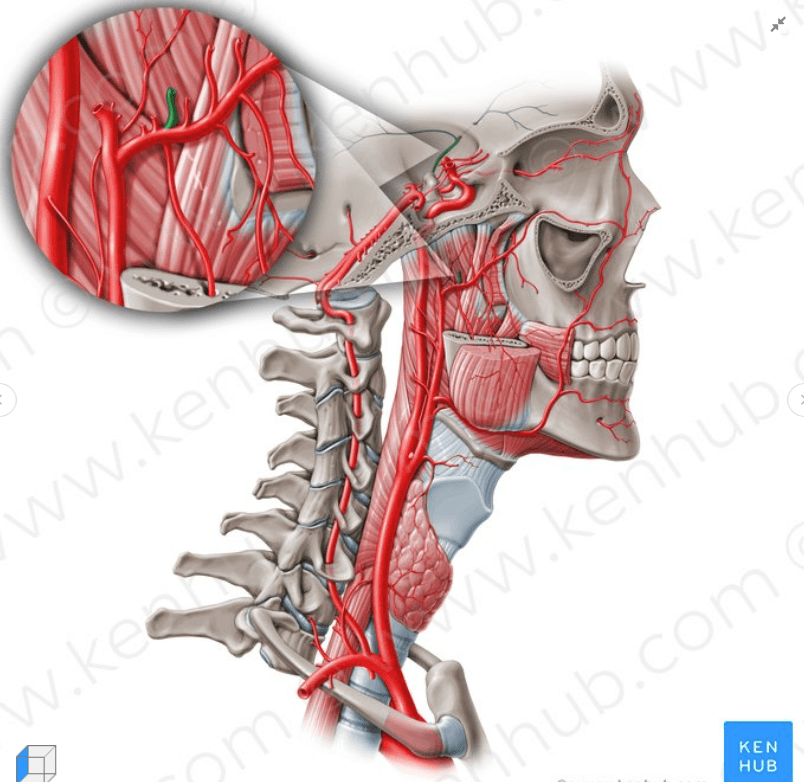
Branches include:
Deep auricular artery
Anterior tympanic artery
Middle meningeal artery
Inferior alveolar artery:
Which gives off its mylohyoid branch just prior to entering the mandibular foramen
Accessory meningeal artery
Pterygoid portion (second part / muscular part):
The second or pterygoid portion (or muscular portion) runs obliquely forward and upward under cover of the ramus of the mandible and insertion of the temporalis muscle:
On the superficial (very infrequently on the deep) surface of the lateral pterygoid muscle.
It then passes between the two heads of origin of this muscle and enters the fossa.
Branches include:
Masseteric artery
Pterygoid branches
Deep temporal arteries:
Anterior and posterior
Buccal (buccinator) artery
Pterygopalatine portions (third part):
The third or pterygopalatine portion lies in the pterygopalatine fossa in relation with the pterygopalatine ganglion.
This is considered the terminal branch of the maxillary artery.
Branches include:
Sphenopalatine artery:
Nasopalatine artery is the terminal branch of the maxillary artery
Descending palatine artery:
Greater palatine artery
Lesser palatine artery
Infraorbital artery
Posterior superior alveolar artery
Artery of pterygoid canal
Pharyngeal artery
Middle superior alveolar artery (could be a branch of the infraorbital artery)
Anterior superior alveolar arteries (could be a branch of the infraorbital artery)
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon at the Braman Comprehensive Cancer Center at Mount Sinai Medical Center in Miami, Florida.
