- The history of goitrous growth and associated symptoms is critical for determining surgical candidacy:
- This history should be obtained not only from the patient but also from his or her family
- Regional symptoms should be addressed relating to:
- Respiration
- Phonation
- Swallowing
- Presence of globus (lump sensation)
- As Pemberton emphasized in 1921:
- Symptoms associated with goiter may be positionally induced
- Positions that may provoke goiter regional symptomatology include being:
- Supine
- Arms raised (as when reaching for an upper cabinet),
- Extreme neck extension
- Extreme neck flexion (as with reading a book in bed)
- Turning the head to the extreme left or right
- Patients thus need to be questioned about positional provocation of regional symptoms
- In addition, the family needs to be questioned about nocturnal symptoms:
- As symptoms may manifest initially in the setting of recumbency and upper airway relaxation during sleep
- Symptoms may also be associated with exercise and increased oxygen demands
- A history of preceding upper respiratory tract infection may produce dyspnea in a patient with long-standing tracheal obstruction secondary to goiter:
- Through new laryngotracheal mucosal edema
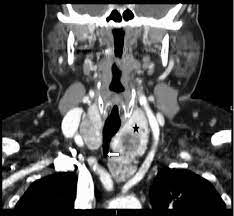
- Patients with cervical or substernal goiter may present with:
- Cough
- Dyspnea
- Foreign-body sensation
- Neck tightness
- Change in collar size
- Wheezing:
- Some patients may come to the head and neck surgeon with a misdiagnosis of asthma or chronic obstructive pulmonary disease (COPD)
- Patients with large cervical and substernal goiter:
- Approximately 25% of patients were asymptomatic
- Symptoms of hypothyroidism and hyperthyroidism should be reviewed:
- Hyperthyroidism may slowly evolve in patients with multinodular goiter or may develop acutely in response to significant iodine load such as with CT scan contrast (Jod-Basedow phenomenon) or with the introduction of iodized salt in endemic goiter regions
- A history of migration from an area of endemic goiter should be obtained, as well as a history of exposure to known goitrogens, notably iodine and lithium
- A family history of thyroid disease should be obtained

#Arrangoiz #ThyroidSurgeon #ThyroidExpert #HeadandNeckSurgeon #CancerSurgeon #MultinodularGoiter #Goiter #SubsternalGoiter #CervicalGoiter #CASO #CenterforAdvancedSurgicalOncolgy