http://www.sociedadquirurgica.com
Author: Rodrigo Arrangoiz MS, MD, FACS, FSSO
My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
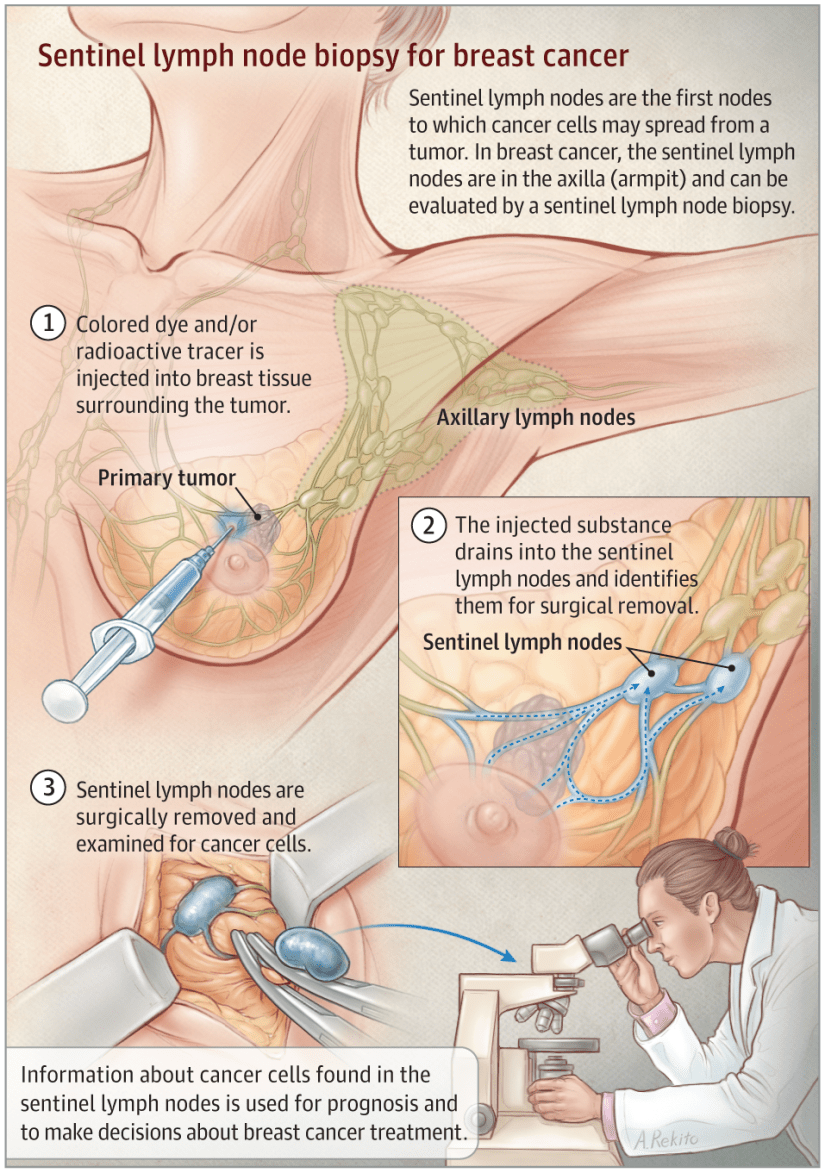
Management of Sentinel Lymph Node (SLN) Positive Breast Cancer Patients
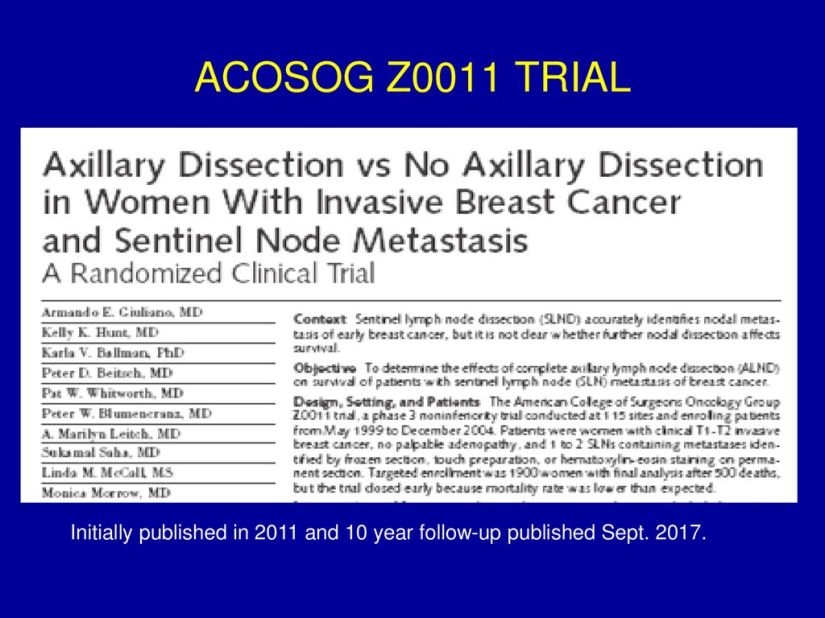
- Traditionally, axillary lymph node dissection (ALND) was performed in the setting of a positive Sentinel Lymph Node (SLN):
- A paradigm shift occurred in 2010 following results of the ACOSOG Z0011 trial which challenged the traditional approach:
- This trial definitively changed the management of SLN positive axillary metastases in patients with early-stage clinically node-negative breast cancer.
- The Z0011 trial enrolled patients with:
- Clinically node-negative
- T1 or T2 early-stage breast cancer undergoing breast conservation therapy (BCT) and SLN dissection
- With three or fewer positive SLNs as detected by hematoxylin and eosin (H&E) staining.
- Critically important to this study was the requirement that:
- All patients received postoperative whole breast radiation and chemotherapy as indicated.
- Patients were randomized to completion axillary dissection versus no further axillary surgery.
- At a median follow-up of 6.3 years:
- There was no difference in overall survival:
- ALND 91.9% vs. 92.5% in SLN-only (P = 0.24)
- There was no difference in disease free survival at 5 years:
- ALND 82.2% vs. 83.8% in SLN-only (P = 0.13)
- There was no significant difference in local recurrence:
- 3.6% of the ALND group versus 1.8% of the SLND-only group.
- After ALND alone:
- Ipsilateral axillary recurrence was identified in 0.5% of patients