He is first author on some publications on oral cavity cancer:
Oral Tongue Cancer: Literature Review and Current Management
The proximity or direct extension of a primary tumor of the oral cavity to the mandible requires appropriate radiological studies to establish the presence and extent of bone involvement:
Although the absence of radiographic findings does not rule out bone invasion:
Bone destruction as seen on the radiograph confirms tumor invasion
Radionuclide bone scans:
Often are positive before the radiographic appearance of bone destruction:
But they seldom provide accurate information regarding the extent of bone invasion
Bone scans also may be positive in non-neoplastic conditions:
Such as inflammatory lesions
Plain radiographs of the mandible in the antero-posterior and oblique views:
Are not satisfactory as a routine screening test to establish or rule out bone destruction
A panoramic view of the mandible (an orthopantomogram):
Is helpful to assess the general architecture of the mandible in relation to the dento-alveolar structures and invasion by the tumor (Figure)
However, for technical reasons:
The midline of the mandible near the symphysis is not adequately evaluated by a panoramic view
In addition, early invasion of the lingual cortex of the mandible is not seen on a panoramic view
Occlusal films of the body of the mandible and intraoral dental films:
Often are most accurate in demonstrating early invasion by a tumor
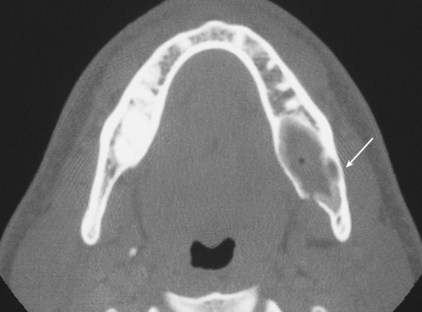
CT scans of the mandible:
Generally are not optimal for routine screening:
But may be considered in certain circumstances:
Such as primary tumors of the mandible and lesions where soft tissue extension from tumors involving the ascending ramus of the mandible is suspected (Figure)
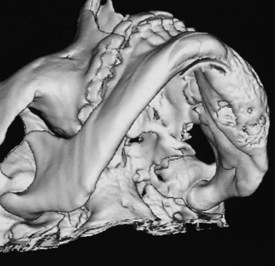
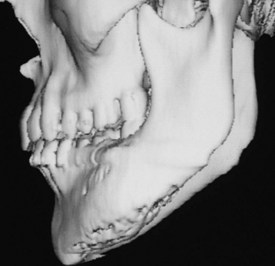
Three-dimensional reconstructions of CT images provide an excellent overview of the mandible or maxilla from any desired angle
A computerized tomogram of the oral cavity and neck:
Is the standard initial radiographic study for assessment of locoregional extent of the tumor
It allows comprehensive evaluation of neck nodes and also the relationship of the primary tumor to adjoining bone:
Especially in situations such as primary tumors of the mandible and lesions where soft-tissue extension from tumors involving the ascending ramus of the mandible is suspected
Three-dimensional reconstructions of the mandible of a patient with an ossifying fibroma of the body of the mandible on the left-hand side causing expansion and involving the lingual cortex are shown in the Figures
A three-dimensional CT scan and a one-to-one reproduction of the CT scan:
Are of great value to the surgeon for mandible reconstruction with a microvascular free flap
The decision to extend a supraomohyoid neck dissection (levels I to III) to include level IV (extended supraomohyoid neck dissection):
Hinges on whether pN+ disease is discovered in levels I to III, the number of positive nodes, and the pN classification
Below is a comprehensive review of the specific scenarios and supporting data
Scenario 1 – cN0 Neck → Intraoperative Discovery of pN+ Disease in Levels I to III:
This is the most clinically relevant scenario
When a patient undergoes END for a cN0 neck and positive nodes are found on frozen section or final pathology:
The risk of concurrent level IV to V disease rises substantially compared to the overall cN0 population
The Haas et al. (2025) study directly addressed this question in 61 cN0 patients who were found to be pN+ in levels I to III [1]:
9.8% (6/61) had metastases in levels IV to V:
Well above the 5% threshold generally used to justify elective dissection
> 1 positive node in levels I to III was the strongest predictor of level IV to V involvement (p = 0.027)
pN classification > pN2b significantly increased the prevalence of level IV to V metastases (p = 0.002)
Extracapsular spread (ECS) showed a trend toward increased IV to V involvement (p = 0.078), though not statistically significant in this cohort
This 9.8% rate stands in stark contrast to the 0.50% true skip metastasis rate in the overall cN0 population, underscoring that the discovery of pN+ disease in levels I to III fundamentally changes the risk calculus
