My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
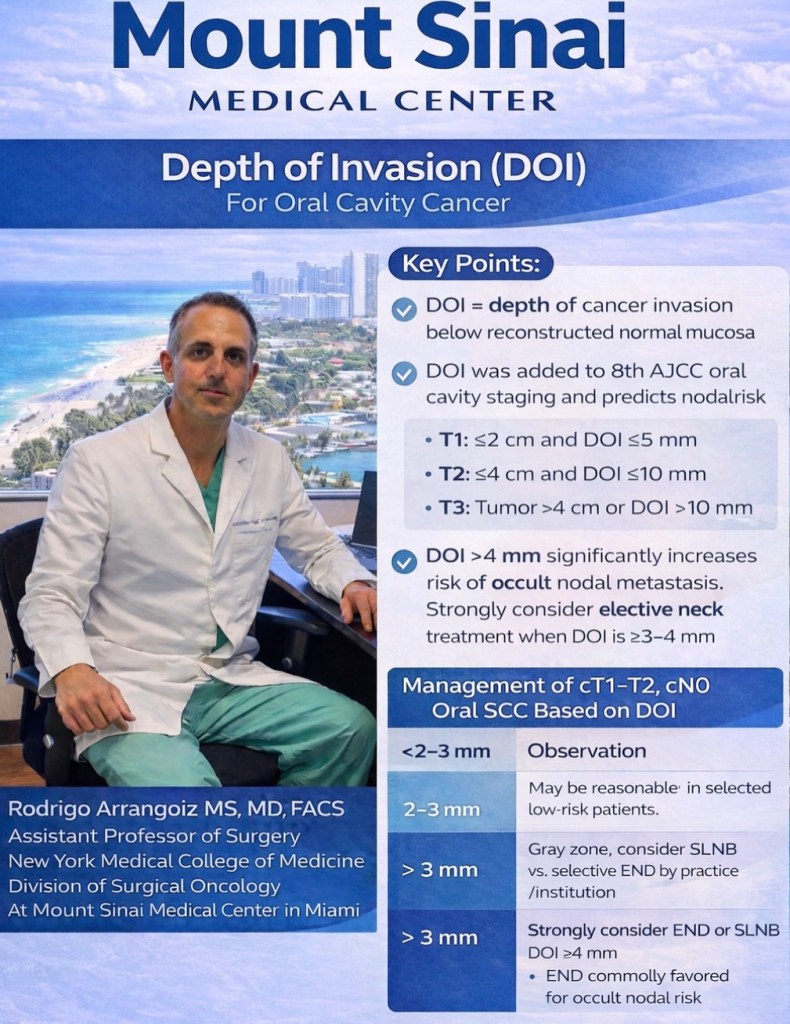
The 2025 ATA guidelines (Recommendation 11) formally endorse active surveillance (AS) as an acceptable management option for cT1aN0M0 papillary thyroid cancers (≤1 cm), graded as a conditional recommendation with low certainty evidence.
For recurrent / persistent nodal disease, the guidelines state that stable disease can continue monitoring, while bulky and / or invasive recurrent disease is generally best treated with surgery.
Recommendation 14 specifies that surgical resection is indicated when there is tumor growth ≥ 3 mm, new biopsy-proven lymph node metastases, distant metastases, extrathyroidal extension, or patient preference.
The NCCN Thyroid Carcinoma Guidelines (v1.2026) similarly note that AS is supported by low-quality evidence for papillary thyroid microcarcinoma ≤ 1 cm, with limited data for cancers >1 cm.
Quantitative Data on Progression During Active Surveillance
A 2026 systematic review and meta-analysis (10 studies, n = 841) provides the most comprehensive pooled data. The overall pooled progression rate during AS was 23% (95% CI, 12–34%), rising to 32% in biopsy-confirmed cases. Critically, after adjustment for follow-up loss, the estimated progression rate increased to 35% to 70%, suggesting that reported rates may substantially underestimate true progression. Subgroup analyses showed higher progression in patients with elevated baseline thyroglobulin (log-transformed Tg: 1.02 in progressors vs. −0.07 in stable, p < 0.05) and in those with advanced stage (≥ 5% Stage IV patients: 28% vs. 14%, p < 0.05).
Individual cohort studies provide additional granularity:
Jerkovich et al. (2022): 50 patients with cytology-confirmed metastatic lymph nodes (mean size 10.1 mm) under AS; 24% had lymph node growth at median 29 months. The only predictor of growth was a Tg rise ≥0.5 ng/mL (OR 16.2, p = 0.020). Median progression-free survival was 6.6 years. Among the 7 patients who underwent surgery after progression, none had structural incomplete response at follow-up.
