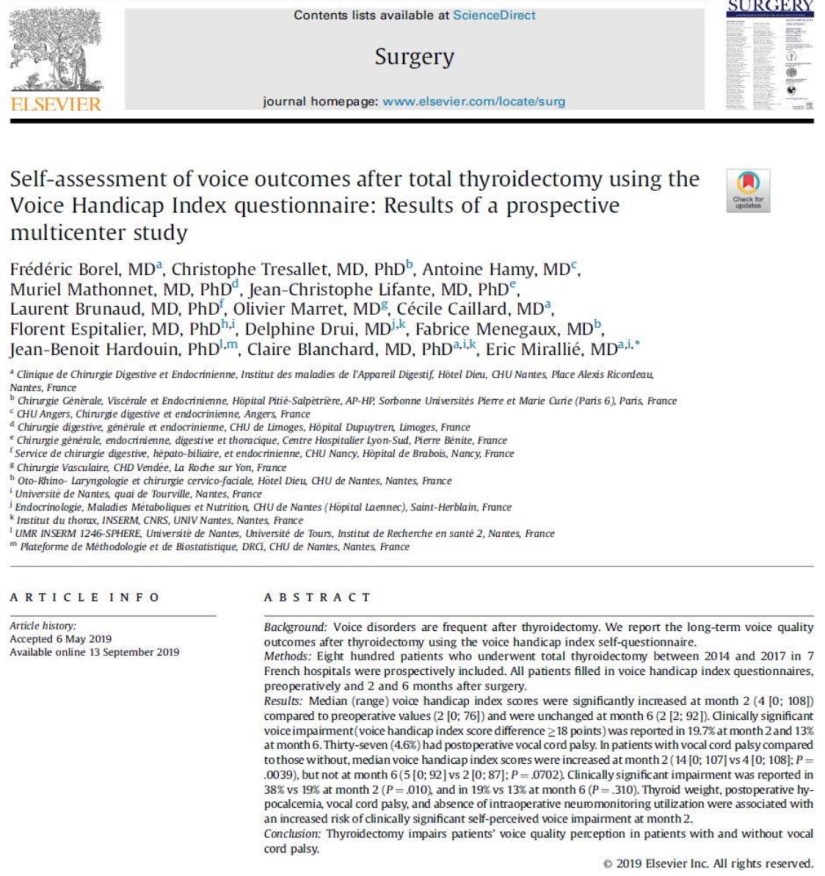
👉Self-rated voice quality is affected post-thyroidectomy even in patients without RLN injury.
👉Read more at:https://www.surgjournal.com/article/S0039-6060(19)30559-8/fulltext
#Arrangoiz
#ThyroidSurgeon
#HeadandNeckSurgeon
👉Self-rated voice quality is affected post-thyroidectomy even in patients without RLN injury.
👉Read more at:https://www.surgjournal.com/article/S0039-6060(19)30559-8/fulltext
#Arrangoiz
#ThyroidSurgeon
#HeadandNeckSurgeon
 👉Need some help staying organized when seeing your doctor for primary hyperparathyroidism?
👉Need some help staying organized when seeing your doctor for primary hyperparathyroidism?
👉Use the handy worksheet from the American Association of Endocrine Surgeons website patient resources found here:
https://collectedmed.com/index.php/article/article/demo_article_display/7552/83/2/1
#Arrangoiz
#ParathyroidSurgeon
#ParathyroidExpert
👉I have been accepted as a member of the American Head and Neck Society
#Arrangoiz
#HeadandNeckSurgeon
#CancerSurgeon
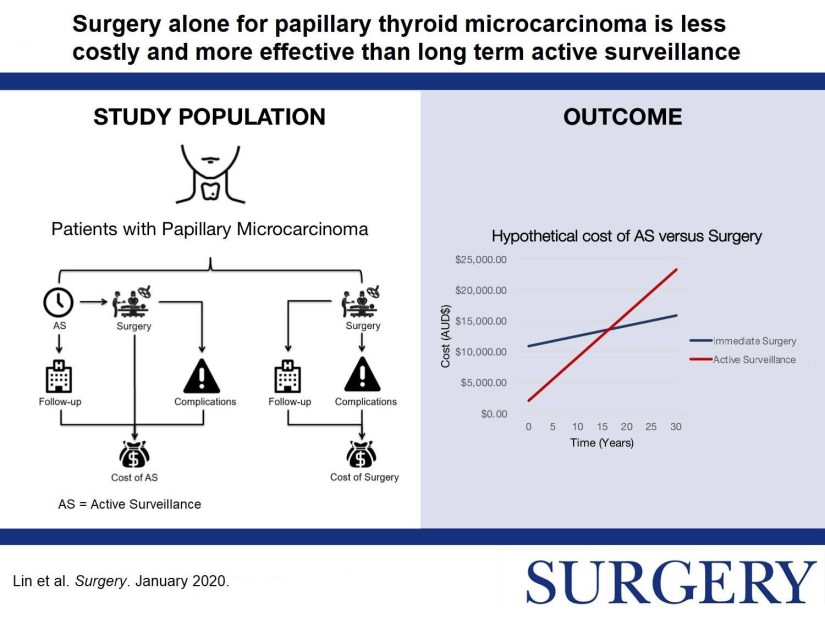
👉Surgery or active surveillance for #thyroid papillary microcarcinoma?