Scenario 2 – cN+ Neck (Preoperatively Known Nodal Disease):
For the clinically node-positive neck, both ASCO and NCCN guidelines explicitly recommend including level IV in the dissection [2][3]
The ASCO guideline states:
An ipsilateral therapeutic selective neck dissection for a cN+ neck should include:
Nodal levels Ia, Ib, IIa, IIb, III, and IV with ≥ 18 lymph nodes (evidence-based, intermediate quality, moderate strength) [2]
The NCCN guidelines specify:
cN1 to cN2a–c disease warrants selective or comprehensive neck dissection [3]
The American Head and Neck Society review provides the supporting data:
Occult level IV nodal metastatic disease is reported in 11.1% to 23.7% of cN+ oral tongue cancers, and 15% of all patients undergoing therapeutic neck dissection had level IV metastases [4]:
This rate is high enough that level IV dissection should be considered even in the absence of overt metastatic lymph node involvement at that level [4]
Scenario 3 – When to Add Level V:
Level V dissection carries significant risk to the spinal accessory nerve and is not routinely recommended
However, the data support its inclusion in specific circumstances [4]:
Clinical involvement of levels I to IV:
Was associated with occult metastases in level V in 27% of oral cavity SCCs in one study
Level V should be considered in patients with bulky, multilevel nodal disease
The overall rate of level V metastasis:
In therapeutic neck dissections is only ~4%
Practical Decision Framework – When to Extend to Level IV:
Prognostic Implications of Level IV Disease:
Importantly, the discovery of level IV or V disease is not merely an anatomic finding:
It carries significant prognostic weight
The NCCN guidelines list nodal disease in levels IV or V as an adverse pathologic feature:
Which triggers consideration of adjuvant systemic therapy / RT [3]
A SEER-based study of 8,281 patients:
Found that 5-year disease-specific survival dropped from 42.0% for level I to III disease to 30.6% for level IV [5]
Furthermore, level IV to V metastasis:
Is an independent risk factor for distant metastasis on multivariate analysis [6]
Morbidity Considerations:
Extension to level IV is not without cost
The American Head and Neck Society review notes that dissection of level IV:
Is associated with a low but possible risk of injury to the phrenic nerve or brachial plexus and increases the risk of chylous fistula [4]:
These risks must be weighed against the oncologic benefit, particularly in the cN0 setting where the absolute risk of level IV disease is low
Summary:
For the cN0 neck with no intraoperative evidence of nodal disease:
Levels I to III remain the standard
However, when intraoperative frozen section or final pathology reveals pN+ disease:
Particularly > 1 positive node or pN > pN2b:
The risk of level IV to V involvement rises to ~10%:
Justifying extension to level IV [1]
For any preoperatively cN+ neck:
Level IV should be included as standard practice per ASCO and NCCN guidelines [2][3]
Level V should be reserved for:
Multilevel, bulky nodal disease
References:
1. In Vivo Probability of Metastases in Levels IV-V in Oral Squamous Cell Carcinoma With a cN0/pN+ Situation in Levels I-Iii. Haas L, Mischkowski RA, Knape U, Król KM, Sakkas A. In Vivo (Athens, Greece). 2025 Nov-Dec;39(6):3437-3444. doi:10.21873/invivo.14141.
2. Management of the Neck in Squamous Cell Carcinoma of the Oral Cavity and Oropharynx: ASCO Clinical Practice Guideline. Koyfman SA, Ismaila N, Crook D, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2019;37(20):1753-1774. doi:10.1200/JCO.18.01921.
3. Head and Neck Cancers. National Comprehensive Cancer Network. Updated 2025-12-08.
4. Oral Cavity Cancer Surgical and Nodal Management: A Review From the American Head and Neck Society. Eskander A, Dziegielewski PT, Patel MR, et al. JAMA Otolaryngology– Head & Neck Surgery. 2024;150(2):172-178. doi:10.1001/jamaoto.2023.4049.
5. Impact of Nodal Level Distribution on Survival in Oral Cavity Squamous Cell Carcinoma: A Population-Based Study. Marchiano E, Patel TD, Eloy JA, Baredes S, Park RC. Otolaryngology–Head and Neck Surgery : Official Journal of American Academy of Otolaryngology-Head and Neck Surgery. 2016;155(1):99-105. doi:10.1177/0194599816636356.
