-
The basic functional unit of the thyroid gland is the:
-
Thyroid follicle:
-
The thyroid follicle is made up of a:
-
Single layer of cells that forms a sphere that surrounds a protein aggregate called colloid.
-
-
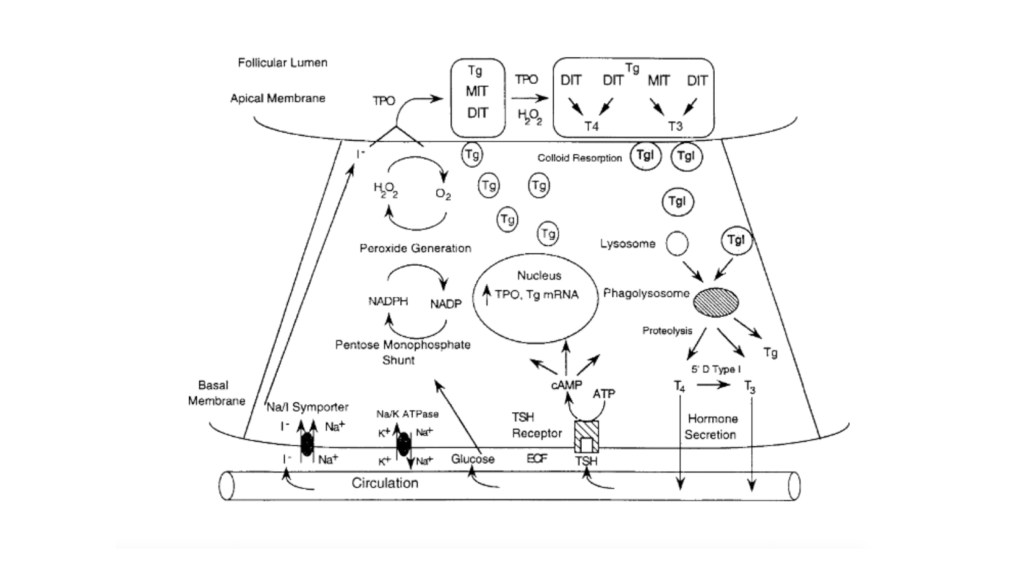
The thyroid follicular cells are polarized:
-
With the side toward the colloid called the:
-
Apical membrane
-
-
And the outer side of the cell in contact with capillaries called the:
-
Basal membrane (Figure)
-
-
-
-
-
The synthesis of thyroid hormone is activated after binding of:
-
Thyrotropin-stimulating hormone (TSH) to the basal membrane surface receptor:
-
The TSH receptor
-
-
TSH stimulates all the steps of thyroid hormone synthesis and secretion, including:
-
Iodide transport
-
Synthesis of thyroglobulin
-
Iodination of thyroglobulin
-
Secretion of thyroid hormones
-
-
TSH binding of the TSH receptor on the basal membrane of the thyroid follicular cell activates adenylate cyclase:
-
To increase intracellular cAMP:
-
Which activates a cascade of numerous steps in the thyroid hormone synthetic pathway
-
-
-
-
The first step is transport of iodide across the basal membrane into the follicular cell in an energy-dependent manner by the Na+/I symporter:
-
The iodide becomes covalently attached to the precursor thyroid hormone glycoprotein:
-
Thyroglobulin:
-
This occurs at the interface between the apical membrane and the colloid by the enzyme thyroperoxidase (TPO).
-
-
-
-
The iodide is attached to the tyrosine molecules in the thyroglobulin molecule to form:
-
Monoiodotyrosines (MITs) and diiodotyrosines (DITs).
-
TPO enzymatically couples two iodotyrosines to create bioactive thyroid hormones:
-
Two diiodotyrosines (DITs) = L-thyroxine (T4)
-
One monoiodotyrosine (MIT) and diiodotyrosine (DIT) =triiodothyronine (T3).
-
-
The T4 and T3 remain part of the thyroglobulin molecule and is stored as colloid within the interior of the follicle.
-
-
The thyroid gland is a unique endocrine organ:because it stores large amounts of thyroid hormones as colloid that is released as needed through TSH stimulation.
-
In healthy and iodine-sufficient individuals:
-
The majority of thyroid hormone is stored as T4 with a small amount, less than 20%, stored as T3.
-
-
TSH receptor stimulation leads to colloid uptake into the cytoplasm by pinocytosis to form a cytoplasmic vesicle:
-
The cytoplasmic vesicles fuse with lysosomes to from a phagolysosome and the proteases found within the lysosome hydrolyze the peptide bonds of thyroglobulin to release T4 and T3 into the cytoplasm where it diffuses into the bloodstream.
-
Approximately 90 mcg of T4 is secreted from the thyroid each day in adults.
-
T4 and T3 travel in the circulation bound 99.97% and 99.5%, respectively, to a group of serum thyroid hormone binding proteins synthesized in the liver, which include:
-
Thyroxine binding globulin (TBG), transthyretin (also known as prealbumin), and albumin.
-
TBGhas the highest affinity to bind thyroid hormone and is clinically the most important member of this group:
-
TBG carries about 68% of the circulating T4 and 80% of the T3.
-
-
Transthyretin, formally named prealbumin binds with a lower affinity and carries 11% of the circulating T4 and 9% of T3.
-
Albumin has the lowest affinity for thyroid hormone but the largest capacity, binding 20% of the T4 and 11% of the T3.
-
-
More than 99% of thyroid hormones circulate bound to these carrier proteinsand are biologically inactive.
-
The half time of T4 in the blood is 7 to 10 days.
-
The thyroid hormones not associated with protein, free T4 and free T3, can enter the cells and are biologically active.
-
T4 is made exclusively by the thyroid gland, whereas T3 is made primarily in peripheral tissues by deiodination of circulating T4 by a group of enzymes called deiodinases:
-
Deiodinase enzyme activity is tightly regulated to maintain a normal T3 despite fluctuations in T4.
-
-
T3 binds with a much higher affinity to the thyroid hormone receptor and is more biologically active than T4.
-
The activity of a specific 5′-deiodinase and the resulting T3 level can be reduced by:
-
Hyperthyroidism
-
Drugs:
-
Beta-blockers
-
Ipodate
-
Amiodarone
-
Dexamethasone
-
Propylthiouracil,
-
-
Malnutrition
-
Severe illness.
-
-
Conversely, during hypothyroidism, the 5′ deiodinase is activated to ensure that T4 is converted to the more bioactive T3.
-
-
Normally, 20% of the daily T3 requirement is directly synthesized and secreted by the thyroid gland:
-
During starvation and illness:
-
The 5′ deiodinase converts the bioactive T4 and T3 to biologically inactive molecules:
-
Reverse T3 (rT3) and 3, 3′ diiodothyronine
-
-
-
The small quantity of free T3 binds to its intranuclear thyroid hormone receptor to alter gene expression:
-
Which in turn alters cellular function and determines the thyroidal status.
-
The thyroid hormone receptor (TR) is a nuclear protein that is a member of a superfamily of receptors that bind steroid hormone such as retinoic acid, vitamin D, and estrogen.
-
-
-
-

Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
-
He is an expert in the management of thyroid and parathyroid diseases.