- After SLNB alone:
- Ipsilateral axillary recurrence was identified in 0.9%
- There was no difference in overall survival:
- Although this study closed early due to poor accrual:
- Results suggest that in clinically node-negative patients with early-stage breast cancer who will receive whole breast radiotherapy and systemic adjuvant therapy as indicated, ALND does not confer an improved survival advantage:
- In this setting SLN dissection alone for appropriate staging with completed adjuvant therapy may offer excellent regional control with decreased morbidity.
- Results suggest that in clinically node-negative patients with early-stage breast cancer who will receive whole breast radiotherapy and systemic adjuvant therapy as indicated, ALND does not confer an improved survival advantage:
- Since the publication of these practice-changing results,:
- The Z0011 findings have been rapidly and widely adopted and are now considered standard practice.
- It is important to note that these findings are not applicable to all patients including:
- Those with locally advanced (T3 or T4) disease
- Those who received neoadjuvant chemotherapy
- Those undergoing mastectomy
- A paradigm shift occurred in 2010 following results of the ACOSOG Z0011 trial which challenged the traditional approach:
Rodrigo Arrangoiz MS, MD, FACS a surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
-
He is an expert in the management of breast cancer.
-
If you have any questions about the management of Sentinel Lymph Node (SLN) positive breast cancer patients please fill free to contact Dr. Arrangoiz.
-