6. Risk Factors for Distant Metastasis in Locoregionally Controlled Oral Squamous Cell Carcinoma: A Retrospective Study. Tomioka H, Yamagata Y, Oikawa Y, et al. Scientific Reports. 2021;11(1):5213. doi:10.1038/s41598-021-84704-w.
Remains one of the most powerful and actionable prognostic factors in oral tongue / oral cavity SCC
Classically, Scholl and colleagues:
Reviewed 268 patients with squamous carcinoma of the oral tongue:
They found that 54 (20.1%) had microscopic “cut-through” at the intraoperative frozen section margin:
An initially positive margin
Even when additional resection converted these to final negative margins:
Local control remained significantly worse:
Than in patients whose margins were clear on the first pass
They also reported that margin involvement patternsdiffered by T stage:
T1 to T2 tumors:
More often had positive mucosal margins
T3 to T4 tumors:
Commonly failed at the deep / soft-tissue margins
Similar observations were made in classic series evaluating “positive” epidermoid carcinoma margins in the head and neck:
Looser, Shah, and Strong:
Demonstrated that patients with involved margins:
Had substantially higher local recurrence than those with negative margins:
With early reports quoting local recurrence in roughly two-thirds to three-quarters of patients with positive margins versus about one-third with negative margins
Loree and Strong:
Subsequently examined 398 oral cavity SCCs:
Showing that positive or “close” margins (tumor at or within 0.5 mm of the inked edge, or significant premalignant change / in situ carcinoma at the margin):
Were associated with a doubling of local recurrence (36% vs 18%) and inferior 5-year survival compared with negative margins (52% vs 60%)
The reliability and utility of intraoperative frozen section (FS) margin assessment have also been extensively studied:
Spiro et al:
Reported an overall intraoperative FS diagnostic accuracy of approximately 89% for oral tongue cancer:
Importantly found that accuracy was similar whether sections were taken directly from the patient’s tumor bed or from the oriented surgical specimen
Positive or “close” margins:
Defined in their series as tumor present at the ink or within roughly one high-power field of the resection edge:
Were associated with a significantly increased risk of local recurrence (p < 0.003)
Subsequent work by Byers and others:
Confirmed the prognostic and therapeutic value of frozen section (FS):
Guided re-resection in HNSCC:
But also highlighted that FS cannot fully compensate for suboptimal initial resection planes
Definitions of margin status and distance:
There is now better consensus on margin nomenclature
Most contemporary series and guidelines define:
Positive margin:
Invasive carcinoma or severe / high-grade dysplasia:
At the inked edge, or < 1 mm from the inked edge
Close margin:
Invasive carcinoma typically 1 to 4 or 1 to 5 mm from the inked edge:
Cut-off values vary:
But a 5 mm microscopic threshold is most commonly used in oral cavity SCC
Clear margin:
≥ 5 mm from invasive tumor to the inked edge after formalin fixation
Tasche et al., in a large JAMA Otolaryngology analysis:
Proposed that a distance < 1 mm behaves biologically like an involved margin:
With similarly high local recurrence risk
Whereas 1 to 5 mm margins had intermediate risk and ≥ 5 mm margins were associated with the lowest recurrence
More recent multicenter work emphasizes the importance of deep margin distance in particular:
With data suggesting that deep margins ≤ 3 mm carry a significantly higher risk of local failure compared with > 3 mm:
Even when the mucosal margin is wide
Impact of positive and close margins on outcomes:
Multiple retrospective series and meta-analyses now support and refine the early observations of Scholl, Looser, Loree, and Strong:
Positive final margins are consistently associated with:
~ 2-fold higher risk of local recurrence, increased regional / distant failure in some series, and significantly worse disease-specific and overall survival
Binahmed et al. and McMahon et al:
Both showed that patients with involved margins:
Had roughly double the local recurrence and significantly poorer survival compared with those with clear margins, and that close margins behaved intermediately between clearly negative and frankly positive margins
Liao et al:
Identified margin status, together with T stage, DOI, and perineural invasion:
As major predictors of local tumor control in oral cavity SCC
A 2019 systematic review and meta-analysis by Gorphe:
Concluded that positive margins carry an approximately two-fold increased risk of death and local failure across head and neck sites, independent of other factors
More granular contemporary analyses, including Buchakjian et al. and Szewczyk et al., have shown that:
Close margins (1 to 4.9 mm) often do not independently worsen outcomes if other adverse factors (lymphovascular invasion, perineural invasion, ENE, nodal disease, advanced T stage):
Are absent and if appropriate adjuvant therapy is given when indicated