👉More in this study by Dr. Sywak et. al: https://www.surgjournal.com/article/S0039-6060(19)30468-4/fulltext
#Arrangoiz
#HeadandNeckSurgeon
#ThyroidSurgeon
#ThyroidExpert
#ThyroidCancer
#CancerSurgeon
#SurgicalOncologist
#Teacher
#Surgeon
#ThyroidCancer






👉The technique of subtotal thyroidectomy formerly employed relied on the anatomical removal of visibly abnormal thyroid tissue, leaving behind bilateral posterior remnants.
👉The move to total thyroidectomy has meant not only that more thyroid tissue is now removed, but that rather there has been a progressive awareness of the vagaries of embryological development of the thyroid, with dissection now focused on those changes in order to ensure completeness of resection, and thus efficacy of the procedure.
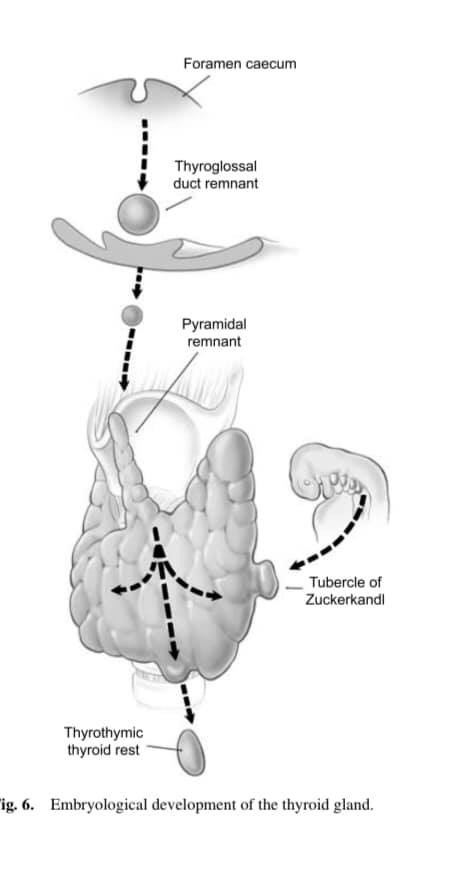
👉Thyroid development involves the midline descent of thyroid tissue from the foramen caecum to the level of the larynx along the thyroglossal tract, at which stage the left and right lobes develop.
👉What is not as well appreciated is that thyroid descent may well continue into the thyrothymic region (and even into the anterior mediastinum) forming a prolongation of thyroid tissue or even completely separate thyrothymic thyroid rests.
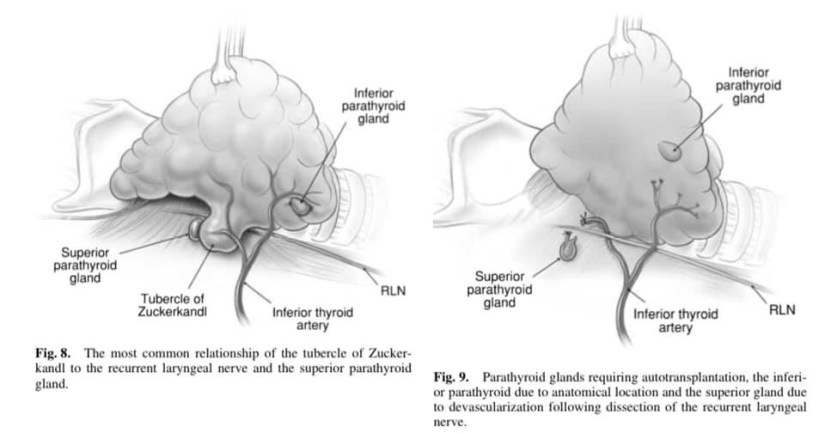
👉In addition the lateral thyroid component arising from the 4th branchial cleft and ultimobranchial body fuses with the median component to form the tubercle of Zuckerkandl, a distinct anatomical structure.
👉This fusion is not only the source of the thyroid’s C-cells, but is also essential in the process of follicular development.
👉Thyroglossal tract and pyramidal remnants – Routine dissection of the pyramidal area up to the laryngeal cartilage should be part of every total thyroidectomy. Even minimal recurrence in this area can be very apparent to the patient. More importantly, in patients with Graves’ disease, a small pyramidal lobe remnant can contain sufficient thyroid tissue to cause clinical recurrence even after an apparent ‘total’ thyroidectomy.