Walter et al. (2023): 40 patients with metastatic cervical lymph nodes ≤2 cm; 35% progressed (17.5% enlargement ≥3 mm, 17.5% new metastasis) at median 27.5 months. Of 14 who progressed, 6 remained on AS with 5/6 showing no further progression.
Tufano et al. (2015): Lateral neck lymph nodes with suspicious ultrasonographic features demonstrated a low potential for structural progression—over a median of 3.5 years, only 9% increased by more than 5 mm.
Size Thresholds: Confirmed
The ATA-endorsed size thresholds for FNA biopsy consideration (and by extension, the boundary for observation) are ≥8 mm in the central compartment and ≥10 mm in the lateral compartment. The NCCN guidelines do not specify exact size cutoffs for AS of recurrent nodes but recommend “disease monitoring for non-progressive disease that is stable and distant from critical structures”.
Thyroglobulin Doubling Time as a Prognostic Marker
A Tg doubling time (Tg-DT) <1 year portends poor prognosis, while Tg-DT >2 years signifies good prognosis. The AHNS consensus statement recommends cross-sectional imaging at 4 to 6 month intervals when Tg-DT is <1 year, with longer intervals for longer doubling times.
A study by Albano et al. demonstrated that a TgDT threshold of ≤2.5 years predicted positive FDG-PET/CT results with 93% sensitivity and 87% specificity (AUC = 0.911), outperforming absolute Tg level alone. Ito et al. (2025) showed that combining unstimulated Tg ≥3 ng/mL with a Tg doubling rate ≥0.33/year identified the highest-risk group for both lymph node and distant recurrence.
FDG-PET Avidity: Strong Prognostic Data
FDG-PET avidity is a well-established marker of aggressive biology. Robbins et al. demonstrated that a positive FDG-PET/CT predicted a 7-fold increased risk of mortality compared with negative FDG findings. FDG uptake reflects tumor dedifferentiation and is a major negative predictive factor for response to RAI treatment. An SUVmax >5.0 has been associated with very high rates of disease progression even in the presence of mixed iodine-avid disease, and SUVmax >10 has been linked to shorter locoregional disease-free survival and anaplastic transformation. The 2025 ATA guidelines recommend FDG-PET/CT as both a diagnostic and prognostic tool in high-risk patients, particularly those with aggressive histologies or negative RAI imaging.
BRAF/TERT Mutations: Quantified Risk
The co-occurrence of BRAF V600E and TERT promoter mutations is the most powerful molecular predictor of aggressive behavior. A meta-analysis showed this combination was associated with reduced disease-specific survival (RR 15.09, 95% CI 7.75–29.37), far exceeding BRAF V600E alone (RR 5.34). Song et al. (2016) reported that co-existing BRAF + TERT mutations increased recurrence risk (HR 4.64 for BRAF/TERT; HR 5.36 for RAS/TERT) and mortality (HR 15.13 for BRAF/TERT; HR 14.75 for RAS/TERT). Ryu et al. (2026) demonstrated that TERT-mutant tumors show continuous recurrence over time without the expected decline seen in TERT-wildtype cases, and are associated with significantly higher mortality. Xing et al. (2025) showed that the BRAF/TERT genetic duet worsened survival across all AJCC stages.
Reoperative Surgery Outcomes
The 2025 ATA guidelines report that reoperative surgery results in 27% to 63% excellent responses, 5.7% to 13.3% biochemically incomplete responses, 10% to 44% structurally incomplete responses, and 8.6% to 30% indeterminate responses. Independent risk factors for incomplete response after reoperation include age >45 years, aggressive histology, and lymph node ratio >0.6 at initial resection.
The Central Tension: Is Progression Evidence That Surveillance Is Failing?
The assertion that “progression itself is evidence that surveillance is failing” requires nuance. The data suggest that not all progression is equal:
Slow, limited nodal growth in low-risk patients can often be managed with continued observation or delayed intervention without compromising outcomes. In the Jerkovich cohort, all 7 patients who underwent surgery after progression on AS achieved structural complete response. In the Walter cohort, 5 of 6 patients who remained on AS despite progression showed no further growth.
However, the 2026 meta-analysis raises a cautionary note: true progression rates may be 2–3 times higher than reported due to follow-up loss, and AS “should be considered with caution”. Trimboli and Piccardo (2026) argue that until stronger prospective data are available, AS in DTC should be applied within a well-defined multidisciplinary framework with transparent communication about uncertainties.