The prognostic effect of close margins is modulated by:
Depth of invasion, pattern of invasion, and composite histologic risk models (e.g., Brandwein-Gensler)
Subsite-specific studies have further refined this:
Tongue and floor-of-mouth tumors are particularly prone to failure at the deep margin:
In several series, deep margin positivity or ≤ 2 to 3 mm clearance:
Has been more predictive of local recurrence than mucosal margin distance
Microscopic cut-through and “revised” margins:
Building on Scholl’s original work, the concept of microscopic tumor cut-through (MTCT):
A positive FS margin that is revised to negative on final pathology, has been extensively studied
Patel et al. (Head & Neck 2010) showed that MTCT:
Was associated with significantly worse local control and disease-specific survival compared with margins that were negative from the outset:
Particularly in patients with nodal disease
Guillemaud et al. similarly reported that intraoperative cut-through, even if revised to R0:
Predicted higher local recurrence and worse outcomes in oral cavity SCC
A meta-analysis by Bulbul et al. concluded that clearance of a positive margin improves outcomes relative to leaving it unrevised:
But patients with MTCT still fare worse than those whose margins were always negative:
Suggesting MTCT is a marker of more aggressive biology and / or challenging local anatomy
More recently, Agne et al. evaluated T3 to T4 OCSCC and confirmed that MTCT:
remained an independent predictor of local recurrence on multivariable analysis (HR ~1.8–2.2 for local failure):
Although its effect on disease-specific survival attenuated when controlling for nodal stage and other high-risk features
These data support considering MTCT as a high-risk feature warranting discussion of treatment intensification:
For example (e.g., adjuvant chemoradiotherapy) in a multidisciplinary tumor board, even when final margins are technically negative
Kwok et al. addressed the related question of “clear versus revised margins” in 417 patients with oral and pharyngeal carcinoma:
Patients who required immediate re-resection for a positive FS margin but ended with R0 status:
Had survival similar to those with primary R0 resection, and both groups did substantially better than patients left with residual microscopic or macroscopic disease
This suggests that while MTCT carries biologic risk:
An aggressive intraoperative strategy to convert to R0 is still beneficial and should remain standard practice
Intraoperative margin assessment:
Specimen vs tumor bed:
There is growing recognition that how margins are sampled:
Is almost as important as the final measurement
Meier et al.’s AHNS survey and several subsequent series have documented wide variation in intraoperative margin practices (tumor bed vs specimen mapping, number of samples, definition of “adequate” clearance), and a substantial rate of FS–permanent section discrepancy
Key contemporary points include:
Specimen-based mapping (oriented and inked, with communication between surgeon and pathologist):
Tends to provide more reliable correlation between FS and final margins than random tumor-bed biopsies
FS accuracy remains high (often ~ 85% to 95%):
But false-negatives and false-positives still occur:
Particularly at the deep margin, in previously irradiated fields, and in specimens with significant shrinkage
In some series, “complete FS margins” with a measurable 1 to 5 mm histologic buffer were associated with improved local control compared with conventional limited sampling
Recent reviews and consensus statements (e.g., Kubik et al., Kain et al., Chen et al. 2024) now recommend:
A planned 1 to 1.5 cm gross resection margin in vivo for oral tongue SCC, anticipating ~30% to 50% shrinkage with formalin fixation and tissue relaxation
Routine use of oriented, inked specimens with targeted FS from high-risk areas (deep margin, close relationship to muscle bundles or neurovascular structures)
Consideration of advanced adjuncts—near-infrared fluorescence mapping, specimen 3D-mapping, and emerging augmented-reality registration—for difficult tongue and floor-of-mouth resections
Integration with histologic risk models:
Finally, margin status must be interpreted in the context of overall histologic risk
The Brandwein-Gensler model:
Worst pattern of invasion, perineural invasion, lymphocytic host response and later refinements:
Have shown that high-risk tumors have markedly increased recurrence and disease-specific mortality even when margins are clear
Conversely, some low-risk early-stage tumors with close (but not involved) margins may do well without aggressive adjuvant therapy
This supports a nuanced, risk-adapted approach in which:
Positive margins or MTCT → strong indication for adjuvant chemoradiotherapy in most patients
Close margins (1 to 4 mm) → individualized decision based on DOI, nodal status, PNI/LVI, pattern of invasion, and patient-specific factors
Clear margins (≥ 5 mm) → lowest risk group, managed according to other adverse features.
