My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
A Phase III Randomized Study of Postoperative Radiotherapy Following Segmental Mastectomy and Axillary Dissection in Patients with Noninvasive Intraductal Adenocarcinoma of the Breast:
Compared:
Lumpectomy alone to
Lumpectomy plus breast radiation
818 patients with localized ductal carcinoma in situ (DCIS)
This trial concluded that:
Radiotherapy significantly decreases the rate of invasive cancer and DCIS in the ipsilateral breast:
By approximately 50%
NSABP B-32:
Was a randomized controlled phase III trial conducted at 80 centers in Canada and the U.S:
5611 women with invasive breast cancer were randomly assigned to either:
Sentinel lymph node (SLN) resection plus ALND (group 1) or
To SLN resection alone with ALND:
Only if the SLNs were positive (group 2)
In the 3986 SLN-negative patients:
8-year estimates for:
Overall survival:
Were 91.8% (95% CI, 90.4%–93.3%) in the first group and
90.3% (88.8%–91.8%) in the second group
Treatment comparisons for disease-free survival:
Yielded an unadjusted HR of 1.05 (95% CI, 0.90–1.22; P=0.54)
Disease-specific survival was:
82.4% (80.5%–84.4%) in group 1 and
81.5% (79.6%–83.4%) in group 2
There were eight regional node recurrences as first events in group 1 and 14 in group 2 (P=0.22)
Patients are continuing follow-up for long-term assessment of survival and regional control
NSABP protocol B-43:
Aims to evaluate the effect of trastuzumab in HER2-positive DCIS
Patients with HER2-positive DCIS treated with BCS were randomized to:
Breast radiation alone versus
Breast radiation plus two doses of trastuzumab:
Starting on day 1 of breast radiation and repeated 3 weeks later
The primary endpoint:
Is the development of any breast cancer
REFERENCES
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233-1241.
Fisher B, Dignam J, Wolmark N, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998;16:441-452.
Fisher B, Montague E, Redmond C. Comparison of radical mastectomy with alternative treatments for primary breast cancer: a first report of results from a prospective randomized clinical trial. Cancer. 1977;39:2827-2839.
Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomized phase 3 trial. Lancet Oncol. 2010;11:927-933.
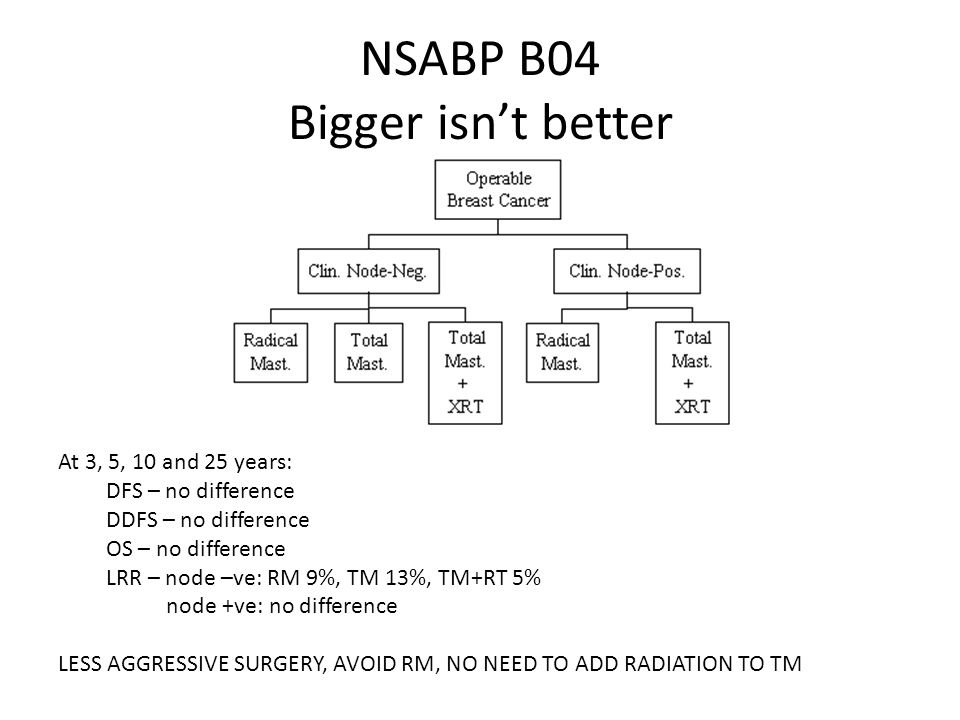