The evidence therefore supports a nuanced position: AS is appropriate and evidence-based for carefully selected patients with stable, low-volume recurrence, but documented progression—particularly when accompanied by rising Tg kinetics, FDG avidity, aggressive molecular profile, or threatened critical structures—should prompt serious consideration of intervention. The key is that AS is not a passive strategy but an active decision-making framework requiring serial reassessment.
👉A lateral mandibulotomy has several disadvantages:
First, the muscular pull on the two segments of the mandible is unequal:
Putting the mandibulotomy site under significant stress and causing a delay in healing:
For this reason, intermaxillary fixation may be required
Second, the ability to gain access to the suture line to maintain cleanliness following surgery in the oral cavity is hampered as a result of intermaxillary fixation:
Leading to poor oral hygiene and the potential risk for sepsis of the suture line
In addition, a lateral mandibulotomy poses several anatomic disadvantages:
Leading to denervation of the teeth distal to the mandibulotomy site and the skin of the chin:
As a result of transection of the inferior alveolar nerve
A lateral mandibulotomy also causes devascularization of the distal teeth and the distal segment of the mandible:
From its endosteal blood supply
The exposure provided by a lateral mandibulotomy is:
Limited
If the patient needs postoperative radiation therapy:
The mandibulotomy site is directly within the lateral portal of radiation therapy:
Leading to delayed healing and complications at the site of the mandibulotomy
👉For these reasons, a lateral mandibulotomy is not recommended
Are available for resection of primary tumors of the oral cavity
The choice of a particularapproach will depend on factors such as:
The size and site of the primary tumor:
Anterior versus posterior
As well as its depth of invasion
Proximity to the mandible or maxilla
Factorssuch as dentition, size of the oral aperture, trismus, and the size and mobility of the tongue:
Also influence selection of the surgical approach
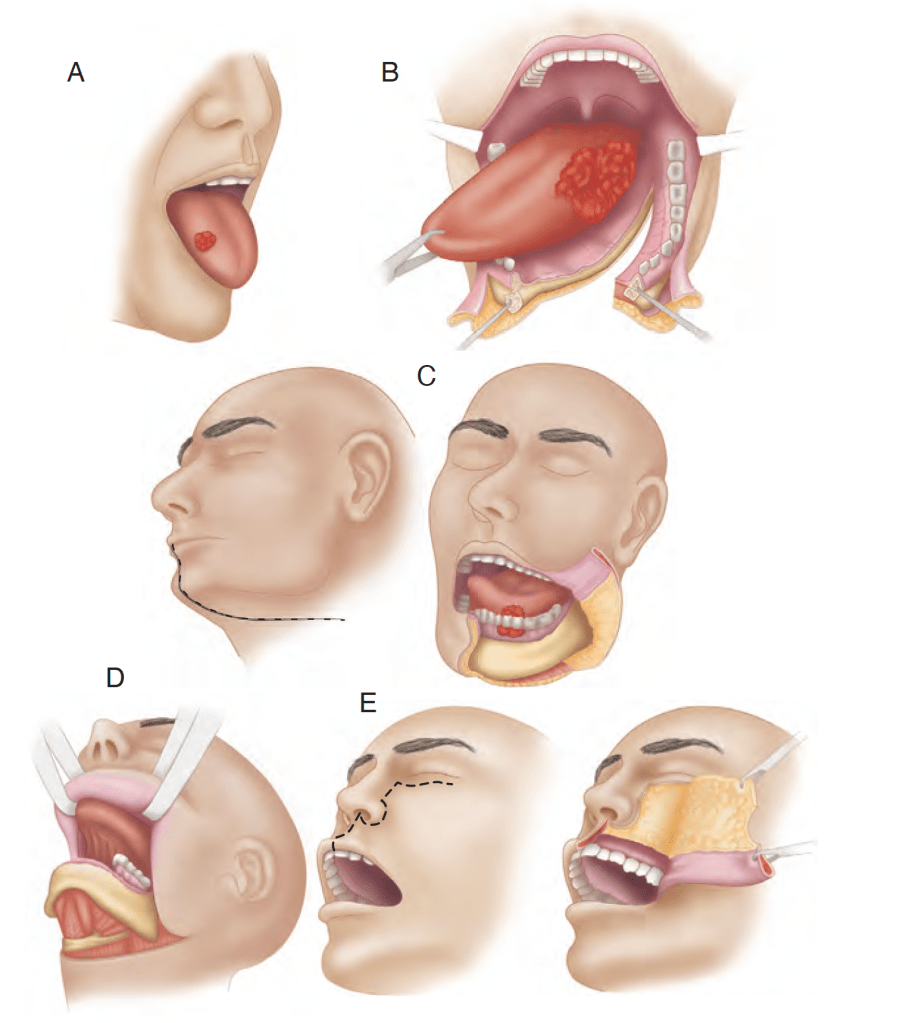
The various surgical approaches such as:
Peroral, mandibulotomy, lower cheek flap approach, visor flap approach, and upper cheek flap approach are shown in Figure
The transoral approach has wider applications with technologic advances using:
Lasers (transoral laser microsurgery [TLM]) and robotics (transoral robotic surgery [TORS])
Various surgical approaches. A, Peroral. B, Mandibulotomy. C, Lower cheek flap. D, Visor flap. E, Upper cheek flap.
