My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
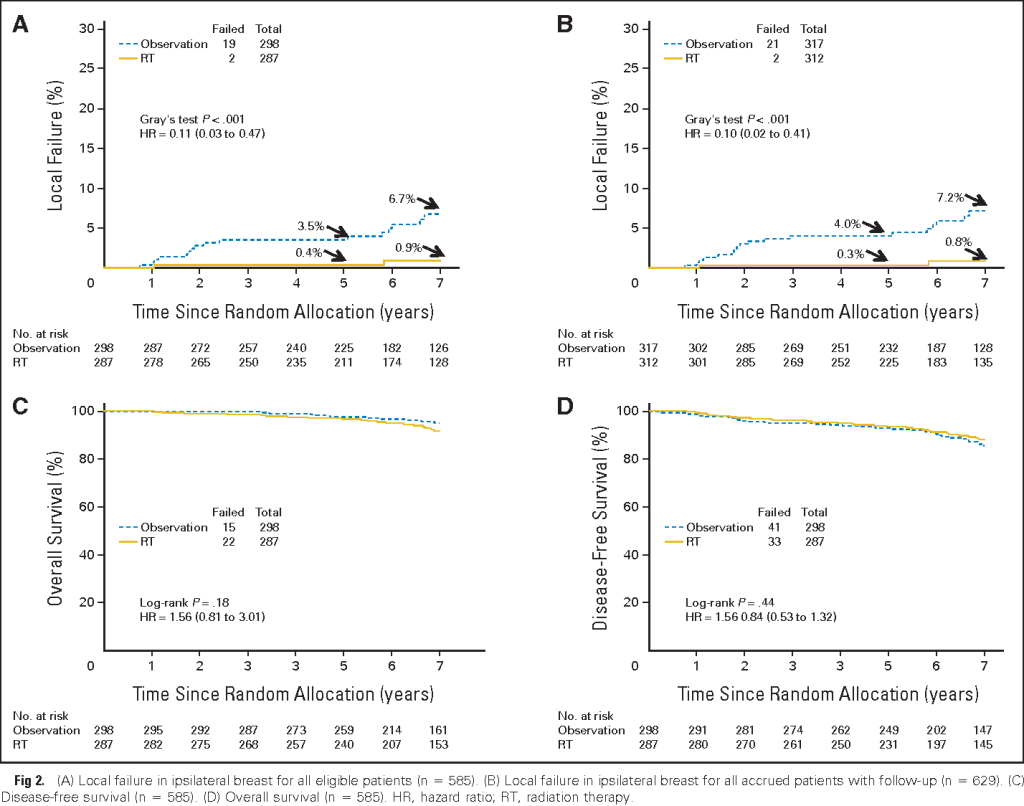
👉The Radiation Therapy Oncology Group (RTOG) 9804 trial evaluated the impact of RT after breast-conserving therapy (BCT) in patients with mammographically detected low-risk DCIS as defined by size <2.5 cm, unicentricity, low- and intermediate-grade, and margins >3 mm.
👉Data were analyzed after a median follow-up of 7.17 years in 636 patients randomly assigned to either RT or observation after BCT.
👉The primary endpoint of ipsilateral local failure was 0.9% in the RT arm versus 6.7% in the observation arm.
PATIENTS AND METHODS:
👉This prospective randomized trial (1998 to 2006) in women with mammographically detected low- or intermediate-grade DCIS, measuring less than 2.5 cmwith margins ≥ 3 mm, compared RT with observation after surgery.
👉The study was designed for 1,790 patients but was closed early because of lower than projected accrual.
👉Six hundred thirty-six patients from the United States and Canada were entered; tamoxifen use (62%) was optional.
👉Ipsilateral local failure (LF) was the primary end point; LF and contralateral failure were estimated using cumulative incidence, and overall and disease-free survival were estimated using the Kaplan-Meier method.
RESULTS:
👉Median follow-up time was 7.17 years (range, 0.01 to 11.33 years).
👉Two LFs occurred in the RT arm, and 19 occurred in the observation arm.
👉At 7 years, the LF rate was 0.9% (95% CI, 0.0% to 2.2%) in the RT arm versus 6.7% (95% CI, 3.2% to 9.6%) in the observation arm (hazard ratio, 0.11; 95% CI, 0.03 to 0.47; P < .001).
👉Grade 1 to 2 acute toxicities occurred in 30% and 76% of patients in the observation and RT arms, respectively; grade 3 or 4 toxicities occurred in 4.0% and 4.2% of patients, respectively.
👉Late RT toxicity was grade 1 in 30%, grade 2 in 4.6%, and grade 3 in 0.7% of patients.