A Protocol for the Evaluation of Radical Mastectomy (RM) and Total Mastectomy (TM) With and Without Radiation in the Primary Treatment of Cancer of the Female Breast:
Enrolled 1079 patients with clinically node-negative disease
And randomized them to:
RM
TM plus local-regional axillary radiation
TM alone
In parallel:
586 patients with clinically node-positive disease:
Were randomized to:
RM
TM plus radiation
After 25 years of follow-up:
The study failed to demonstrate a significant difference:
In long-term outcome between:
Clinically node-negative patients:
Who received RM and those who received TM plus radiation, or
Between clinically node-positive patients:
Who received RM and those who received TM with nodal radiation
Patients with COVID-19 generally present with respiratory symptoms:
More specifically:
Cough:
46% to 82% of the cases
Shortness of breath:
20% to 64% of the cases
Upper respiratory tract symptoms:
5% to 25% of the cases:
Including nasal / sinus congestion
The Brigham and Women’s Hospital guidelines further state that:
Approximately 20% of those with COVID-19 develop ARDS
2% to 25% have a respiratory viral co-infection
The most common cause of ICU admission for COVID-19 patients is:
Hypoxemic respiratory failure
Among those admitted:
Intubation is often required within 12 to 24 hours
Of COVID-19 patients who die:
About half die from respiratory failure
Third die from concomitant respiratory and heart failure
Many patients with COVID-19 are presenting with:
Hypoxemia disproportionate:
To their imaging findings
Hypoxemia arises in ARDS:
Through a mismatch of ventilation and perfusion:
Predominantly due to shunt:
1 to 3 with shunt fractions much greater than would be anticipated for their relatively compliant lungs
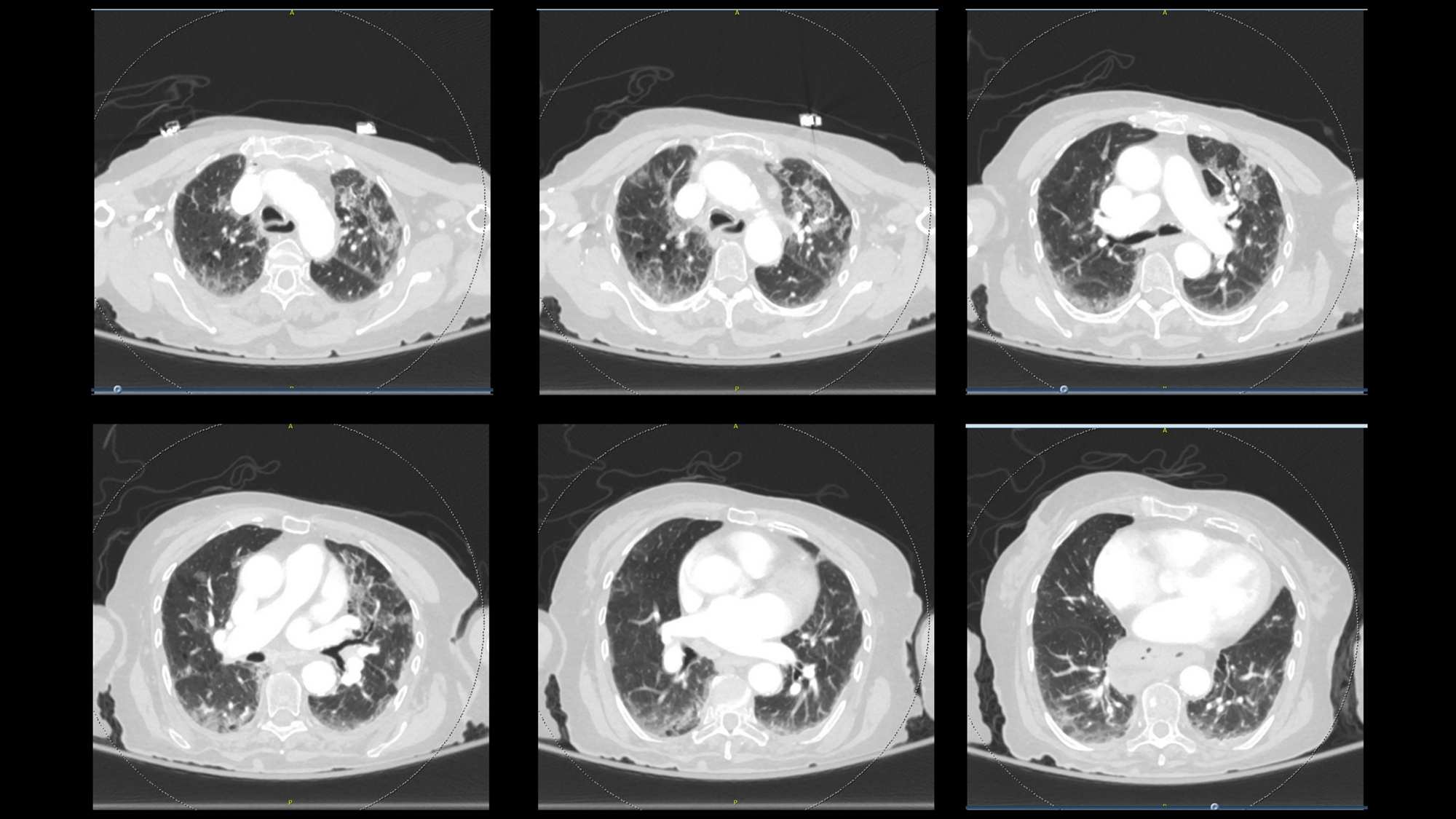
Patients with COVID-19 have:
Scattered, peripheral ground glass opacities on chest computed tomography scans:
Indicating ineffective lung units, and as such:
Shunt:
Appears to be a major cause of the hypoxemia
Dr. Gattioni and colleagues report:
Disproportionate blood flow to these areas:
Possibly accounting for the profound hypoxemia
They suggest at least two distinct phenotypes:
Low recruitability phenotype:
Presenting with:
Low elastance
High compliance
Low recruitability
But yet substantial hypoxemia:
They hypothesis that a mechanism for this profound hypoxemia could be:
Loss of V/Q matching from:
Pulmonary arterial vasoplegia
Later, patients progressed to the H phenotype:
High elastance
Low compliance
High recruitability
Need for higher PEEP
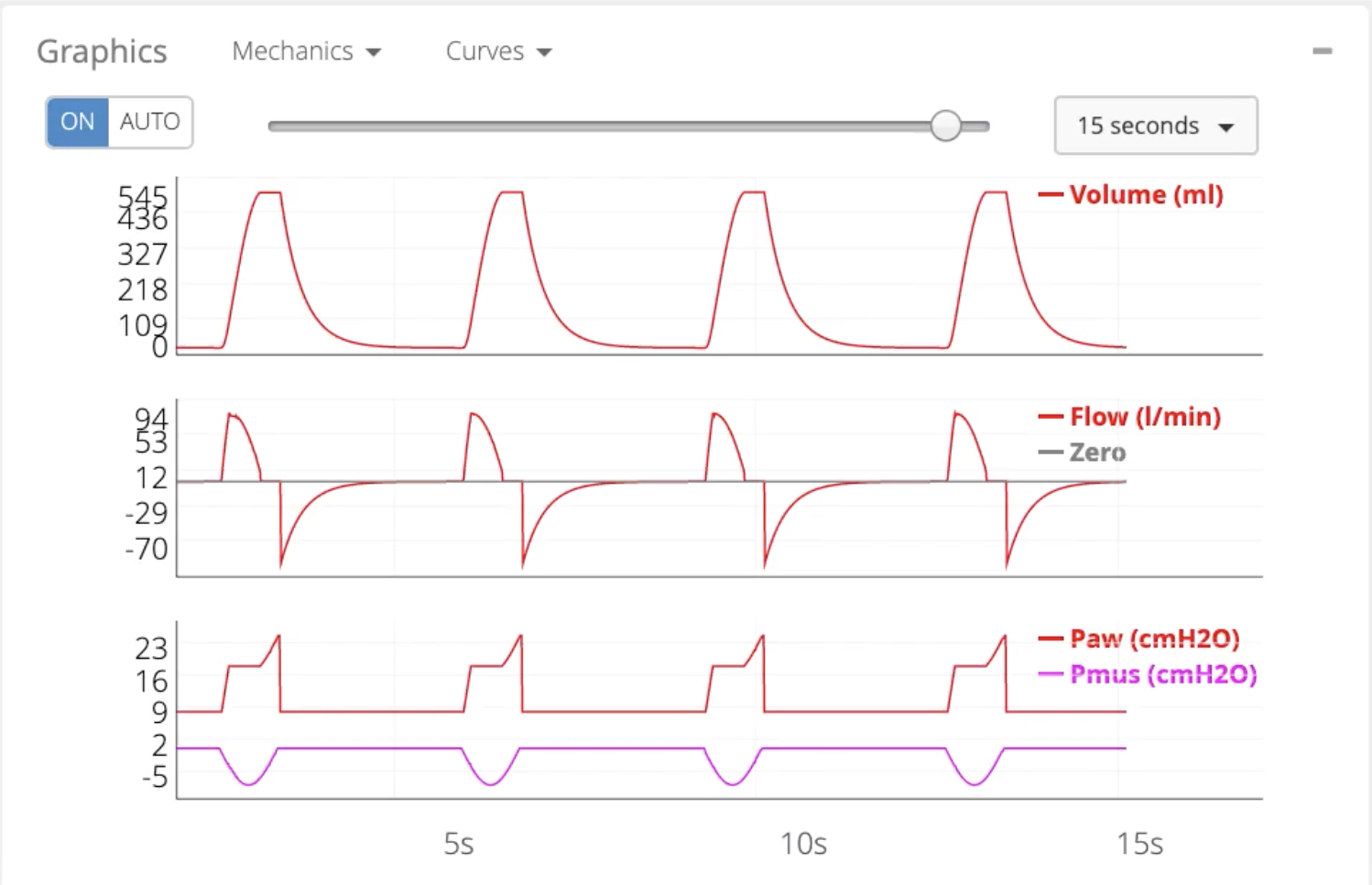
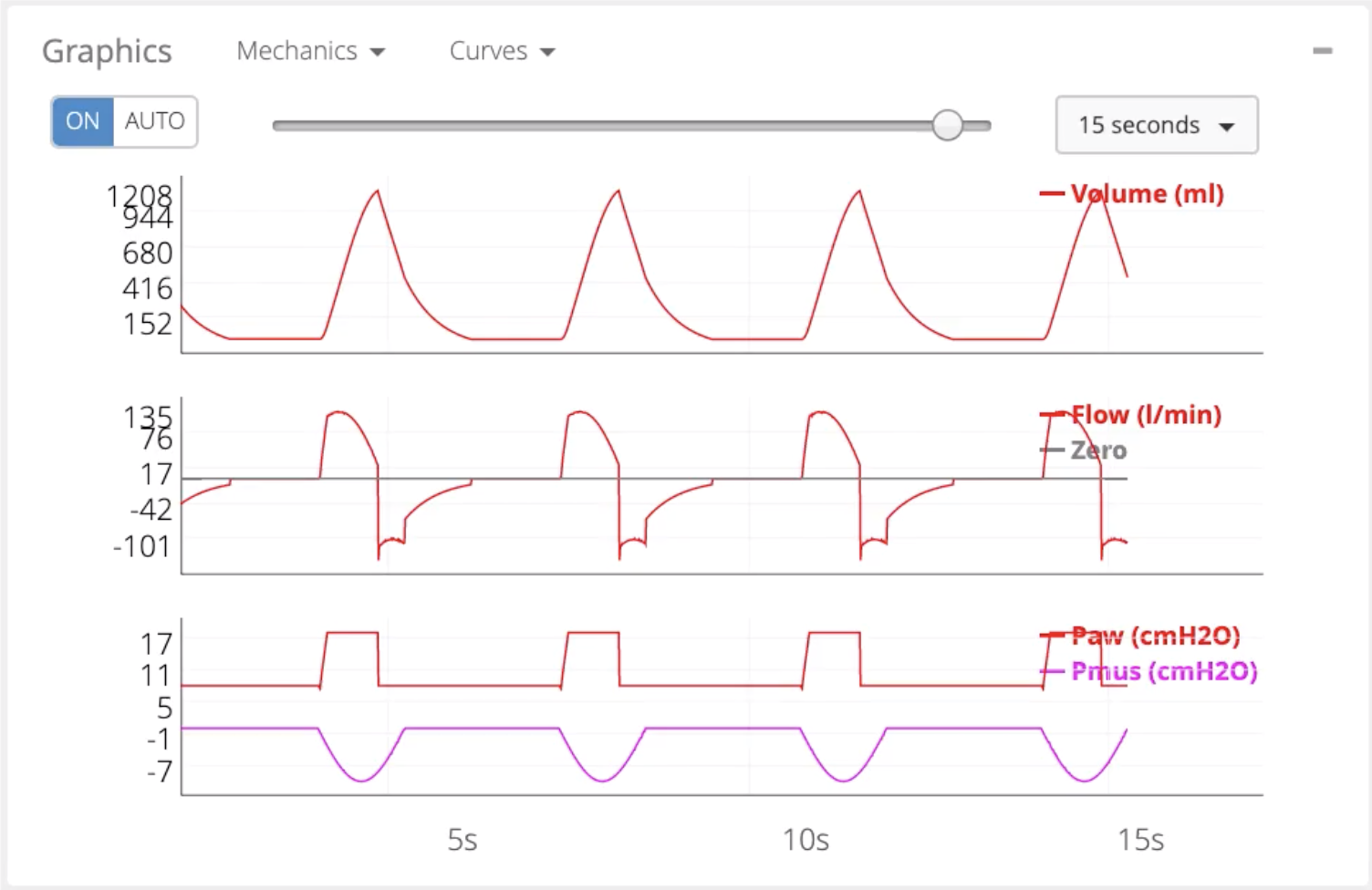
The CT scan below demonstrates the mild-moderate ground glass findings in COVID-19:
On presentation:
Patients are presenting with substantial hypoxemia:
With many having oxygen saturations in the 70s, 80s, 90s:
They deteriorate with any exertion
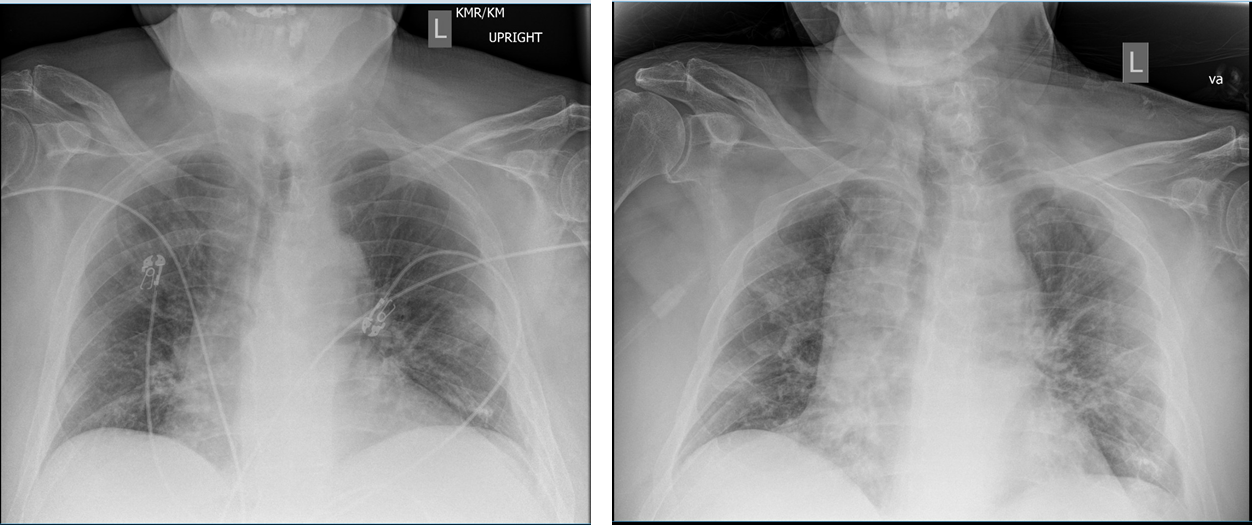
Chest x-ray imaging will vary substantially depending upon where the patient is in the course of their illness
The initial mode of treatment involves:
Providing supplemental oxygen immediately to improve the oxygen saturation
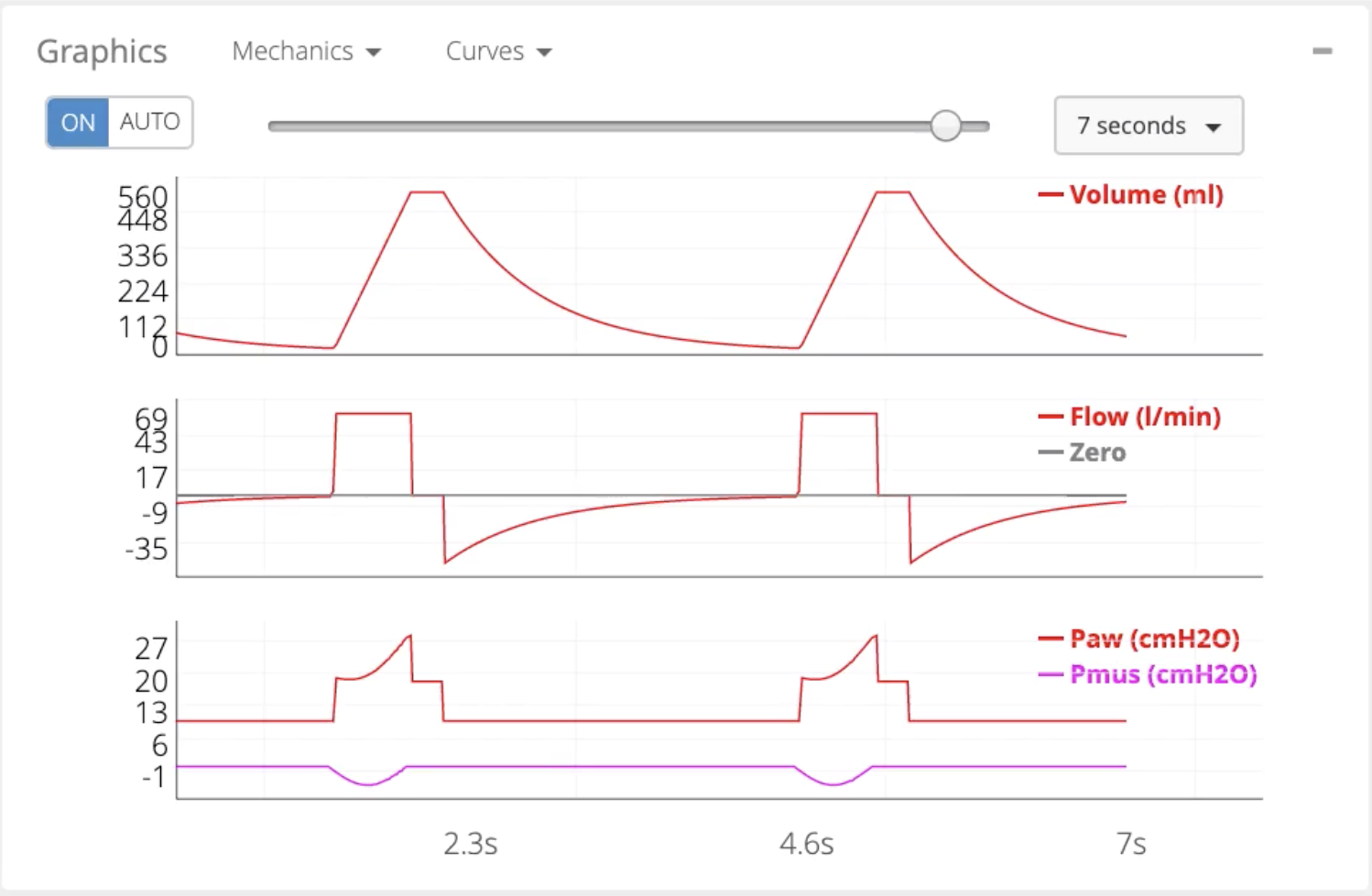
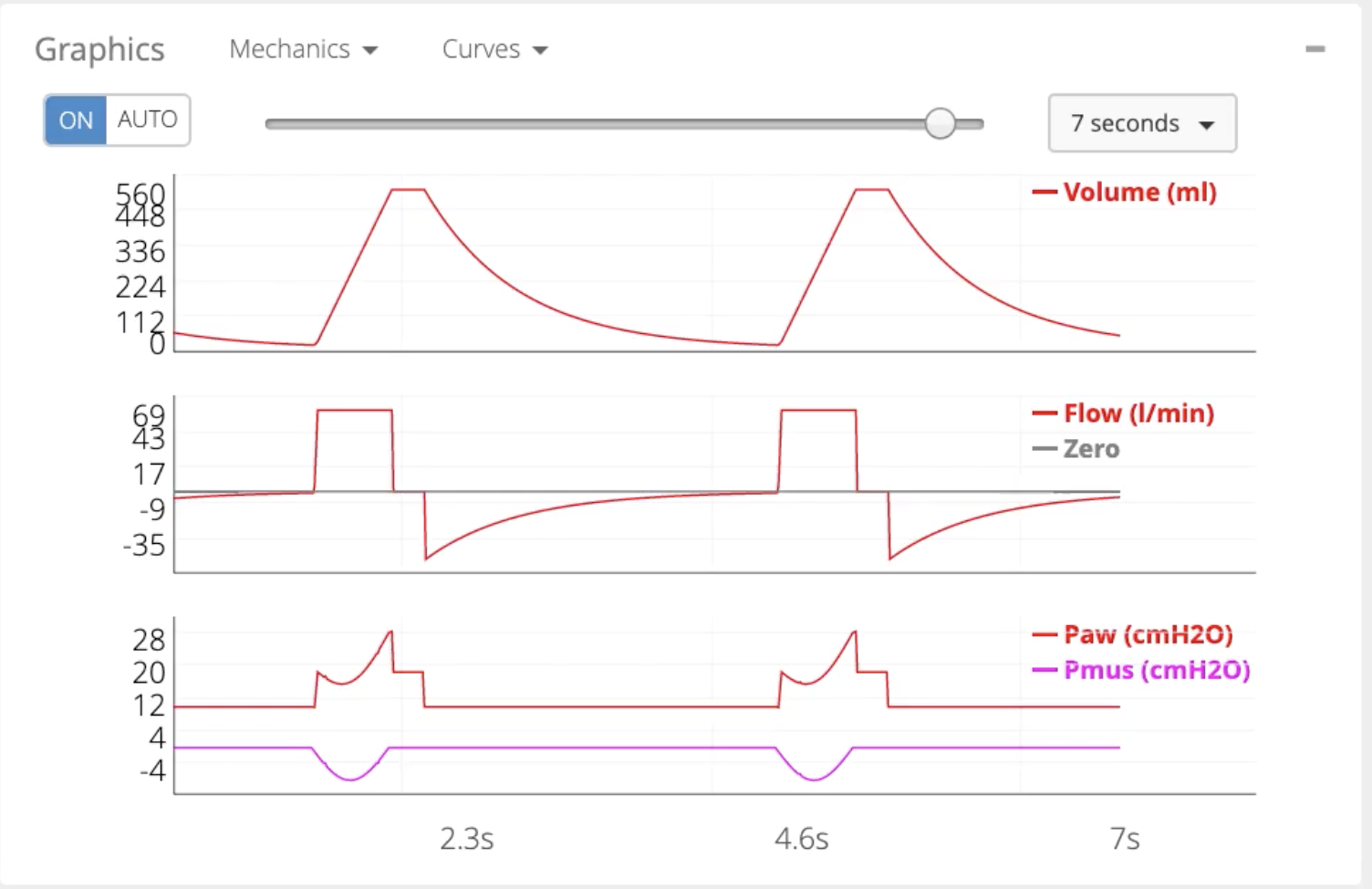
Although patients may or may not be complaining of dyspnea:
Nearly all hypoxemic patients are noted to be tachypneic:
Patients who are tachypneic:
Generate largetidal volumes:
Which can induce lung injury:
From generating large negative intrathoracic pressure and therefore a large transpulmonary pressure
As such, the hypoxemia should be treated to:
Decrease hypoxemic drive
The role of high-flow nasal cannula and non-invasive positive pressure ventilation:
Are controversial in COVID-19:
The concerns are for healthcare workers, as the risk of aerosolization has been noted with these modalities, especially non-invasive positive pressure ventilation
Although there are limited data regarding the use of HNFC in COVID-19:
A small study of patients with Influenza A showed that 45% avoided intubation:
Although all more severe patients were eventually intubated
Similarly, non-invasive positive pressure ventilation (NIPPV) is a common means of respiratory support in many patients:
But its use in COVID-19 should be limited
NIPPV failed in 57% to 85% of patients with Influenza A H1N1 associated ARDS:
With failing patients having a higher ICU mortality than those treated with invasive mechanical ventilation
Some component of this may be due to patients continuing to:
Generate those large tidal volumes
Continuing to induce self-inflicted lung injury
Subjects with SOFA score ≥ 5 had a higher risk of NIV failure (odds ratio = 3.3, 95% CI 2.4-4.5)
A small study of COVID-19 patients in Wuhan found that 76% failed NIPPV, and the mortality rates were similarly high for both groups
NIPPV also aerosolizes the virus:
Many recommend that it should be avoided in most circumstances:
However, there may well be a role for judicious use of non-invasive ventilation in COVID-19
Each institution is developing their own policies and procedures, with some adopting the process widely and others not using it at all
When the decision is made to intubate a patient:
The patient can have significant clinical deterioration with COVID-19
The patient arrives with a high work of breathing:
The induction agents and paralytics are administered, the patient is laid in a recumbent position, and the patient will be derecruited
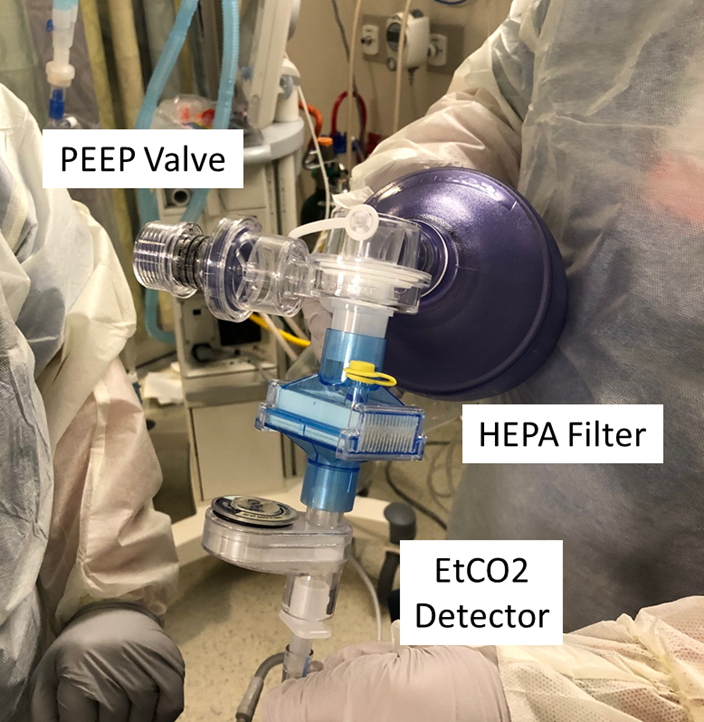
Recruiting the patient can be a substantial endeavor:
Typically, we use a bag method with a PEEP valve to recruit patients and prepare them to be placed on the ventilator immediately after intubation:
If this method is to be used, a HEPA filter must be placed between the endotracheal tube and the bag:
However, many institutions are now foregoing any bagging and instead placing the patient directly on the ventilator:
To reduce the risk of aerosolization
An advantage is:
That the patient does not receive any:
High tidal volume, high-pressure breaths from the bagging
The downside, however, is:
That recruitment may take longer, and these patients may be profoundly hypoxemic during that time period
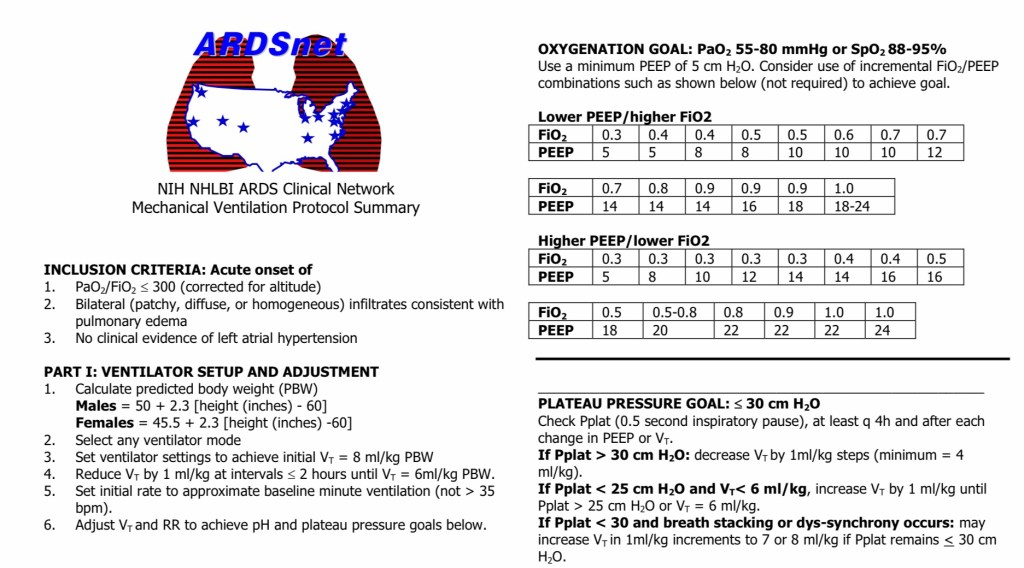
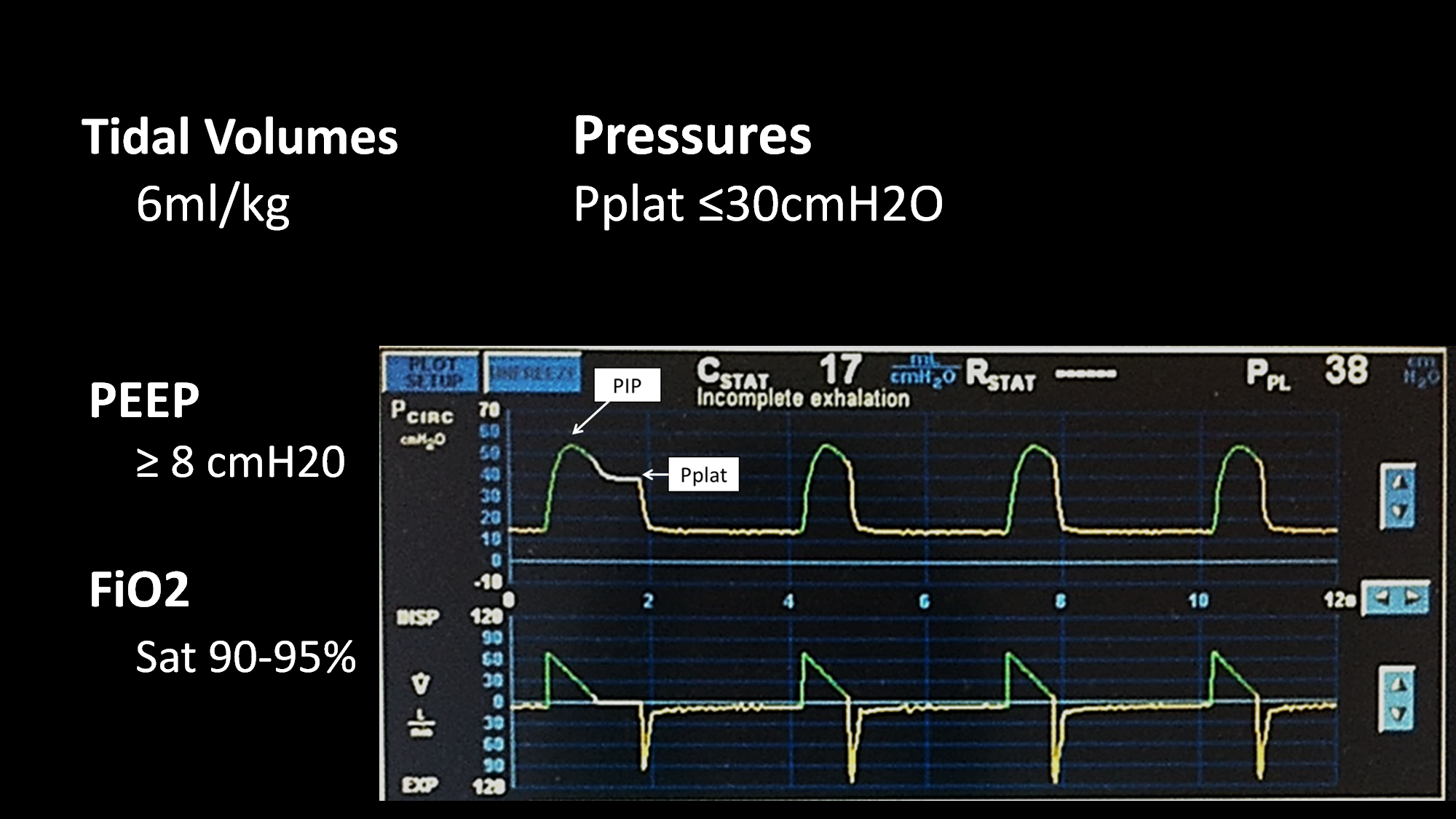
Once the patient is placed on the ventilator, general principles of good ventilator management still apply:
The patient should be placed on:
Low tidal volume ventilation:
4 ml/kg to 8 ml/kg of PBW:
Starting with a tidal volume of 6 ml/kg of predicted body weight
The plateau pressure should be checked and monitored:
Ensuring a value less than 30 cm of water
The driving pressure should be:
Less than 15 centimeters of water
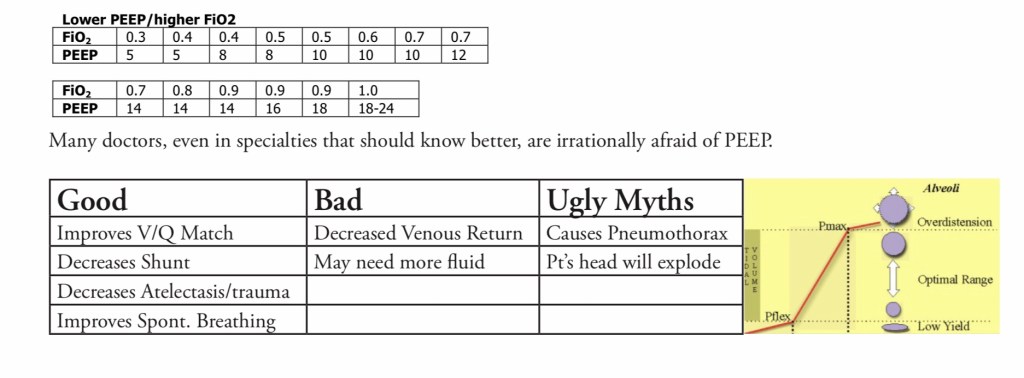
These patients likely require a moderate PEEP at least:
We recommend starting with a PEEP of 8 and adjusting from there:
While PEEP can improve oxygenation:
Too much PEEP can be deleterious causing:
Increased intrathoracic pressure
Lung injury
Hemodynamic compromise if severe
For patients with COVID-19:
Who have a PaO2 / FiO2 ratio of less than a 150:
The next step should be placing the patient:
In a prone position:
Many institutions have protocols or guidelines for prone positioning
Prone positioning has been shown to improve mortality in patients with ARDS:
Authors are reporting good outcomes with proning in patients with COVID-19
Although a simple procedure, it requires a systems-based approach, with investment from nurses, respiratory therapists, and physicians alike
All attention must be on the patient’s endotracheal tube, invasive lines, and position during the turns
Additionally, close attention must be paid to patients in a prone position to ensure that their orbits and eyes are protected, that pressure points are well-supported, that medical equipment is not trapped under the body, possibly causing opportunity for injury or bedsores
Most protocols involve:
Leaving the patient in the prone position for 12 to 16 hours
The patient will be reproned as long as their PaO2/ Fi02 ratio remains:
Less than 150 while they are supine
When the patient’s PaO2/ FiO2 ratio starts to improve:
The patient no longer requires routine proning
For patients with persistent severe hypoxemia:
Inhaled pulmonary vasodilators:
Can be considered
Inhaled epoprostenol is an excellent pulmonary vasodilator:
However, it is not recommended in COVID-19 as it mandates frequent ventilator circuit changes
Therefore, if an inhaled pulmonary vasodilator is needed:
Inhaled nitric oxide is preferred:
We start at 20 parts per million and assess the patient for an improvement in SpO2
If the patient does not have at least a 20% improvement in the SpO2:
The inhaled pulmonary vasodilator is unlikely to be effective and should not be continued
If the patient is responsive, the pulmonary vasodilator can be continued with gradual weaning as a patient improves clinically over the next several days
Bacterial superinfection:
Has been noted in about 20% to 30% of patients with COVID-19, and as such:
Many patients will require antibiotics
Procalcitonin can be useful for assessing COVID-19 alone
Steroids are not routinely recommended for COVID-19 treatment:
However, patients who have another indication for steroids:
Such as asthma or adrenal insufficiency:
They should receive them
The surviving sepsis campaign recommends use of steroids in severe ARDS:
However, this is not a universal recommendation
The role of other medications including:
Hydroxychloroquine, azithromycin, and statins:
Are unclear
We encourage everyone to refer to local protocols for guidance on the use of these medications
Some medications, such as Remdesivir, are being evaluated in clinical trials
Although CT scans:
Have been shown to be fairly sensitive for the diagnosis of COVID-19:
Once the diagnosis is made:
We do not encourage the routine use of CT scans:
Not only does a CT scan pose risk to a critically ill patient, mandating travel with the associated risks of line pulls, hemodynamic instability, and hypoxemia, but this can lead to infection control issues mandating the cleaning of the scanners as well
Patients with COVID-19:
Have been noted to be fairly hypercoagulable:
With many authors reporting:
Thromboembolic disease, clotting of dialysis lines, and other clinical manifestations of hypercoagulability:
D-dimer levels can be quite elevated coming into the thousands
The best practices for initiation of therapeutic anticoagulation:
In the absence of a documented thromboembolism:
Are unclear at this time:
Some clinicians are using markedly elevated D-dimer levels:
Such as greater than 2000:
As an indication for anticoagulation, whereas others are basing it upon clotting of lines and other clinical markers
Bronchoscopy is an aerosolizing procedure and as such:
Should be minimized or avoided in patients with COVID-19
Additionally, suctioning can be aerosolizing and all healthcare workers in the room should be aware and in appropriate PPE before these procedures are performed
The risk of distant recurrence and the potential benefit of adjuvant chemotherapy
Retrospective analyses of tissue samples from prospective, randomized trials:
Showed that the score estimates:
The risk of distant recurrence and predicts the benefit from adjuvant chemotherapy
The TAILORx trial was designed to determine:;
Whether Oncotype DX could be used prospectively:
To guide decision making regarding the use of adjuvant chemotherapy:
In node-negative, hormone receptor-positive breast cancers:
With an intermediate recurrence score:
A group where the benefit of chemotherapy is less clear:
The intermediate score for purposes of the trial was defined as 11 to 25
All patients were treated with hormonal therapy
Patients with scores of less than 11:
Were treated with hormonal therapy alone
Those with scores above 25:
Were treated with chemotherapy plus hormonal therapy
Patients with intermediate scores (11 to 25):
Were randomized to receive chemotherapy or not
Primary endpoints of the trial:
Are disease-free survival and overall survival
Methods:
Eligibility criteria included:
Women 18 to 75 years of age
HR-positive
HER2-negative
Axillary node (AN)-negative breast cancer
Tumors 1.1 to 5.0 cm in size:
Or 0.6 to 1.0 cm and intermediate grade to high grade
Agreed to have chemotherapy assigned or randomized based on the RS
Women with a mid-range RS (11 to 25):
Were randomized to receive:
Endocrine therapy (ET) or
Chemotherapy and endocrine therapy (CET)
The primary endpoint was:
Invasive disease-free survival (iDFS),
The trial was designed to show non-inferiority for ET alone by not rejecting equality:
Hazard ratio [HR] margin up to 1.322 for omission of chemotherapy, 1-sided type I error rate 10%, type II error rate 5%
The target sample size was adjusted to compensate for non-adherence to randomized treatment, and the protocol-specified final analysis was triggered after 835 iDFS events
Results:
Of the 10,253 eligible women enrolled between 4/7/06-10/6/10:
6711 (65.5%) had a:
RS of 11 to 25 and adequate information
There were 836 iDFS events at final analysis:
With amedian followup of 90 months
ET was non-inferior to CET for iDFS:
HR 1.08, 95% confidence intervals [CI] 0.94, 1.24, p=0.26) in the intention-to-treat (ITT) population
ET was also non-inferior for distant recurrence-free interval:
DRFI:
HR 1.03, p=0.80
ET was also non-inferior for recurrence-free interval:
RFI:
HR 1.12, p=0.28
ET was also non-inferior for overall survival:
OS:
HR 0.97, p=0.80
Nine year rates were similar for:
iDFS:
83.3% vs. 84.3%
DRFI:
94.5% vs. 95.0%
RFI:
92.2% vs. 92.9%
OS:
93.9% vs. 93.8%
Recurrence:
Accounted for 338 (41.6%) the first iDFS event:
Of which 199 (23.8%) were distant recurrences
Treatment interaction tests were significant for age (iDFS p=0.03; RFI p= 0.02), but not menopause, tumor size, grade, or RS (continuous or RS 11-15, 16-20, 21-25).
