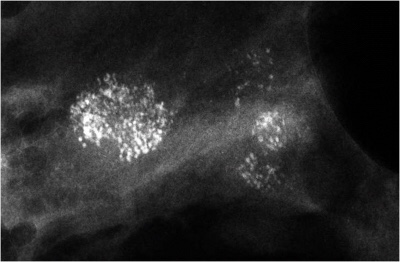
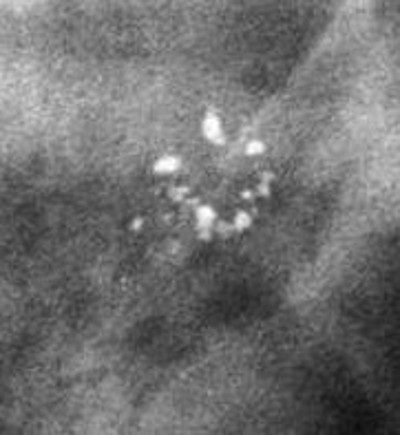

👉The cancers that caused all four of the mammographic abnormalities have the word “ductal” associated with them (Figure 1 and Figure 2: grade 1 and 2 “ductal carcinoma in situ,” Figure 3 and Figure 4 invasive ductal cancers), but it is now thought that 75% of all breast cancers actually originate in the acini of the lobules, and they have a better long-term prognosis than cancers that originate in the lactiferous ducts.
👉The powdery calcifications (Figure 1) are caused by a process most pathologists would term low nuclear grade ductal carcinoma in situ.
👉The “crushed stone” type calcifications (Figure 2) are caused by what would be termed intermediate nuclear grade ductal carcinoma in situ.
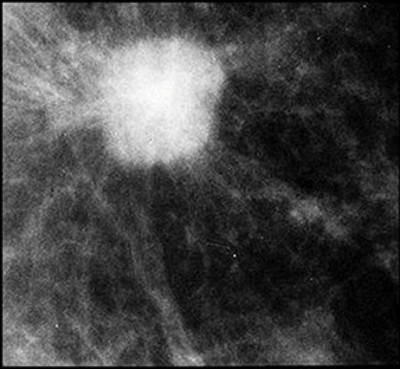
👉The spiculated mass (Figure 3) is the mammographic image of a tumor that would be termed low or intermediate grade infiltrating ductal carcinoma.
👉The round mass (Figure 4) is caused by a process called high-grade infiltrating ductal carcinoma, but it could also be a mucinous carcinoma or an invasive cribriform cancer.
👉Even the high-grade invasive carcinoma has an excellent prognosis if it is screen-detected when it is 14 mm or smaller in size.
👉Since 75% of all breast cancers (described above) originate within the acini of the breast lobules (terminal ductal lobular units), it is misleading to term them “ductal” in situ or invasive “ductal” carcinoma.
👉About 20% of all breast cancers originate in the major (lactiferous) ducts. These are diffuse from the outset since the ducts and their branches are usually filled with grade 3 cancer cells.
👉The graph shows the 25-year follow-up of patients in the Swedish Two-County mammographic screening trial segregated according to mammographic presentation.
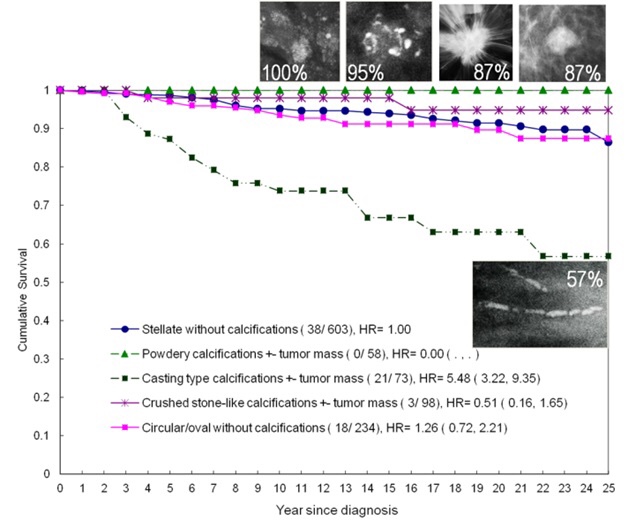
👉The cancers in the group with the poor prognosis originated in the ducts, were diffuse at the time of diagnosis, and had extensive ductal (casting type) calcifications.
👉The similarity of breast and prostate histology is known to all first-year medical students.
👉For years pathologists have classified prostate cancer by its anatomic site of origin.
👉Cancers that begin in the acini are called acinar adenocarcinoma of the prostate and have an excellent prognosis.
👉Those that begin in the ducts are called ductal adenocarcinoma of the prostate and have a poor prognosis.
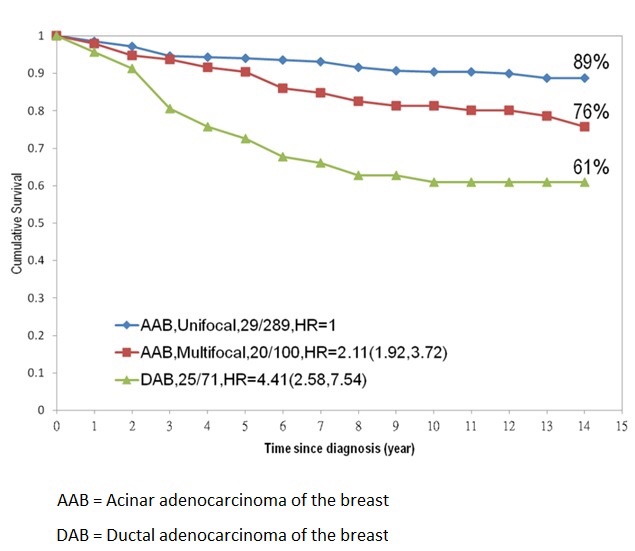
👉In recent years, Tabár and colleagues have called attention to a similar pattern of origin and prognosis for carcinomas of the breast, coining the terms acinar adenocarcinoma of the breast and ductal adenocarcinoma of the breast.
👉The TNM classification system does not always accurately reflect the prognosis of some breast cancers.
👉A 9-mm infiltrating carcinoma would have the same TNM classification regardless of whether it was a unifocal lesion, an extensive multifocal lesion with the largest focus being 9 mm, or a 9-mm infiltrating carcinoma associated with extensive casting calcifications, but the prognosis of each would be markedly different (Graph).

👉Rodrigo Arrangoiz MS, MD, FACS cirujano oncology y cirujano de mamá de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
-
Es experto en el manejo del cáncer de mama.

👉Es miembro de la American Society of Breast Surgeons:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016





 Rodrigo Arrangoiz MS, MD, FACS
Rodrigo Arrangoiz MS, MD, FACS