CONCLUSION
👉In this good-risk subset of patients with DCIS, with a median follow-up of 7 years, the LF rate was low with observation but was decreased significantly with the addition of RT. Longer follow-up is planned because the timeline for LF in this setting seems protracted.
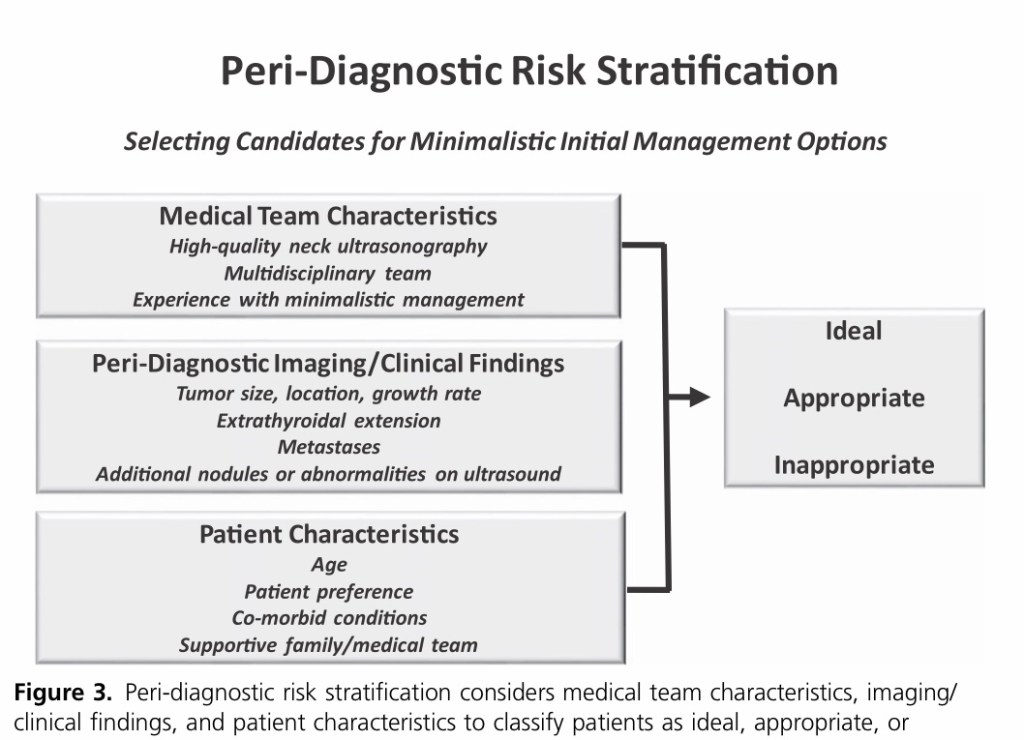
👉Risk stratification begins immediately upon identification of a suspicious thyroid nodule.
👉In the absence of a validated peri-diagnostic risk-stratification system, we use a clinical framework that incorporates tumor imaging characteristics, medical team characteristics, and patient preferences to risk stratify patients as ideal, appropriate, or inappropriate for minimalistic initial management options, such as active surveillance or thyroid lobectomy.
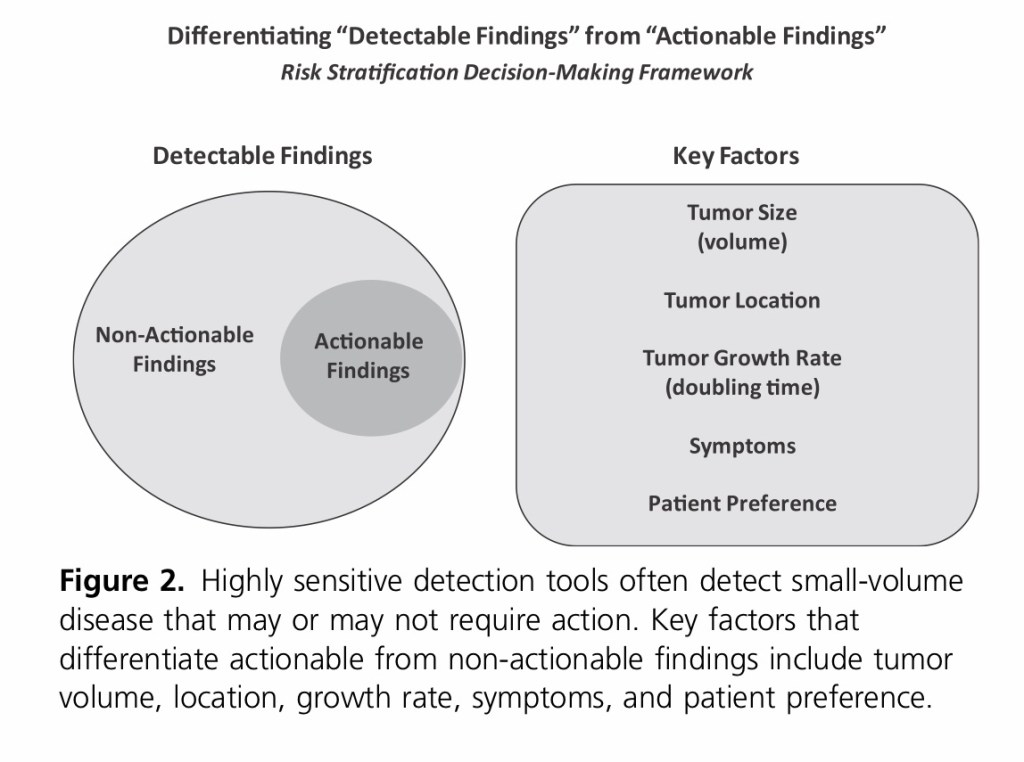
👉This clinical framework address the key factors that differentiate actionable from non-actionable disease.
