- Existen muchos factores en el transcurso de la vida que pueden influir en el riesgo de que tenga cáncer de mama. Algunos factores no se pueden cambiar, como hacerse mayor o los antecedentes familiares, pero usted puede disminuir el riesgo de tener cáncer de mama al cuidar su salud de la siguiente manera:
- Mantenga un peso saludable.
- Haga ejercicio con regularidad.

- No tome alcohol o, si lo hace, limite las bebidas alcohólicas a no más de una por día.
- Si está recibiendo, o le han dicho que reciba, terapia de reemplazo hormonalExternal o anticonceptivos orales (píldoras anticonceptivas), consulte con su médico acerca de los riesgos y averigüe si es lo mejor para usted.
- Si es posible, amamante a sus hijos.
- Si tiene antecedentes familiares de cáncer de mama o cambios heredados en sus genes BRCA1 y BRCA2, hable con su médico acerca de otras maneras de reducir su riesgo.
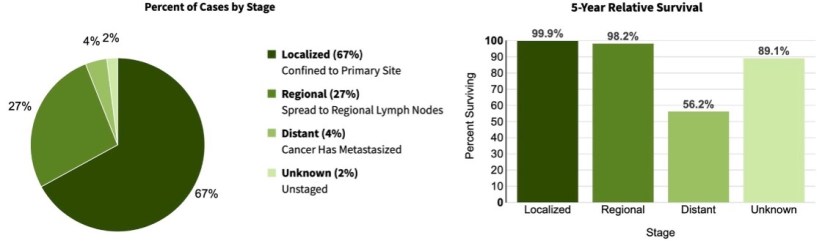
- Mantener una buena salud durante toda la vida disminuirá el riesgo de tener cáncer y mejorará las probabilidades de sobrevivir si se enferma de cáncer.

👉Rodrigo Arrangoiz MS, MD, FACS cirujano oncology y cirujano de mamá de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
-
Es experto en el manejo del cáncer de mama.

👉Es miembro de la American Society of Breast Surgeons:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer
👉Plática del Dr. Arrangoiz sobre el cáncer de mama:












 👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y miembro de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y miembro de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:


