My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
T0 – No tumor identified, but EBV-positive cervical node(s) involvement
T1 – Tumor confined to nasopharynx, or extension to oropharynx and/or nasal cavity without parapharyngeal involvement
T2 – Tumor with extension to parapharyngeal space, and/or adjacent soft tissue involvement (medial pterygoid, lateral pterygoid, prevertebral muscles)
T3 – Tumor with infiltration of bony structures at skull base, cervical vertebra, pterygoid structures, and/or paranasal sinuses
T4 – Tumor with intracranial extension, involvement of cranial nerves, hypopharynx, orbit, parotid gland, and/ or extensive soft tissue infiltration beyond the lateral surface of the lateral pterygoid muscle
N1 – Unilateral metastasis in cervical lymph node(s) and/ or unilateral or bilateral metastasis in retropharyngeal lymph node(s), 6 cm or smaller in greatest dimension, above the caudal border of cricoid cartilage
N2 – Bilateral metastasis in cervical lymph node(s), 6 cm or smaller in greatest dimension, above the caudal border of cricoid cartilage
N3 – Unilateral or bilateral metastasis in cervical lymph node(s), larger than 6 cm in greatest dimensión, and/ or extension below the caudal border of cricoid cartilage
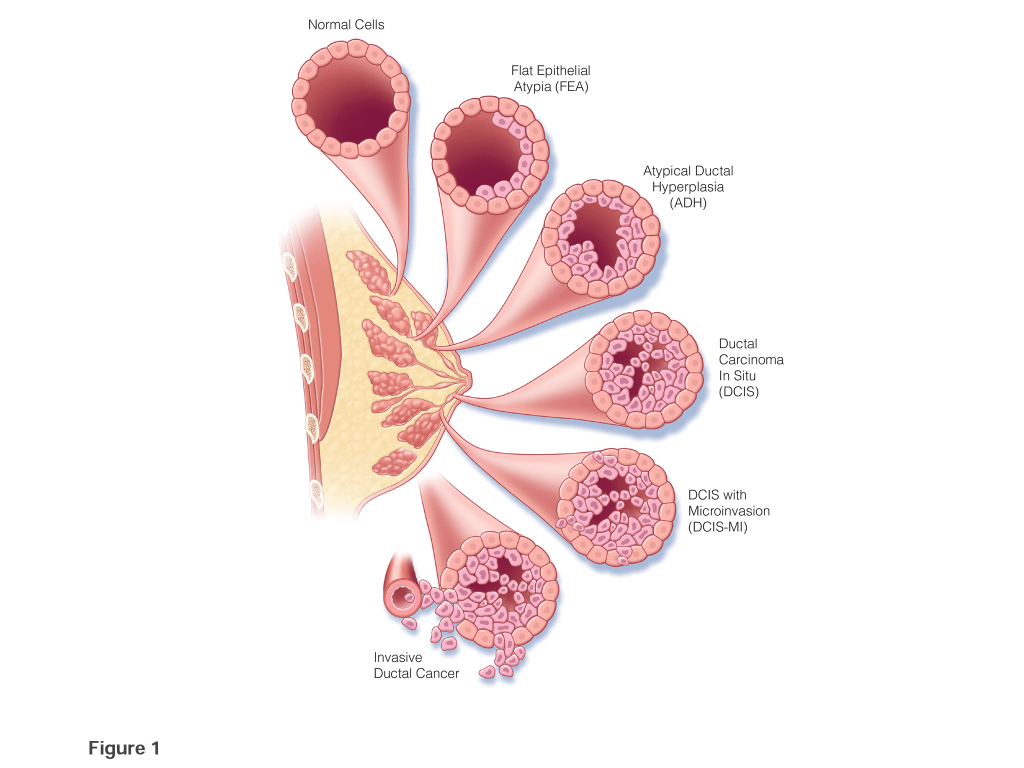
Ductal carcinoma in situ (DCIS) is a malignant intra-ductal proliferation of epithelial cells within the tubular-lobular system of the breast with no microscopic evidence of permeation across the basement membrane. There appears to be a progression between flat epithelial atypia, atypical ductal hyperplasia (ADH), and DCIS, in which DCIS is final step prior to the development of invasive disease. The clinical risk factors and molecular alterations related with malignant transformation are very similar between DCIS and invasive cancer. The concurrence of DCIS and invasive carcinoma within one lesion suggests that DCIS is a precursor lesion to invasive carcinoma. Evidence of the ability of DCIS to progress is that 50% of all recurrences after breast-conserving surgery (BCS) for DCIS, with or without adjuvant treatment, are invasive.