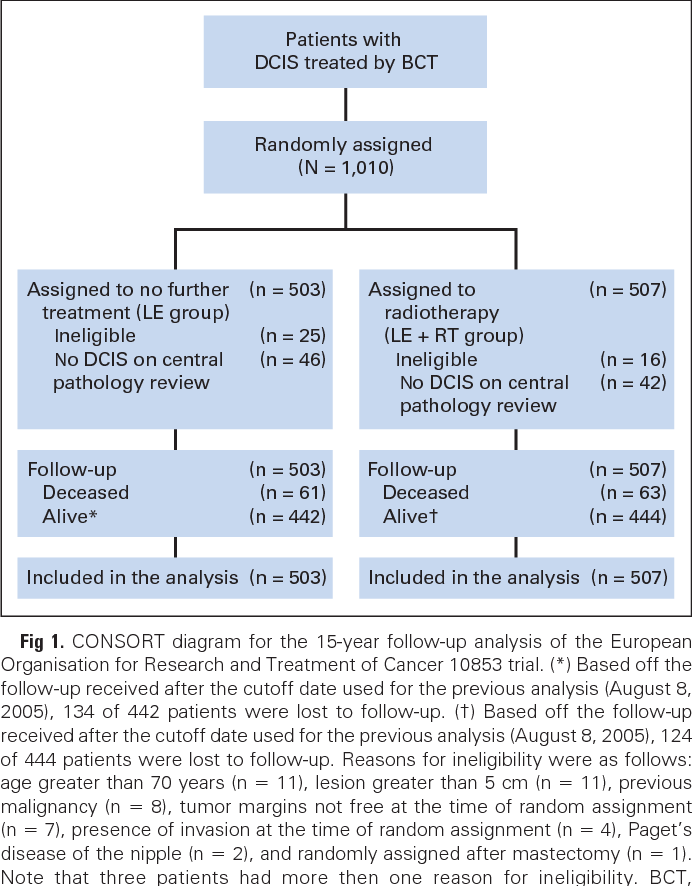
Nina Bijker, Philip Meijnen, Johannes L Peterse, Jan Bogaerts, Irène Van Hoorebeeck, Jean-Pierre Julien, Massimiliano Gennaro, Philippe Rouanet, Antoine Avril, Ian S Fentiman, Harry Bartelink, Emiel J Th RutgersJournal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology 2006 July 20, 24 (21): 3381-7
PURPOSE
👉The European Organisation for Research and Treatment of Cancer conducted a randomized trial investigating the role of radiotherapy (RT) after local excision (LE) of ductal carcinoma-in-situ (DCIS) of the breast. They analyzed the efficacy of RT with 10 years follow-up on both the overall risk of local recurrence (LR) and related to clinical, histologic, and treatment factors.
PATIENTS AND METHODS
👉After complete LE, women with DCIS were randomly assigned to no further treatment or RT (50 Gy).
👉One thousand ten women with mostly (71%) mammographically detected DCIS were included.
👉The median follow-up was 10.5 years.
RESULTS
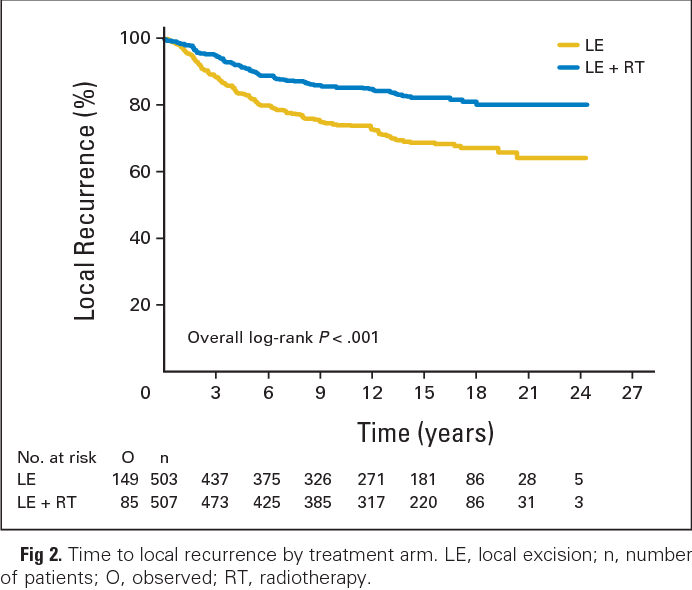
👉The 10-year LR-free rate was 74% in the group treated with LE alonecompared with 85% in the women treated by LE plus RT (log-rank P < .0001; hazard ratio [HR] = 0.53).
👉The risk of DCIS and invasive LR was reduced by 48% (P = .0011) and 42% (P = .0065) respectively.
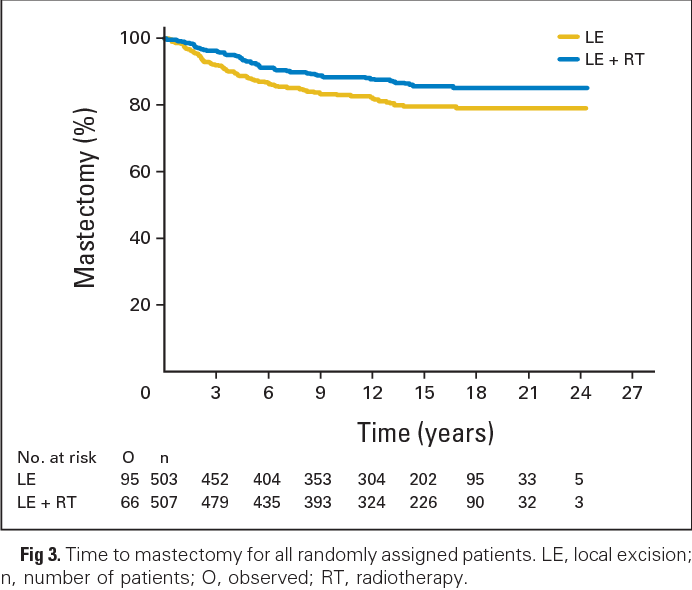
👉Both groups had similar low risks of metastases and death.
👉At multivariate analysis, factors significantly associated with an increased LR risk were young age(< or = 40 years; HR = 1.89), symptomatic detection (HR = 1.55), intermediately or poorly differentiated DCIS (as opposed to well-differentiated DCIS; HR = 1.85 and HR = 1.61 respectively), cribriform or solid growth pattern (as opposed to clinging/micropapillary subtypes; HR = 2.39 and HR = 2.25 respectively), doubtful margins (HR = 1.84), and treatment by LE alone (HR = 1.82).
👉The effect of RT was homogeneous across all assessed risk factors.
CONCLUSION
👉With long-term follow-up, RT after LE for DCIS continued to reduce the risk of LR, with a 47% reduction at 10 years. All patient subgroups benefited from RT.
👉In October 2016, the AJCC (www.cancerstaging.org) published the eighth edition of the AJCC / TNM cancer staging system, which replaced the seventh edition that had been used by clinicians, cancer registries, and researchers since 2009.
👉On the 1st of January 2018, tumor registries officially began using the eighth edition for tumor staging.
👉Whereas the staging tables for medullary thyroid cancer and anaplastic thyroid cancershowed only minimal changes, the rules for the staging of well differentiated thyroid cancer underwent substantial modifications.
👉These included the following:
An increase of the age cutoff from 45 years to 55 years of age at diagnosis
Removal of microscopic extrathyroidal extension as a key component of the staging system
No longer mandating assignment of stage III to older patients with microscopic extrathyroidal extension or lymph node metastases
Establishment of a new T3b category for tumors of any size that demonstrate gross extrathyroidal extension involving only the surrounding strap muscles
👉The AJCC Differentiated Thyroid Cancer Committee carefully considered the possibility of inclusion of mo- lecular markers (specifically, BRAFV600E and TERT promoter mutations) in the AJCC prognostic staging definitions.
👉Whereas both of these mutations, particularly when present together, have been shown to be predictors of poor clinical outcomes, they appeared to add only marginal benefit to the traditional anatomic staging factors.