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer
http://www.sociedadquirurigca.com

Management of Clinical N1 Disease After Neoadjuvant Chemotherapy in Patients with Breast Cancer
Following neoadjuvant chemotherapy for breast cancer:
- Pathologic complete response (pCR) in the axillary nodes:
- Is found in 40% of patients presenting with biopsy proven node-positive disease.
- This observation led to several clinical trials including:
- American College of Surgeons Oncology Group (ACOSOG Z1071)
- SENTINA (Arm C)
- SN FNAC
- This trials evaluated the feasibility and accuracy of sentinel lymph node mapping (SLNM) and sentinel lymph node biopsy (SLNB) dissection as axillary staging after neoadjuvant chemotherapy in clinical N1 disease.
- Although the false-negative rate of SLNB in this setting was above the predetermined threshold, several important factors associated with and impacting the false negative rate were described.
- This included:
- Use of dual agent mapping technique
- Evaluation of at least 3 SLNs
- Immunohistochemistry (IHC) evaluation in addition to H&E staining
- Excision of the clipped (biopsy proven) node.
- This included:
- This observation led to several clinical trials including:
- Is found in 40% of patients presenting with biopsy proven node-positive disease.
- The ACOSOG Z1071 trial evaluated the false-negative rate (FNR) in patients with clinical N1 disease in whom at least 2 SLNs were identified:
- This FNR was 12.6%.
- The FNR was improved to 10.8%:
- In patients in whom both radioisotope and blue dye were used.
- In addition, the FNR in the Z1071 trial varied based on the number of SLNs identified:
- For patients with a single SLN identified,:
- The FNR was 31.5%
- For those with 2 SLNs identified:
- The FNR was 21.1%
- For those with 3 or more SLNs identified:
- The FNR was 9.1%
- For patients with a single SLN identified,:
- Data from the SENTINA trial also showed an improved FNR in patients in whom 3 or more SLNs were identified:
- The trial was a 4-arm multicenter study.
- Arm C was similar to the ACOSOG Z1071 trial in that it included patients who were clinically node-positive and converted to clinically node-negative (non-palpable) after chemotherapy:
- The FNRs were 24.3% when a single SLN was identified
- 18.5% when 2 SLNs were removed
- Less than 10% when 3 or more SLNs were removed
- Similar to the Z1071 trial:
- The FNR was lower (8.6%) for patients who underwent mapping with radioisotope and blue dye.
- The more recently reported SN FNAC study required the use of immunohistochemistry and considered SLN metastases of any size, including isolated tumor cells, to be positive:
- Using this definition,:
- The FNR was 8.4%.
- If isolated tumor cells identified by immunohistochemistry had been considered negative:
- The FNR would have increased to 13.3%.
- Using this definition,:
- The results of these findings led to refined technique termed targeted axillary dissection (TAD):
- This procedure involves SLNB dissection and selective targeted excision of the clipped (biopsy proven) axillary node.
- Response is documented during chemotherapy with ultrasound and clinical exam.
- In selected patients planned for TAD, the clipped node is preoperatively localized with an I-125 radioactive seed or wire.