When the peroral approach does not offer adequate exposure:
The visor flap or cheek flap approaches (upper or lower) become necessary
The visor flap approach:
Provides sufficient exposure for anteriorly located lesions:
But is not satisfactory for tumors located in the posterior oral cavity
The benefit of this approach is that it avoids a lower lip–splitting incision:
But produces permanent numbness of the chin:
Because the mental nerves need to be transected for adequate mobilization of the flap
It also may cause sagging of the lower lip and drooling:
Because of a loss of support and sensation:
Thus its utility is limited
The lower cheek flap approach:
Requires a midline lip–splitting incision that is continued laterally into the neck for exposureand neck dissection:
This approach provides excellent exposure for nearly all tumors of the oral cavity:
Except those of the upper gum and hard palate
Mandible resection (marginal or segmental) and reconstruction:
Require the lower cheek flap approach in most instances
The lower cheek flap approach:
Is required for marginal or segmental mandibulectomy of tumors adjacent to the body of the mandible
The upper cheek flap approach (the Weber-Ferguson incision and its modifications):
Is required for resection of larger tumors of the hard palate and upper alveolus:
Particularly if they are posteriorly located
Access to larger tumors of the tongue, particularly those closer to the base of the tonguewhere the mandible is not involved:
Requires wider exposure for resection:
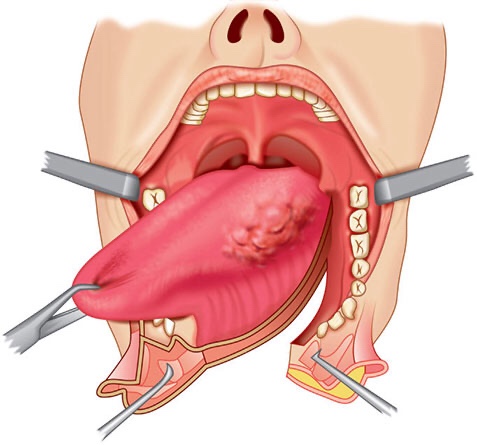
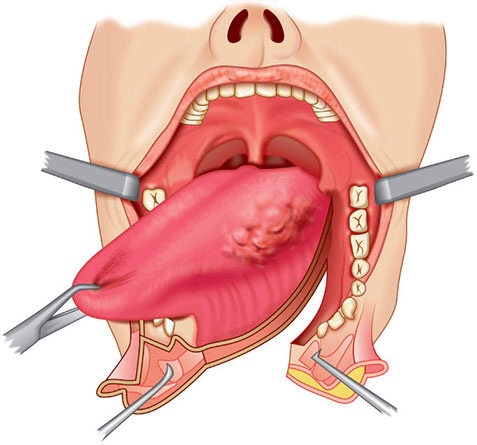
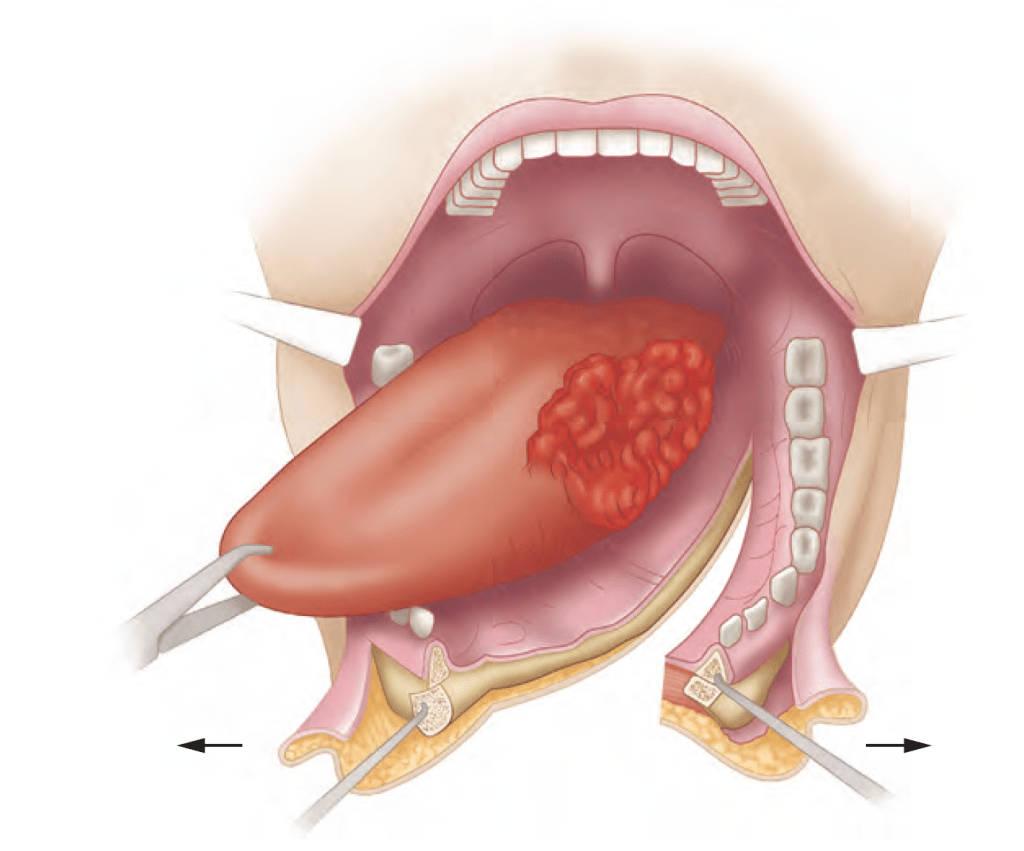
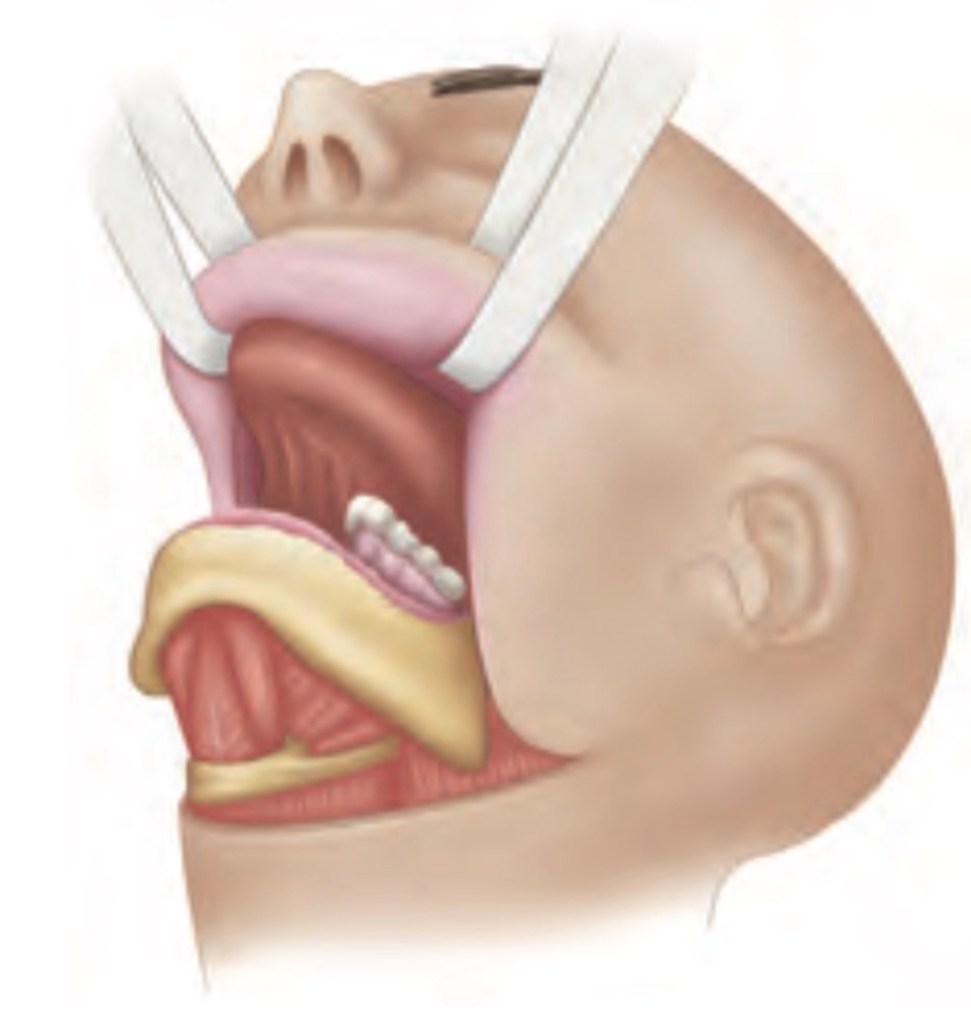
A mandibulotomy or mandibular osteotomy is an excellent mandible sparing surgical approach:
Designed to gain access to the oral cavity or oropharynx for resection of primary tumors otherwise not accessible through the open mouth or by the lower cheek flap approach (Figure)
A mandibulotomy is an excellent mandible-sparing surgical approach to gain access to bulky tumors of the oral cavity or oropharynx.