👉Thus, molecular characterization of differentiated thyroid cancers, although providing some prognostic information,were not powerful enough factors to merit upstaging tumors to prognostic stages above those mandated by TNM risk factors.
👉Nonetheless, similar to the approach used in the ATA risk-stratification system, molecular results can be used to refine further and individualize risk within risk categories or stages.
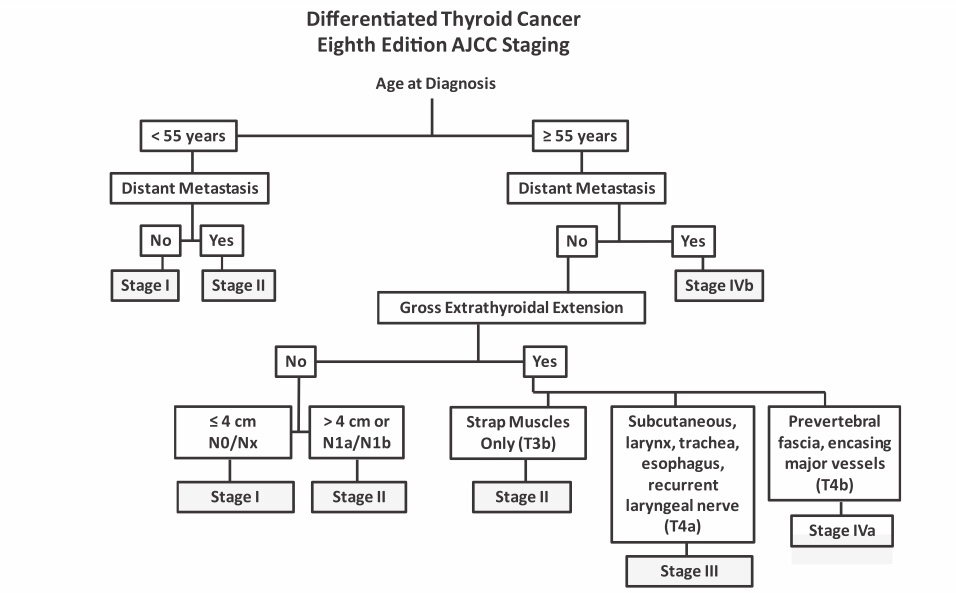
👉The three critical factors that determine the prognostic stage groups of the eighth edition AJCC / TNM cancer staging system include the age at diagnosis,the presence or absence of distant metastases, and the presence or absence of gross extrathyroidal extension.
👉Rather than the use of the standard TNM staging tables provided in the AJCC / TNM manual, I find it easier to use the flow diagram used by MSKCC to stage patients rapidly based on the key clinical risk factors (age at diagnosis, distant metastasis, gross extrathyroidal extension, and lymph node metastases).
A simplified approach to AJCC staging in differentiated thyroid cancer, emphasizing the critical decision factors, which include age at diagnosis, distant metastasis, and gross extrathyroidal extensions.
👉In patients age under 55 years, this figure rapidly classifies patients as either stage I (any T, any N, M0) or stage II (any T, any N, M1).
👉In the older patients (55 years or older), additional factors, such as the presence or absence of distant metastasis, invasion of strap muscles, and extent of gross extrathyroidal extension, are also used to define the prognostic stage groups.
👉In the eighth edition of the AJCC / TNM cancer staging system, it was anticipated that the majority of patients would be classified as stage I or stage II, reflecting the excellent outcomes expected in the majority of thyroid cancer patients.
👉A smaller number of patients, particularly the older patients with either distant metastases or gross extrathyroidal extension, were anticipated to do worse and are therefore classified as stage III or IV.
👉Multiple publications have demonstrated that the eighth edition of the AJCC / TNM cancer staging system moved a substantial number of patients into lower prognostic stage groupswithout affecting the overall survival of those lower-stage groups.
👉The patients who remained in the higher-stage groups had poorer prognoses, as expected.
👉This resulted in a much better separation of the four prognostic stage groups with respect to survival, such that 5- to 10-year disease-specific survival (DSS) was:
99% in stage I patients
88% to 97% in stage II patients
72% to 85% in stage III patients
67% to 72% in stage IV patients
👉Unlike previous editions of the AJCC / TNM staging system in which there was substantial overlap in survival in patients with stage I, II, and III disease, the eighth edition provides meaningful separation among the prognostic stage groups that appear to be clinically relevant.