- Intraoperatively, dual lymphatic mapping for SLN identification is employed and targeted excision of the clipped node is performed.
- Excision is confirmed with specimen radiograph.
- In approximately 23% of cases the clipped node will not be a sentinel node.
- Compared with ALND:
- The false-negative rate of this approach was:
- 10.1% with sentinel node biopsy alone
- 4.2% for excision of the clipped node alone
- 2.0% for TAD.
- The false-negative rate of this approach was:
- In carefully selected patients TAD alone may offer an accurate approach to axillary staging and assessment of residual disease with limited morbidity.
Rodrigo Arrangoiz MS, MD, FACS a surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
-
He is an expert in the management of breast cancer.
-
If you have any questions about SLNM and SLNB after neoadjuvant chemotherapy in breast cancer please fill free to contact Dr. Arrangoiz.
-
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016
#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer
http://www.sociedadquirurigca.com
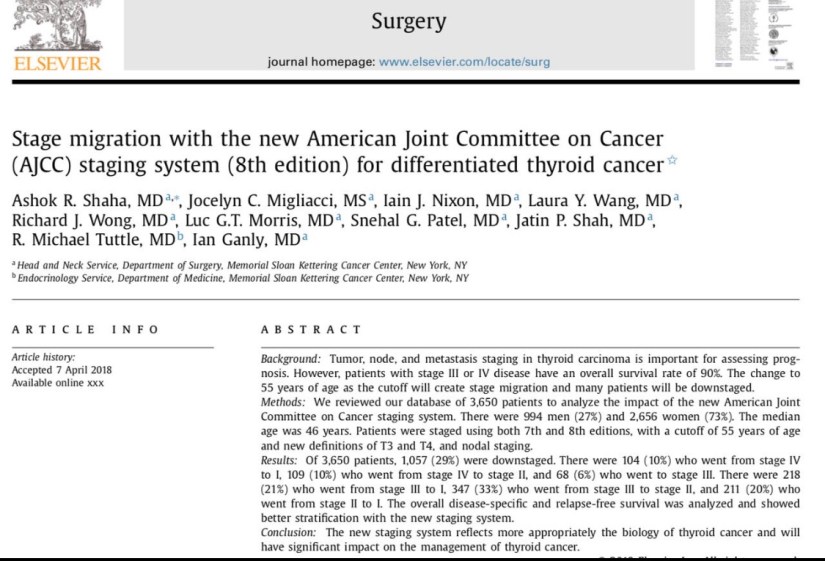
Thyroid Cancer
#Arrangoiz
#ThyroidExpert
#ThyroidSurgeon
#CancerSurgeon
#HeadandNeckSurgeon
#SurgicalOncologist
#CirugiadeTumoresdeCabezayCuello
#CirugiaTiroides
#ExpertoenTiroides
#CirujanodeCancer
#CirujanoOncologo
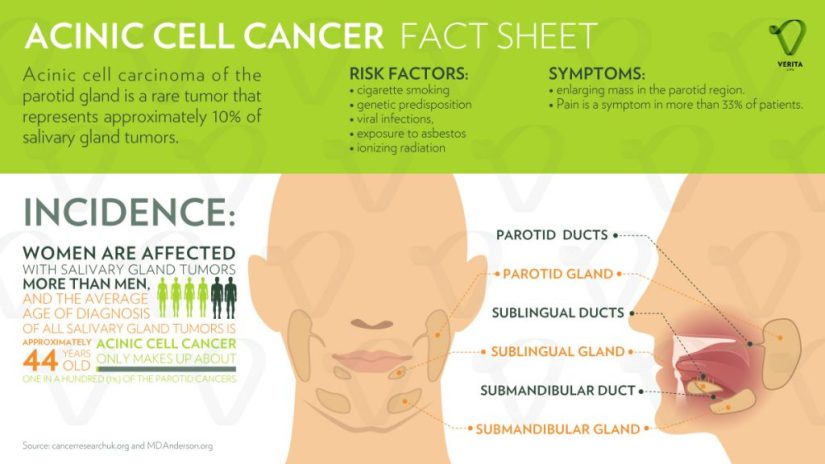
Acinic Cell Carcinoma (AcCC)
-
Acinic cell carcinoma (AcCC) is the second most common malignant tumor involving the parotid gland:
-
Representing 15% of malignant parotid gland neoplasms:
-
It accounts for approximately:
-
5% to 17% of all salivary gland tumors
-
10% to 17% of all malignant salivary gland tumors
-
-
-
-
The parotid gland is composed almost exclusively of serous type acini:
-
It is the most common site of AcCC:
-
80% to 90% of cases
-
-
Other reported sites are:
-
The palate:
-
Up to 15% of the cases
-
-
Submandibular gland:
-
4% of the cases
-
-
Sublingual gland:
-
1% of the cases
-
-
-
-
AcCC occurs most often in:
-
The fifth decade of life
-
In women more often than in men (ratio 3:2)
-
-
It is generally a low-grade carcinoma with indolent behavior.
-
Recurrences are usually delayed, sometimes after decades:
-
In a series reported by Ellis et al:
-
12% of tumors recurred
-
8% metastasized:
-
Regional lymph nodes, bone, lung, and brain:
-
The regional lymph nodes were the most common site of metastases:
-
Spafford et al. reported cervical lymphadenopathy to be present in 10% to 15% of cases of AcCC and Spiro et al. in a series of 67 cases with AcCC treated before 1968, identified five cases (7.5%) with cervical metastases at the time of initial treatment.
-
-
-
-
-
-
It is interesting that this tumor is the most common bilateral malignant salivary gland neoplasm:
-
Although its bilateral presentation is not nearly as common as the bilateral presentations of benign tumors:
-
Warthin’s tumor and pleomorphic adenoma
-
-
-
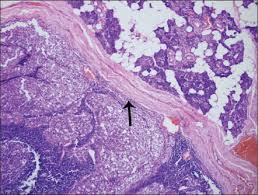
AcCC are typically encased in a fibrous capsule:
-
Grossly resembling round circumscribed nodules with a tan surface:
-
The cut surface is solid but may show cystic degeneration and hemorrhage
-
-