Conclusions:
In women with HR-positive, HER2-negative, AN-negative breast cancer and a RS of 11 to 25:
Adjuvant ET was not inferior to CET in the ITT analysis:
Solin LJ. The Eastern Cooperative Oncology (ECOG) experience. In: Kuerer HM, ed. Kuerer’s Breast Surgical Oncology. New York, NY: McGraw-Hill Companies; 2010:578-581.
National Cancer Institute at the National Institutes of Health Web site. Featured Clinical Trials. Phase III Randomized Study of Adjuvant Combination Chemotherapy and Hormonal Therapy Versus Adjuvant Hormonal Therapy in Women with Previously Resected Axillary Node-Negative Breast Cancer with Various Levels of Risk for Recurrence (TAILORxTrial) (ECOG-PACCT-1). Available at: clinicaltrials.gov/ct2/show?term=TAILORx&rank=1.
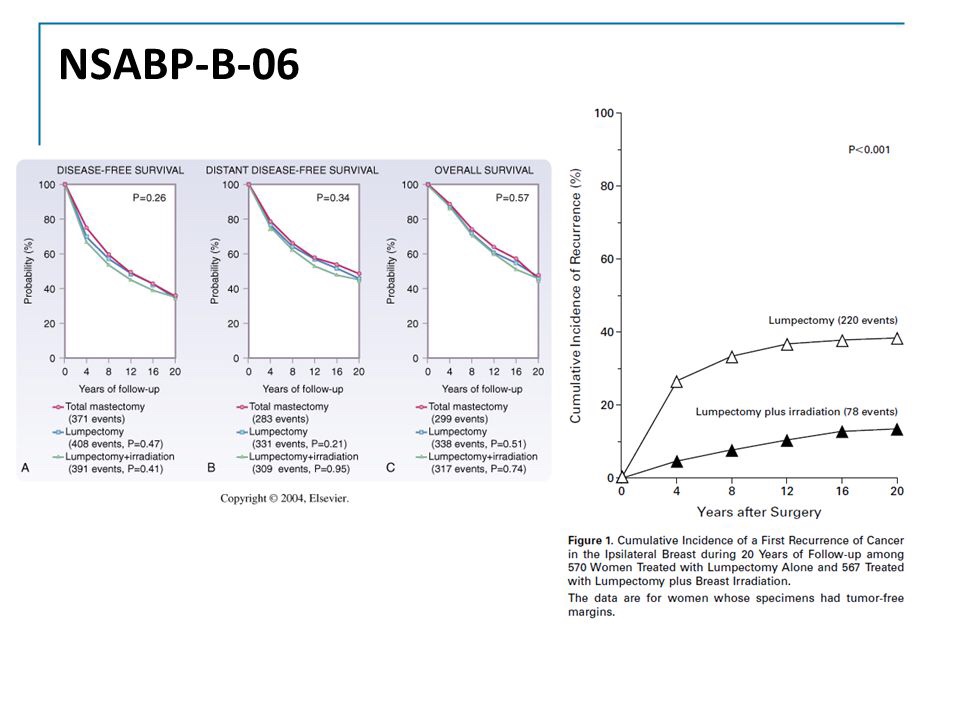
Phase III trial of Total Mastectomy/Axillary Dissection vs Segmental Mastectomy/Axillary Dissection with or without Radiotherapy for Potentially Curable Breast Carcinoma:
Compared lumpectomy and ALND with or without breast radiation with MRM:
In patients with tumors 4 cm or less in greatest diameter
This trial, along with other trials, was instrumental in establishing:
BCS plus radiation therapy:
As the preferred treatment of operable breast cancer:
As compared to mastectomy
After 20 years of follow-up:
There are no observed differences in:
Overall survival
Distant disease-free survival:
Between the MRM group and the groups treated with BCS, with or without radiation
The hazard ratio (HR) for death with BCS alone was:
In the past, patients with positive sentinel nodes have generally been treated with:
Axillary lymph node dissection (ALND)
Side effects of ALND include:
Lymphedema:
In up to 40% of patients
The AMAROS trial:
Is a phase III prospective, multicenter non-inferiority study:
Comparing ALND with axillary radiotherapy (ART)
The primary objective of the trial:
Is to prove equivalent locoregional control:
With reduced morbidity for ART
The SN detection rate:
With radioactive tracer and blue dye combined:
Was 97%
The two treatment arms were comparable:
With regard to age, tumor type, tumor size, grade, and adjuvant therapy
Both ALND and ART after a positive sentinel node biopsy:
Provided excellent and comparable regional control
Median follow-up of 6.1 years
The 5-year axillary recurrence rate was:
0.54% after ALND and
1.03% after ART
The axillary recurrence rate:
After a negative sentinel node biopsy:
was 0.8%
There were no significant differences between treatment arms:
With respect to overall survival:
93.27% ALND
92.52% ART
P=0.3386
Disease-free survival:
86.90% ALND
82.65% ART
P=0.1788
Lymphedema:
Was found significantly more often after ALND than ART:
Patient perceived (subjective) lymphedema:
23% versus 11%
Measured (objective):
13% versus 6% after 5 years of follow-up
P<0.0001
REFERENCES
Rutgers EJ, Donker M, Straver ME, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer patients: final analysis of the EORTC AMAROS trial (10981/22023). J Clin Oncol. 2013;31 (suppl; abstr LBA1001). http://meetinglibrary.asco.org/content/109779-132. Accessed November 7, 2013.
Straver ME, Meijnen P, Tienhoven GV, et al. Sentinel node identification rate and nodal involvement in the EORTC 10981-22023 AMAROS trial. Ann Surg Oncol. 2010;17:1854-1861.