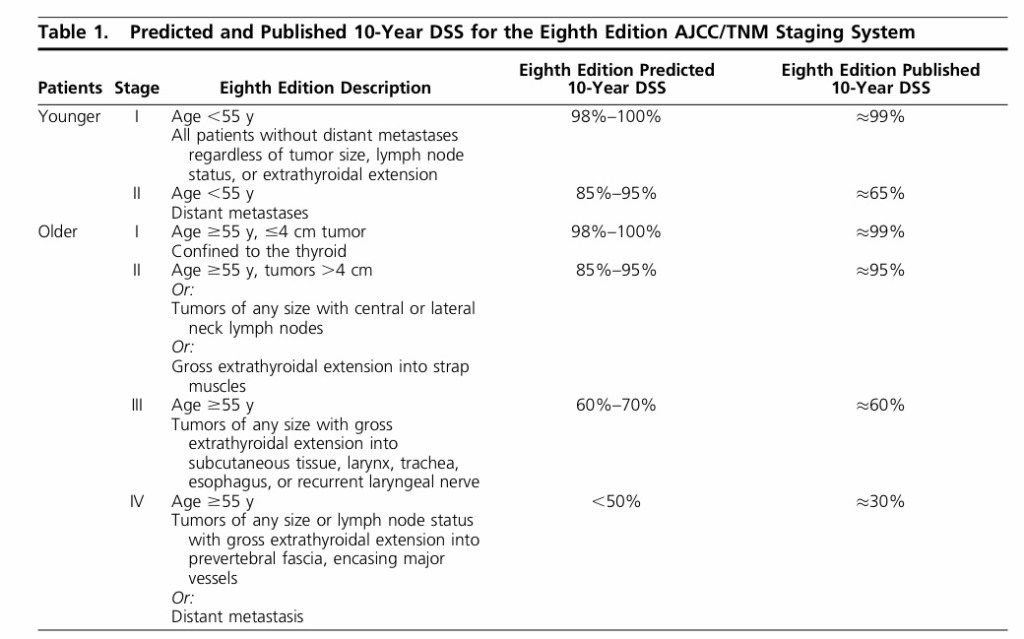
👉The differences in predicted and published 10-year survival rates are best seen when analyzed based on age group (age less than 55 years vs age equal or greater than 55 years) as shown below.
Ten-year median DSS estimates approximated from data extrapolated from publications examining eighth edition AJCC prognostic stages.
👉The predicted 10-year DSS has been validated for all age and stage groups, with only the younger (age less than 55 years) stage II patientsappearing to do more poorly than anticipated.
👉The lower-than-anticipated 10-year DSS in the younger patients (age less than 55 years) with stage II disease was the result of the stage migration of patients in the 45- to 55-year age group from seventh edition AJCC stage IV to eighth edition AJCC stage II.
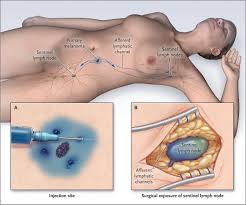
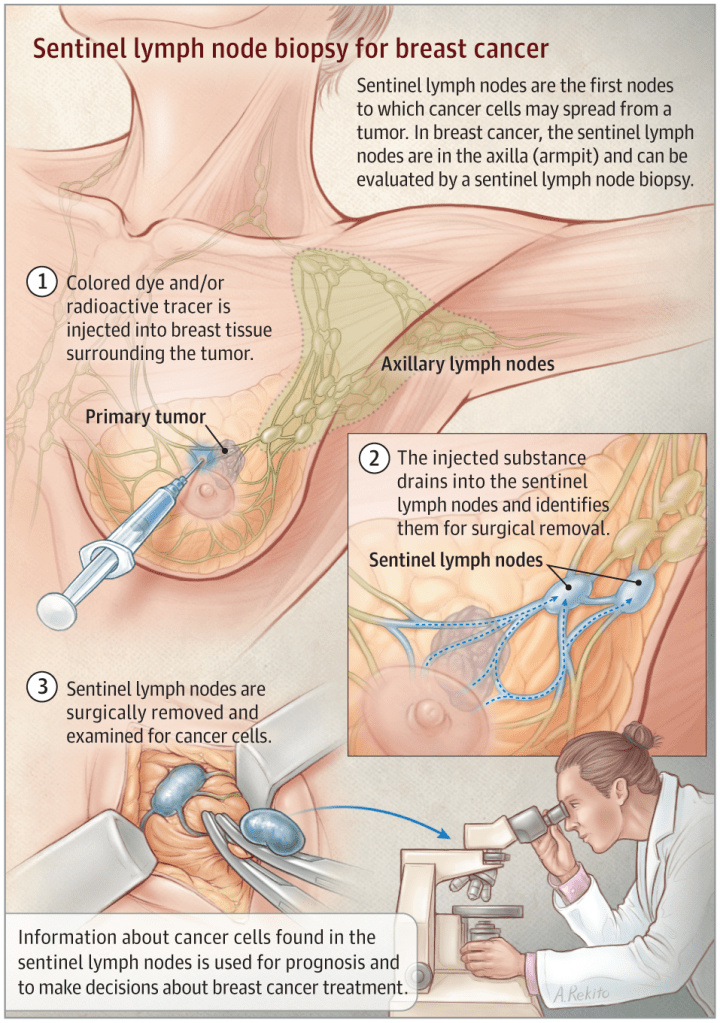
👉Krag et al. first described using technetium-99m sulfur colloid in sentinel node (SN) mapping and noted that he attained an SN identification rate of 98%, with a false-negative rate of 11%.