Reviewed:
Scholl P, Byers RM, Batsakis JG, Wolf P, Santini H. Microscopic cut-through of cancer in the surgical treatment of squamous carcinoma of the tongue: prognostic and therapeutic implications. Am J Surg. 1986;152:354-360.
Looser KG, Shah JP, Strong EW. The significance of “positive” margins in surgically resected epidermoid carcinomas. Head Neck Surg. 1978;1:107-111.
Loree TR, Strong EW. Significance of positive margins in oral cavity squamous carcinoma. Am J Surg. 1990;160:410-414.
Spiro RH, Guillamondegui O, Paulino AF, et al. Pattern of invasion and margin assessment in patients with oral tongue cancer. Head Neck. 1999;21:408-413.
Chen TY, Emrich LJ, Driscoll DL. The clinical significance of pathological findings in surgically resected margins of the primary tumor in head and neck carcinoma. Int J Radiat Oncol Biol Phys. 1987;13:833-837.
McMahon J, O’Brien CJ, Pathak I, et al. Influence of condition of surgical margins on local recurrence and disease-specific survival in oral and oropharyngeal cancer. Br J Oral Maxillofac Surg. 2003;41:224-231.
Binahmed A, Nason RW, Abdoh AA. The clinical significance of the positive surgical margin in oral cancer. Oral Oncol. 2007;43:780-784.
Liao CT, Chang JTC, Wang HM, et al. Analysis of risk factors of predictive local tumor control in oral cavity cancer. Ann Surg Oncol. 2008;15:915-922.
Patel RS, Goldstein DP, Guillemaud J, et al. Impact of positive frozen section microscopic tumor cut-through revised to negative on oral carcinoma control and survival rates. Head Neck. 2010;32:1444-1451.
Guillemaud J, Patel RS, Goldstein DP, et al. Prognostic impact of intraoperative microscopic cut-through on frozen section in oral cavity squamous cell carcinoma. J Otolaryngol Head Neck Surg. 2010;39:370-377.
Kwok P, Gleich O, Hübner G, Strutz J. Prognostic importance of “clear versus revised margins” in oral and pharyngeal cancer. Head Neck. 2010;32:1479-1484.
Gorphe P. A systematic review and meta-analysis of margins in head and neck cancer. Oral Oncol. 2019;95:93-101.
Tasche KK, Buchakjian MR, Pagedar NA, Sperry SM. Definition of “close margin” in oral cancer surgery and association of margin distance with local recurrence rate. JAMA Otolaryngol Head Neck Surg. 2017;143:1166-1172.
Buchakjian MR, Tasche KK, Robinson RA, et al. Association of main specimen and tumor bed margin status with local recurrence and survival in oral cancer surgery. JAMA Otolaryngol Head Neck Surg. 2016;142:1191-1198.
Kain JJ, Birkeland AC, Udayakumar N, et al. Surgical margins in oral cavity squamous cell carcinoma: current practices and future directions. Laryngoscope. 2020;130:128-138. Szewczyk M, et al. A matter of margins in oral cancer—how close is enough? Cancers (Basel). 2024;16(8):1488.
Agne GR, et al. Oncologic outcomes of microscopic tumor cut-through in locally advanced oral squamous cell carcinoma. Arch Head Neck Surg. 2022;51:e20220013. Chen Y, et al. Surgical margins in head and neck squamous cell carcinoma. Int J Surg. 2024;109:54-66.
Brandwein-Gensler M, et al. Oral squamous cell carcinoma: histologic risk assessment, but not margin status, is strongly predictive of local disease-free and overall survival. Am J Surg Pathol. 2005;29:167-178.