-
Histologically, there are five cell types:
-
Serous acinar cells (explaining the predilection for the parotid gland)
-
Cells with clear cytoplasm
-
Intercalated ductal cell
-
Nonspecific glandular cell
-
Vacuolated cell
-


-
The microscopic recognition of AcCC also requires a strong appreciation for its varied growth pattern:
-
There are four histologic growth patterns:
-
Solid
-
Microcystic
-
Papillary
-
Follicular
-
-
Caution must be taken not to misread:
-
The solid pattern as normal parotid parenchyma
-
The papillary-cystic pattern as cystic mucoepidermoid carcinoma
-
The follicular pattern as metastatic thyroid carcinoma
-
-
Serous acinar differentiation is developed most fully in the acinic cell.
-
These cells have dark round nuclei and granular purplish cytoplasm.
-
-
The diagnosis of AcCC may be difficult to establish, especially when some other cell type dominates the histopathology picture:
-
Some examples of this are the predominance of clear cells might cause confusion with mucoepidermoid carcinoma, clear cell adenocarcinoma, and metastatic renal cell carcinoma:
-
In these circumstances, the diagnostic acinic cells can be identified using a periodic acid-Schiff(PAS) reagent (their cytoplasmic secretory granules are PAS positive and diastase resistant).
-
-
-
Overall survival has been crudely estimated to be about 84%:
-
Survival at 5 years has been reported between 76% to 90%, but fell to 56% at 20 years:
-
Emphasizing the need for long-term follow-up
-
-
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British CowdrayMedical Center in Mexico City:
-
Articles and book chapters published by Dr. Arrangoiz on salivary gland neoplasms:
-
Rodrigo Arrangoiz, Pavlos Papavasiliuo, David Sarcu, Thomas J. Galloway, John A. Ridge, Miriam Lango. Current Thinking on Malignant Salivary Gland Neoplasms. Journal of Cancer Treatment and Research. Vol. 1, No. 1, 2013, pp. 8-24. doi: 10.11648/j.jctr.20130101.12
-
Malignant Salivary Gland Neoplasms Literature Review
-
-
He is an expert in the management of salivary gland neoplasms:
-
If you have any questions about salivary gland neoplasms please fill free to ask Dr. Arrangoiz
-
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016
#Arrangoiz
#HeadandNeckSurgeon
#SurgicalOncologist
#Surgeon
#CancerSurgeon
#CirujanodeCabezayCuello
#CirujanoOncologo
http://www.sociedadquirurgica.com
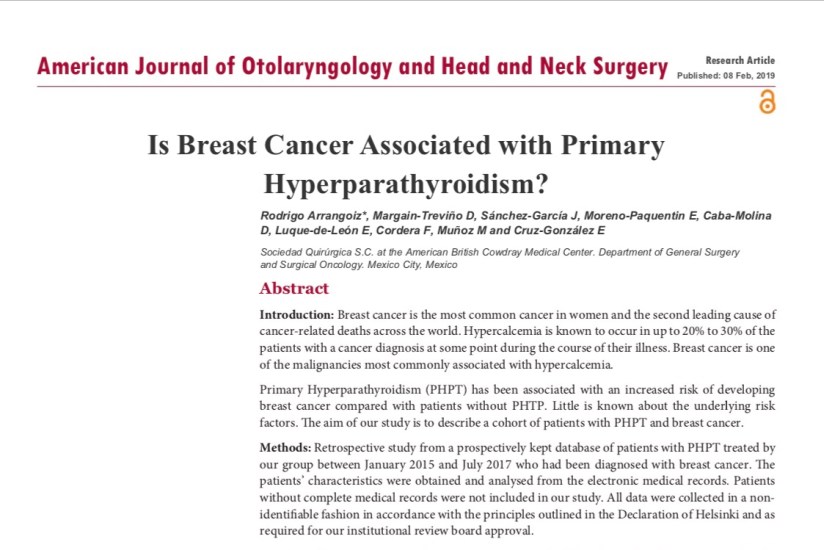
Is Breast Cáncer Associated with a primary Hyperparathyroidism?
Artículo publicado por el equipo de Sociedad Quirúrgica SC
Autor principal Rodrigo ARRANGOIZ MS, MD, FACS
remedypublications.com/american-journal-of-otolaryngology-and-head-and-neck-surgery/articles/pdfs_folder/ajohns-v2-id1033.pdf
TOPDOCTORS Award a Rodrigo Arrangoiz MS, MD, FACS
Rodrigo Arrangoiz MS, MD, FACS miembro de Sociedad Quirúrgica S.C. fue reconocido por #TOPDOCTORS como médico de excelencia en el año 2018:

#Arrangoiz
#ThyroidExpert
#ThyroidSurgeon
#CancerSurgeon
#HeadandNeckSurgeon
#SurgicalOncologist
#CirugiadeTumoresdeCabezayCuello
#CirugiaTiroides
#ExpertoenTiroides
#CirujanodeCancer
#CirujanoOncologo
Hobnail Variant of Papillary Thyroid Carcinoma
👉Trabajo de Sociedad Quirurgica SC, investigador principal Rodrigo Arrangoiz MS, MD, FACS fue presentado en el Miami Thyroid Oncology Symposium Febrero 15 al 16 del 2019.
👉Hobnail Variant of Papillary Thyroid Carcinoma
👉El presentador fue Raúl Moran MD residente de cirugía del hospital ABC.
https://docs.google.com/presentation/d/1j5ZWoGK251CMV44CkzbokQtNc-weNmCVS7WocsDiZDE/edit?usp=sharing




Rodrigo Arrangoiz MS, MD, FACS cirujano de tumores de cabeza y cuello / cirugía endocrina / cirugía oncológica miembro de Sociedad Quirúrgica S.C. experto en el manejo del cáncer de tiroides:
-
Cumple con los requisitos determinados por el Dr. Ashok Saha para realizar cirugía de tiroides de manera efectiva y segura:
Rodrigo Arrangoiz MS, MD, FACS es miembro de la American Thyroid Association:

Entrenamiento:
-
Cirugia general y gastrointestinal:
• Michigan State University:
• 2004 al 2010
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Maestria en ciencias (Clinical research for healthprofessionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

http://www.sociedadquirurgica.com
http://www.hiperparatiroidismo.info
http://www.cirugiatiroides.com
#Arrangoiz
#ThyroidExpert
#ThyroidSurgeon
#CancerSurgeon
#HeadandNeckSurgeon
#SurgicalOncologist
#CirugiadeTumoresdeCabezayCuello
#CirugiaTiroides
#ExpertoenTiroides
#CirujanodeCancer
#CirujanoOncologo
Pathway by Which Oral Cancers Invade the Mandible
To determine the need and extent of mandible resection, it is essential to understand the pathway by which oral cancers invade the mandible .
-
Primary carcinomas of the lip, buccal mucosa, tongue, and floor of the mouth extend along the surface mucosa and the submucosal soft tissues to approach the attached labial, buccal, or lingual gingiva.
-
From this point, the tumor does not extend directly through intact periosteum and cortical bone toward the cancellous part of the mandible because the periosteum acts as a significant protective barrier .
-
Instead, the tumor advances from the attached gingiva toward the alveolus.
-
In patients with teeth, the tumor extends through the dental socket into the cancellous part of the bone and invades the mandible in that fashion (Figure).
-

- Tumor invasion of the dentate mandible occurs through the dental socket to the cancellous bone and then to the alveolar canal.
In edentulous patients, the tumor extends up to the alveolar process and then infiltrates the dental pores in the alveolar ridge and extends to the cancellous part of the mandible (Figure)

- Tumor invasion of the edentulous mandible occurs through the dental pores on the alveolar process to the cancellous bone and then to the alveolar canal.
-
Thus even in patients with early invasion of the mandible, a marginal mandibulectomy is feasible because the cortical part of the mandible inferior to the roots of the teeth remains uninvolved and can be safely spared.
-
In edentulous patients, however, the feasibility of marginal mandibulectomy depends on the vertical height of the body of the mandible .
-
With aging, the alveolar process recedes and the mandibular canal comes closer to the surface of the alveolar process.
-
As shown in the Figure, the resorption of the alveolar process eventually leads to a “pipestem” mandible in elderly patients.
-
-

- Vertical height and location of the alveolar canal in dentate and edentulous mandibles.
The ability to perform a satisfactory marginal mandibulectomy in such patients is almost impossible because the probability of iatrogenic fracture or postsurgical spontaneous fracture of the remaining portion of the mandible is very high.
-
Similarly, in patients who have received previous radiotherapy, a marginal mandibulectomy should be performed with extreme caution.
-
The probability of pathological fracture at the site of the marginal mandibulectomy in such patients is very high.
-
When the tumor extends to involve the cancellous part of the mandible, a segmental mandibulectomy must be performed.
-
A segmental mandibulectomy also may be required in patients with massive primary tumors with significant soft tissue disease in the proximity of the mandible.

Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon and a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center.
He is first author on some publications on oral cavity cancer:
- Oral Tongue Cancer: Literature Review and Current Management
- Understand Cancer: Research and Treatment Oral Cavity Cancer: Literature Review and Current Management.
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

Parotidectomia Realizada por Rodrigo Arrangoiz MS, MD, FACS
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British CowdrayMedical Center in Mexico City:
-
Articles and book chapters published by Dr. Arrangoiz on salivary gland neoplasms:
-
Rodrigo Arrangoiz, Pavlos Papavasiliuo, David Sarcu, Thomas J. Galloway, John A. Ridge, Miriam Lango. Current Thinking on Malignant Salivary Gland Neoplasms. Journal of Cancer Treatment and Research. Vol. 1, No. 1, 2013, pp. 8-24. doi: 10.11648/j.jctr.20130101.12
-
Malignant Salivary Gland Neoplasms Literature Review
-
-
He is an expert in the management of salivary gland neoplasms:
-
If you have any questions about salivary gland neoplasms please fill free to ask Dr. Arrangoiz
-