👉Technetium-99m sulfur colloid is the most widely used radioisotope for lymphatic mapping in the United States.
👉In Europe, technetium-99m colloid albumin is used most often.
👉Similarly, Giuliano et al. described the use of isosulfan blue dye, with a SN detection rate of 98%, without false-negative nodes.
👉Anaphylaxis and hypotension also have been reported as adverse events when using isosulfan blue dye.
👉Overall, isosulfan blue dye is the most commonly used dye for the lymphatic mapping of breast cancer.
👉The SN detection rate using methylene blue has been described as 93%, and concordance with radioisotope was described in 95% of patients.
👉Although methylene blue is available at a lower cost when compared to isosulfan blue, it must be injected carefully into the subcutaneous tissues.
👉Injection into the dermis may lead to epidermolysis and necrosis.
👉Therefore when used, methylene blue should be diluted with saline to minimize these complications (eg, 1 ml of 1% methylene blue diluted with 2 to 3 ml of injectable saline) and injected in the subareolar breast parenchyma deep to the skin.
👉The combination of blue dye and radioisotope improves the SN detection rate as first described by Albertini and colleagues.
👉As a result, several other studies have demonstrated similar findings and, thus, dual-agent lymphatic mapping has been accepted universally as a better method in the detection of the SN.
👉The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-32 used radioisotope and blue dye for the detection of SLNs.
👉Sentinel nodes were identified by blue dye alone in 5.1%, by radioisotope alone in 24.3% and by both tracers in 65.1% of patients.
👉The reported SLN identification rate was 97% with a 9.8% false-negative rate.
The most common adverse events were allergic reactions.
👉Anaphylaxis was also reported as an adverse event.
REFERENCES
Albertini JJ, Lyman GH, Cox C, et al. Lymphatic mapping and sentinel node biopsy in the patient with breast cancer. JAMA. 1996;276:1818-1822.
Giuliano AE, Kirgan DM, Guenther JM, Morton DL. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg. 1994;220:391-401.
Kim T, Giuliano AE, Lyman GH. Lymphatic mapping and sentinel lymph node sampling in breast cancer: a meta-analysis. Cancer. 2006;106:4-16.
Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010;11:927-933.
Krag DN, Weaver DL, Alex JC, Fairbank JT. Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe. Surg Oncol. 1993;2:335-339.
Newman LA, Newman EA. Lymphatic mapping techniques and sentinel lymph node biopsy. Surg Clin N Am. 2007;87:353-364.
Simmons RM, Smith SM, Osborne MP. Methylene blue dye as an alternative to isosulfan blue dye for sentinel lymph node localization. Breast J. 2001;7:181-183.
Simmons R, Thevarajah S, Brennan M, Christos P, Osborne M. Methylene blue dye as an alternative to isosulfan blue dye for sentinel node localization. Ann Surg Oncol. 2003;10:242-247.
Zakaria S, Hoskin TL, Degnim AC. Safety and technical success of methylene blue dye for lymphatic mapping in breast cancer. Am J Surg. 2008;196:228-233.
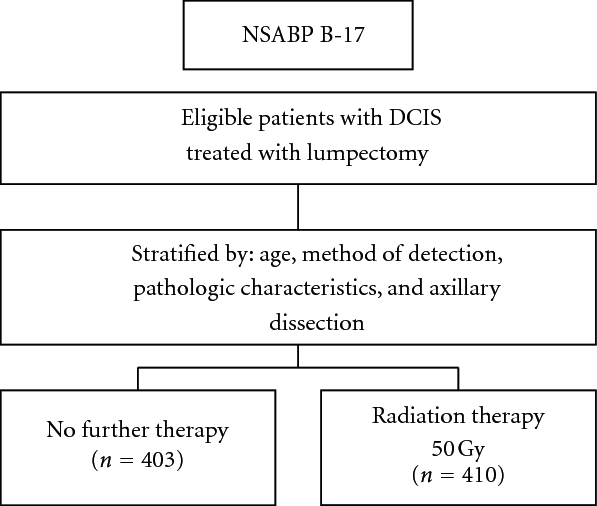
👉The NSABP B-17, Phase III Randomized Study of Postoperative Radiotherapy Following Segmental Mastectomy and Axillary Dissection in Patients with Noninvasive Intraductal Adenocarcinoma of the Breast
👉Compared lumpectomy alone to lumpectomy plus breast irradiation in 818 patients with localized ductal carcinoma in situ.