Data is sparse on the natural history of DCIS, but some series have reported the outcomes for women many years after undergoing a surgical biopsy that was interpreted as benign that contained an unrecognized area of DCIS (1–4). These data identified that approximately 20% to 53% of these women developed ipsilateral invasive carcinoma. Sanders et al. reported on 28 women with unrecognized low-grade DCIS in the surgical biopsy specimen, of which 11 developed invasive carcinoma, all of these cancers developed in the same breast and quadrant as the biopsy containing the DCIS (1). The vast majority of these invasive cancers developed within 10 years, but three were diagnosed after 20 years.
Collins et al, in the Nurses’ Health Study, singled out 13 women who were found to have DCIS on reexamination of the surgical biopsies that were previously diagnosed as benign (2). Ten of these women subsequently developed breast cancer; all were ipsilateral, four were DCIS and six were invasive (2). The interval between the biopsy and the progression to invasive cancer was on average nine years.
Approximately one in eight women (i.e., 12%) in the United States (US) will be diagnosed with breast cancer in her lifetime, and 20% to 25% of these newly diagnosed cases will be DCIS (Siegel 2015, CA Cancer J Clin). In 2020, an estimated 48,530 cases of DCIS will be diagnosed in US (American Cancer Society: Cancer Facts and Figures 2020. Atlanta, Ga: American Cancer Society, 2020. Available onlineExit Disclaimer. Last accessed January 17, 2020).
Universal screening mammography has resulted in a 10-fold increase in the incidence of DCIS since the mid-1980s, but since 2003, the incidence of DCIS has decreased in women age 50 years and older, conceivably secondary to decline in the use of hormone replacement therapy, while the incidence in women under 50 continues to increase (Altekruse SF, Kosary CL, Krapcho M, et al.: SEER Cancer Statistics Review, 1975-2007. Bethesda, Md: National Cancer Institute, 2010. Also available online. Last accessed April 3, 2020). Roughly one in every 1,300 mammograms performed in US will lead to a diagnosis of DCIS, representing 17% to 34% of all mammographically detected breast cancers. Before the institution of widespread screening mammography in the mid-1980s, most of the cases of DCIS were not identified until a palpable tumor developed, but today, 80% to 85% of DCIS cases are screen detected.
The incidence of DCIS in necropsy studies is higher than in the general population, proposing that not all DCIS lesions become clinically significant and supporting concerns that most of the increase in DCIS incidence is due to the detection of non-aggressive subtypes that are unlikely to progress to invasive cancer.
Most women with DCIS are diagnosed at a median age that ranges from 47 to 63 years, similar to that reported for patients with invasive carcinoma. However, the age of peak incidence for DCIS (96.7 per 100,000 women), occurs between the ages of 65 and 69 years, which is younger than that for invasive breast cancer, for which peak incidence (453.1 per 100,000 women), occurs between the ages of 75 and 79 years.
The incidence of first-degree relative having breast cancer (i.e., 10% to 35%) as well as rates of deleterious mutations in the breast cancer associated (BRCA) genes are similar for patients with DCIS as for women with invasive breast cancer. Other risk factors for DCIS include: older age, proliferative breast disease, increased breast density, nulliparity, older age at primiparity, history of breast biopsy, early menarche, late menopause, long-term use of postmenopausal hormone replacement therapy, and elevated body mass index in postmenopausal women, are the same as those for invasive breast cancer, but in many cases, the relationship between a given characteristic and invasive cancer is stronger than the relationship between that characteristic and DCIS.
T1 – Tumor limited to one subsite of hypopharynx and / or 2 cm or smaller in greatest dimensión
T2 – Tumor invades more than one subsite of hypopharynx or an adjacent site, or measures larger than 2 cm but not larger than 4 cm in greatest dimensión without fixation of hemilarynx
T3 – Tumor larger than 4 cm in greatest dimensión or with fixation of hemilarynx or extension to esophagus
T4 – Moderately advanced and very advanced local disease
T4a – Moderately advanced local disease
Tumor invades thyroid/cricoid cartilage, hyoid bone, thyroid gland, or central compartment soft tissue
Significantly increased rates of pCR were observed in HER2+ patients:
Treated with trastuzumab in combination with chemotherapy versus chemotherapy alone
In an initial:
Small trial conducted by Buzdar and colleagues:
The increase in pCR rates when trastuzumab was combined with chemotherapy:
Was so dramatic:
65.2% vs 26.3%
p=.016:
That the study was terminated early by the data safety monitoring board
Other trials have investigated dual HER2 targeting:
In the neoadjuvant setting:
With each regimen having different mechanisms of action and toxicity
The NeoSphere study:
Was a randomized multicenter phase II trial:
Investigating the addition of pertuzumab to trastuzumab:
With or without docetaxel
In patients that received dual HER2-targeting therapy in combination with chemotherapy:
There was almost a doubling of the pCR rates in the breast compared to patients that received trastuzumab and chemotherapy alone:
46% vs 29%
p=.014
In the treatment arm that received dual HER2-targeted therapy without any chemotherapy:
The pCR rate:
In the breast was 17% and in the axilla was 11%:
Suggesting some patients may benefit from HER2-directed therapy alone, without chemotherapy
Both the CHER-LOB and Tryphaena trials:
Show the addition of an anthracycline to dual HER2 blockade:
Further improves pCR rates
To date:
Physical exam and imaging (any imaging):
Are unable to confirm achievement of a pCR:
Therefore, all patients are advised to undergo surgery:
There is interest in conducting clinical trials to evaluate MRI with biopsy of the tumor site:
To identify patients who may be watched after achieving a complete response to neoadjuvant chemotherapy plus HER2-targeted therapy
Recent single institution data:
Suggest the response to neoadjuvant chemotherapy:
May vary according to location:
With the axilla demonstrating higher pCR rates than the breast:
In all tumor subtypes.
References:
Buzdar AU, Ibrahim NK, Francis D, et al. Significantly higher pathologic complete remission rate after neoadjuvant therapy with trastuzumab, paclitaxel and epirubicin chemotherapy: results of a randomized trial in human epidermal growth factor receptor 2-positive operable breast cancer. J Clin Oncol. 2005;23(16):3676-3685.
Untch M, Rezai M, Loibl S, et al. Neoadjuvant treatment with trastuzumab in HER2-positive breast cancer: results from the GeparQuattro study. J Clin Oncol. 2010;28(12): 2024-2031.
Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomized controlled superiority trial with a parallel HER2-negative cohort. Lancet. 2010;375(9712):377-384.
Untch M, Fasching PA, Konecny GE, et al. Pathologic complete response after neoadjuvant chemotherapy plus trastuzumab predicts favorable survival in human epidermal growth factor receptor 2-overexpressing breast cancer: results from the TECHNO trial of the AGO and GBG study groups. J Clin Oncol. 2011;29(25):3351-3357.
Buzdar AU, Suman VJ, Meric-Bernstam F, et al. Fluorouracil, epirubicin, and cyclophosphamide (FEC-75) followed by paclitaxel plus trastuzumab versus paclitaxel plus trastuzumab followed by FEC-75 plus trastuzumab as neoadjuvant treatment for patients with HER2-positive breast cancer (Z1041): a randomized controlled, phase 3 trial. Lancet Oncol. 2013;14(13):1317-1325.
Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomized multicenter, open-label, phase 2 trial. Lancet Oncol. 2012;13(1):25-32.
Baselga J, Bradbury I, Eidtmann H, et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a randomized, open-label, multi-centre, phase 3 trial. Lancet. 2012;379(9816):633-640.
Guarneri V, Frassoldati A, Bottini A, et al. Preoperative chemotherapy plus trastuzumab, lapatinib, or both in human epidermal growth factor receptor 2-positive operable breast cancer: results of the randomized phase II CHER-LOB study. J Clin Oncol. 2012;30(16): 1989-1995.
Rimawi MF, Mayer IA, Forero A, et al. Multicenter phase II study of neoadjuvant lapatinib and trastuzumab with hormonal therapy and without chemotherapy in patients with human epidermal growth factor receptor 2-overexpressing breast cancer: TBCRC 006. J Clin Oncol. 2013;31(14):1726-1731.
Schneeweiss A, Chia S, Hickish T, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol. 2013;24(9): 2278-2284.
Mamtani A, Barrio AV, King TA, et al. How often does neoadjuvant chemotherapy avoid axillary dissection in patients with histologically confirmed nodal metastases? Results of a prospective study. Ann Surg Oncol. 2016;23(11):3467-3474.