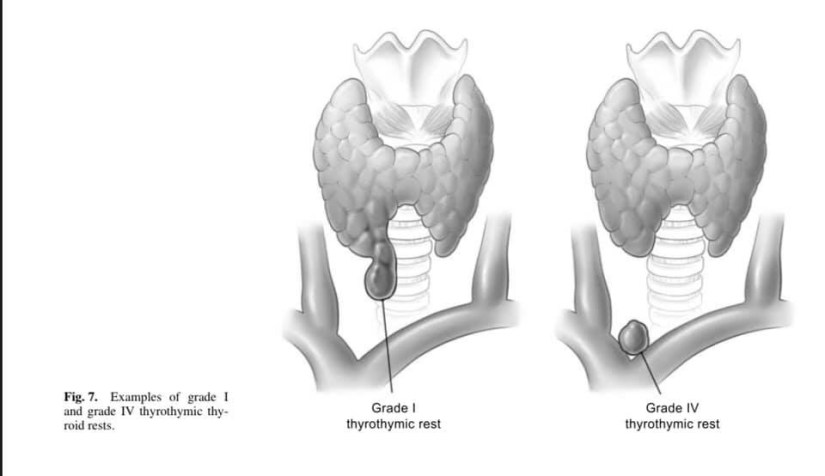
👉Thyrothymic thyroid rests – Thyrothymic thyroid rests are present in over 50% of patients, although most are small. They are often mistaken for small lymph nodes, or even parathyroid glands, and mostly cause no real problems. They are classified according to the nature of their connection to the thyroid gland proper. Grade I is a protrusion of thyroid tissue from the lower edge of the thyroid lobe, grade II is a thyroid rest connected by a bridge of thyroid tissue while grade III is connected by only a fibrovascular core. Grade IV has no connection at all with the thyroid proper. Their clinical significance lies in the fact that, if not removed at the initial operation, they may well reappear as retrosternal recurrence after apparent ‘total’ thyroidectomy. Routine dissection of the thyrothymic area down to the thoracic inlet looking for such rests should therefore be part of every total thyroidectomy.
👉The tubercle of Zuckerkandl – This structure, first described by Zuckerkandl in 1902, is a distinct anatomical entity, and can be found in nearly two-thirds of patients undergoing thyroid surgery. It is classified according to size (grades 0 to grades 3) using a system developed by Pelizzo et al. The tubercle of Zuckerkandl is often the source of local pressure or obstructive symptoms, especially when the thyroid itself is relatively small. The importance of the tubercle of Zuckerkandl, once again, is that if not looked for and removed during thyroid surgery, it may be a source of persistent unrelieved symptoms or recurrence. An understanding of the anatomy of the tubercle of Zuckerkandl is also central to safe surgical dissection. It usually enlarges lateral to the RLN, with the nerve appearing to pass into a cleft medial to it – a situation that some surgeons used to describe as the nerve passing into the thyroid substance. Early elevation of the tubercle of Zuckerkandl usually allows the recurrent nerve to be easily and safely ‘encountered’ even though not initially visible. However, an uncommon but high risk situation is where the RLN runs lateral to an enlarged tubercle of Zuckerkandl, placing it at increased risk of damage during dissection. Another important point is that the normal superior parathyroid gland, also being derived from the fourth branchial cleft, is commonly found in close association, cephalad to the tubercle of Zuckerkandl.
#Arrangoiz
#ThyroidCancer
#ThyroidSurgeon
#ThyroidExpert
#EndocrineSurgery
#HeadandNeckSurgeon
#Arrangoiz
#BreastSurgeon
#CancerSurgeon
#SurgicalOncologist
#Surgeon
#Teacher
#BreastCancer
👉A novel 25 gene panel can be used to predict LN metastasis in early #papillary thyroid cancer (OR = 8.06, P < .001) and disease-free survival (HR = 2.64, P = .043).
👉Read more at:
https://www.surgjournal.com/article/S0039-6060(19)30584-7/fulltext
#Arrangoiz
#ThyroidSurgeon
#ThyroidCancer
#ThyroidExpert
#HeadandNeckSurgeon
#CancerSurgeon
#Teacher

👉A strong correlation b/w immune cell infiltrate and dysregulated thyrocyte DNA repair gene expression suggests a potential mechanism for # papillary thyroid ca development.
More at:https://www.surgjournal.com/article/S0039-6060(19)30459-3/fulltext
#Arrangoiz
#ThyroidSurgeon
#ThyroidExpert
#CancerSurgeon
#Surgeon
#Arrangoiz
#BreastSurgeon
#SurgicalOncologist
#CancerSurgeon