👉This trial concluded that radiotherapy did not improve OS but that it did significantly decrease the rate of invasive or in situ in breast tumor recurrence in the ipsilateral breast.
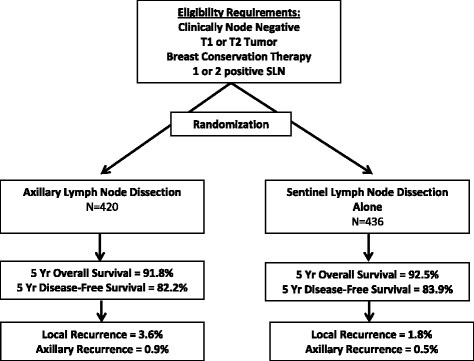
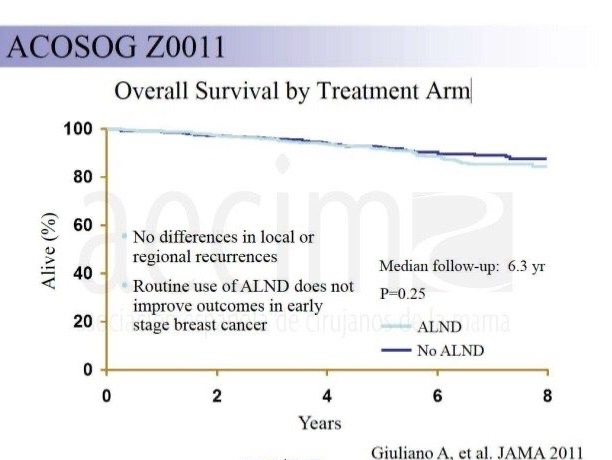
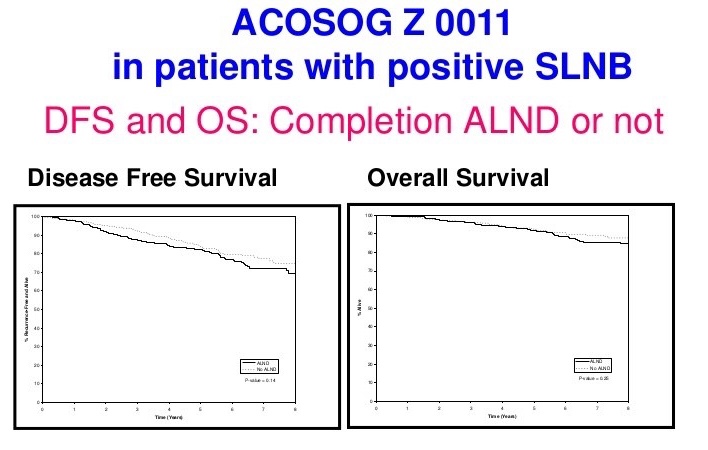
👉Data from the ACOSOG Z0011 trial suggests completion axillary dissection can be avoided for small cancers with clinically node-negative, sentinel node (SN)-positive disease, provided that systemic therapy and whole-breast irradiation (WBI) are incorporated into the treatment strategy for early-stage breast cancer following breast-conserving surgery (BCS).
👉This trial took clinically node-negative patients with 1 to 2 positive SNs by hematoxylin and eosin staining who were treated with BCS and whole-breast irradiation and assigned them into 1 of 2 arms:
👉One that received completion ALND versus the other that received only SLNB.
👉The 10-year overall survival in the SLNB only group versus the completion ALND group was 86.3% and 83.6%, respectively.
👉Similarly, disease-free survival was 80.2% and 78.2%, respectively.
👉The study demonstrated that the 10-year in-breast recurrence rate was higher in the ALND group, 5.6% versus 3.8% (P=0.13) than in the sentinel lymph node resection only group.
👉Regional recurrence occurred in less than 1.5% of patients in both arms.
REFERENCES
Giuliano AE, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial.Ann Surg. 2010;252:426-432.
👉The EORTC Trial 10801 was a randomized multicenter trial that compared breast-conserving therapy with MRM for patients with invasive breast cancer less than 5 cm in diameter.
👉At 10 years, there was no difference between the two groups in OS or in distant metastasis-free rates.
👉Locoregional recurrence at 10 years was 12% for the mastectomy group and 20% for the breast-conserving therapy group.