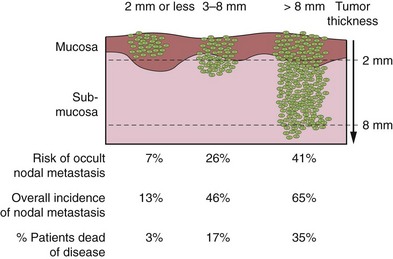
To determine the need and extent of mandible resection:
It is essential to understand the pathwayby which oral cancers invade the mandible
Primary carcinomas of the lip, buccal mucosa, tongue, and floor of the mouth:
Extend along the surface mucosa and the submucosal soft tissues:
To approach the attached labial, buccal, or lingual gingiva
From this point:
The tumor does not extend directly through intact periosteum and cortical bone toward the cancellous part of the mandible:
Because the periosteum acts as a significant protective barrier
Instead:
The tumor advances from the attached gingiva toward the alveolus:
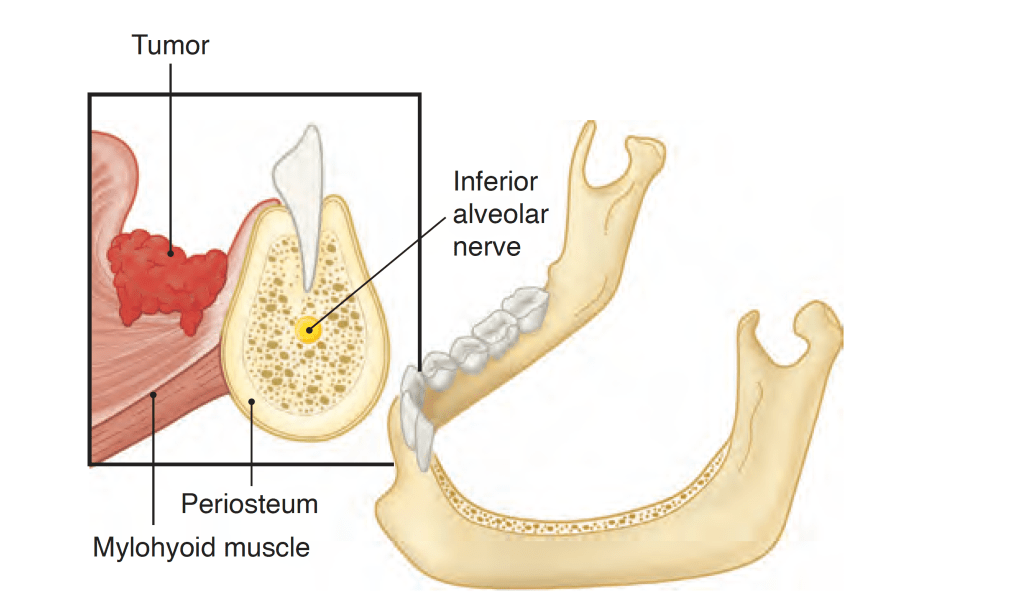
In patients with teeth:
The tumor extends through the dental socket into the cancellous part of the bone and invades the mandible in that fashion (Figure)
Tumor invasion of the dentate mandible occurs through the dental socket to the cancellous bone and then to the alveolar canal
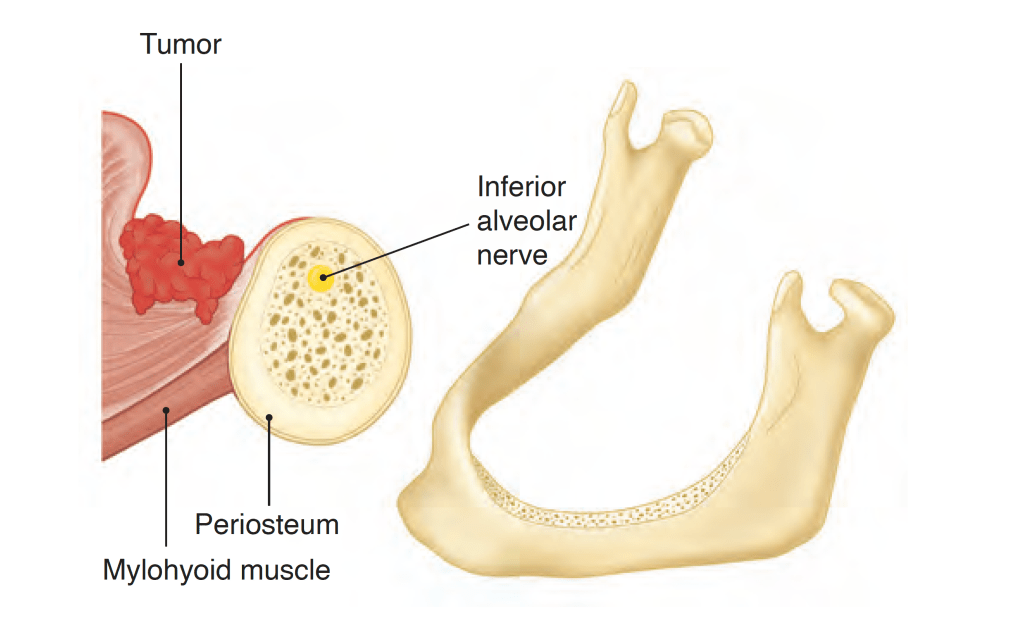
In edentulous patients:
The tumor extends up to the alveolar process and then infiltrates the dental pores in the alveolar ridge and extends to the cancellous part of the mandible (Figure)
Tumor invasion of the edentulous mandible occurs through the dental pores on the alveolar process to the cancellous bone and then to the alveolar canal.
Thus even in patients with early invasion of the mandible:
A marginal mandibulectomy is feasible because the cortical part of the mandible inferior to the roots of the teeth:
Remains uninvolved and can be safely spared
In edentulous patients, however, the feasibility of marginal mandibulectomy depends on the vertical height of the body of the mandible:
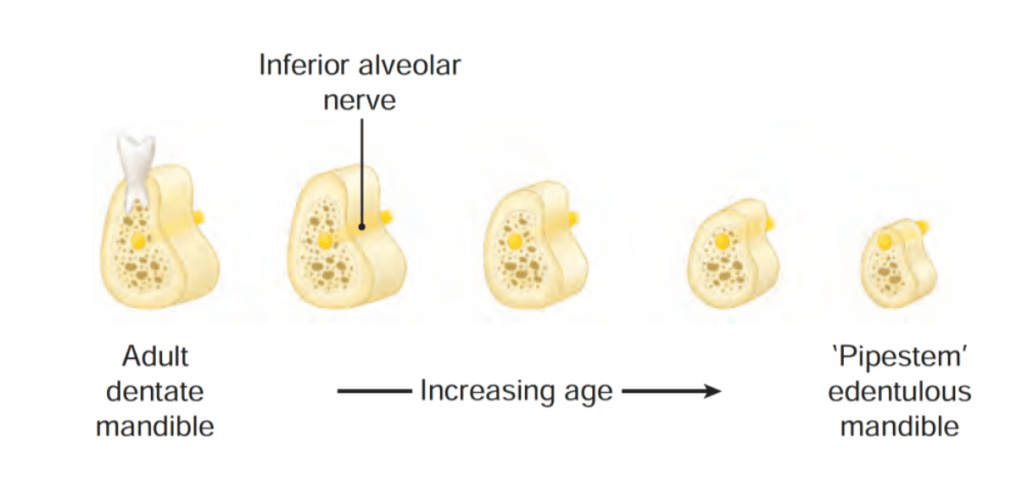
With aging, the alveolar process recedes and the mandibular canal comes closer to the surface of the alveolar process:
As shown in the Figure, the resorption of the alveolar process eventually leads to a “pipestem” mandible in elderly patients
Vertical height and location of the alveolar canal in dentate and edentulous mandibles.
The ability to perform a satisfactory marginal mandibulectomy in such patients is almost impossible:
Because the probability of iatrogenic fracture or postsurgical spontaneous fracture of the remaining portion of the mandible is very high:
Similarly, in patients who have received previous radiotherapy:
A marginal mandibulectomy should be performed with extreme caution:
The probability of pathological fracture at the site of the marginal mandibulectomy in such patients is very high
When the tumor extends to involve the cancellous part of the mandible:
A segmental mandibulectomy must be performed
A segmental mandibulectomy also may be required in patients with massive primary tumors with significant soft tissue disease in the proximity of the mandible
Rodrigo Arrangoiz MS, MD, FACS, FSSO is an Assistant Professor at New York Medical College School of Medicine Division of Surgical Oncology at Mount Sinai Medical Center
He is first author on some publications on oral cavity cancer:
Oral Tongue Cancer: Literature Review and Current Management
The oral cavity represents the entrance to the upper aerodigestive tract:
Which begins at the lips and ends at the anterior surface of the faucial arch
It is lined by:
Squamous epithelium:
With interspersed minor salivary glands
The oral cavity also contains the:
Dentoalveolar structures:
With the upper and lower dentition
The oral cavity is continuously exposed to inhaled and ingested carcinogens:
Thus it is the most common site for the origin of malignant epithelial neoplasms in the head and neck region
Known carcinogens for oral cavity carcinoma include:
Those present in tobacco, alcohol, and betel nuts
The association of human papilloma virus with oral cancer:
Is not as well established as in oropharyngeal cancers
Primary tumors of the oral cavity may arise from the:
Surface epithelium (most common)
Minor salivary glands
Submucosal soft tissues
Lesions of dentoalveolar origin:
Representing a unique group of neoplasms and cysts
The various anatomic sites within the oral cavity as described by the American Joint Committee on Cancer (AJCC) and International Union Against Cancer (UICC) staging system are shown below:
Anatomic sites within the oral cavity
More than 90% of malignant tumors in the oral cavity are:
Squamous cell carcinomas:
The remainder are:
Minor salivary gland carcinomas and other rare tumors
Most patients with cancer in the oral cavity are men:
Although the incidence of tongue cancer in women in the United States has progressively increased over the past several decades
In the Western world:
The tongue (> 50% of cases) and floor of the mouth:
Are the most common sites of origin for primary squamous cell carcinomas in the oral cavity:
However, the retromolar trigone and buccal mucosa:
Are the most frequently encountered primary sites in areas of the world where chewing of tobacco and / or betel nuts is common
The site distribution of various primary cancers in the oral cavity in the United States is shown bowls:
The site distribution of primary cancers in the oral cavity (MSKCC data 1985 to 2015; all patients re-staged according to AJCC 8th edition criteria).
– The goals of treatment of cancer of the oral cavity are:
Cure of the cancer
Preservation or restoration of:
Speech, mastication, swallowing, and external appearance
Minimization of the sequelae of treatment such as:
Dental decay, osteonecrosis of the mandible, and trismus
Awareness of the risk of subsequent primary tumors and their management
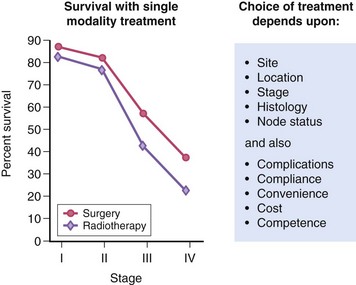
– Surgery and radiotherapy can be used as a single modality or in combination for the treatment of cancer of the oral cavity
– Treatment Approaches:
In general, early-stage (stage I or II) head and neck tumors:
May be treated using a single modality (surgery or radiotherapy):
Whereas advanced disease (stage III or IV) frequently benefits from multimodality therapy
The best therapeutic approach for the primary tumor depends on the anatomic site
Most neck disease can be treated equally well with surgery or radiation:
Thus the modality chosen to treat the neck is based on which modality is selected for the primary
When the primary tumor is treated with irradiation:
The regional lymphatics “at-risk” are incorporated into the treatment fields
Neck dissections should remain standardized (ie, complete anatomic dissections, as opposed to “berry picking” or random biopsy) in these settings to avoid incomplete surgery
Rodrigo ArrangoizSinai Medical Center in Miami, Florida:
He is first author on some publications on oral cavity cancer:
Oral Tongue Cancer: Literature Review and Current Management