My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
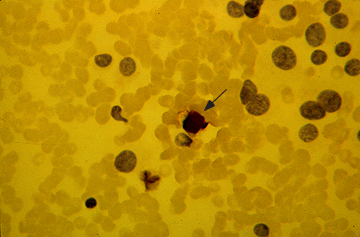
Fine-needle aspirate with immunostaining for calcitonin in medullary cancer of the thyroid. The nuclei of the tumor cells are placed eccentrically and are larger and more pleomorphic than those of normal follicular cells. Immunocytologic staining for calcitonin is positive (brown staining, which is best seen at the arrow). The background contains many red cells that nonspecifically take up the stain.
Is unique in many ways among inherited cancer syndromes:
MTC is founded on the following findings:
The hereditary variant:
Affecting as many as 25% of MTC patients:
Is more frequent than many other common hereditary tumors.
Unlike many other hereditary tumors:
Hereditary MTC features a strong genotype-phenotype correlation:
That is utilized worldwide for risk assessment
This genotype-dependent, age-related tumor progression:
Not only underlies the development of:
Hereditary MTC
But also the formation of:
MEN 2–associated pheochromocytoma and hyperparathyroidism (HPT).
Disease progression from C-cell hyperplasia to MTC:
Requiring the acquisition of somatic mutations for malignant progression:
Is a stochastic sequence of events not fully under the control of a gene carrier’s genetic makeup.
Serum calcitonin:
A sensitive diagnostic marker of MTC, better reflects a gene carrier’s stage of C-cell disease than his or her underlying germline mutation in the RET (REarranged during Transfection) proto-oncogene:
We may now tailor the timing and extent of surgical intervention in the neck to the gene carrier’s stage of disease through consideration of serum calcitonin levels.
Lymph node metastases are indicative of progressive disease:
Portending a worse prognosis for sporadic and hereditary MTC alike.
Although multifocal tumor growth:
More common in hereditary than sporadic MTC:
65% versus 8%:
No difference in biochemical cure and survival between hereditary and sporadic disease has been found after adjusting for extent of disease.
MEN 2B is a special and virulent variant of MEN type 2:
Characterized by the presence of MTC in early infancy.
More than 90% of MEN 2B RET gene carriers:
Harbor de novo germline mutations.
Such de novo germline mutations are rare in other MTC syndromic settings such as familial MTC (FMTC) and MEN 2A.
DNA-based screening of families for the MEN 2B trait for early detection of hereditary MTC hence is rarely an option.
Intriguingly, there are some early clues in MEN 2B infants:
Notably tearless crying and pseudo-Hirschsprung’s disease:
These clinical signs may help identify gene carriers before they develop the more characteristic MEN 2B stigmata:
Prompting rapid DNA-based screening and immediate surgical intervention.
What is Head and Neck Surgery?:
It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
The head and neck surgeon’s work area:
Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:
This is the neurosurgeon field.
Among the diagnostic procedures performed by the head and neck surgeon, are the following:
Nasopharyngolaryngoscopy:
Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions.
The surgeries most commonly performed by the head and neck surgeon are:
Total or near total thyroidectomies
Hemithryoidectomies (lobectomies)
Comprehensive neck dissections
Selective neck dissections
Maxillectomies:
Total maxillectomy
Subtotal maxillectomy
Infrastructure maxillectomy
Suprastructure maxillectomy
Medial maxillectomy
Mandibulectomy:
Segmental
Marginal
Tracheostomy
Salivary gland surgeries:
Parotid gland operations:
Limited superficial parotidectomy with identification and preservation of the facial nerve
Superficial parotidectomy with identification and preservation of the facial nerve
Near total parotidectomy with identification and preservation of the facial nerve
Total parotidectomy
Submandibular gland resection
Sublingual gland resection
Resection of tumors of the oral cavity:
Glossectomy
Resection of the floor of the mouth tumors
Resection of tumors of the pharynx
Resection of tumors of the larynx
Split-thickness skin grafts
Full-thickness skin grafts
Sentinel lymph node mapping and sentinel lymph node biopsy
Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
The formation of the head and neck surgeon includes mastering the following subjects:
Surgical Anatomy
History and Basic Principles of Head and Neck Surgery
Epidemiology, Etiology, and Pathology of Head and Neck Diseases
Diagnostic Radiology of the Head and Neck Region
Tumors of the Scalp, Skin and Melanoma
Eyelids and Orbit
Nasal Cavity and Paranasal Sinuses
Skull Base and Temporal Bone
Lips and Oral Cavity
Pharynx and Esophagus
Larynx and Trachea
Cervical Lymph Nodes
Thyroid and Parathyroid Glands
Salivary Glands
Neurogenic Tumors and Paragangliomas
Soft Tissue Tumors
Bone Tumors and Odontogenic Lesions
Reconstructive Surgery
Oncologic Dentistry and Maxillofacial Prosthetics
Principles of Radiation Oncology
Principles of Chemotherapy
Molecular Oncology, Genomics and Immunology
Nutrition
Biostatistic
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
Rodrigo Arrangoiz MS, MD, FACS:
Is a member of the American Head and Neck Society
He is a member of the American Thyroid Association:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
The pathological tumor, node, metastasis (pTNM) criteria for clinical / pathologic tumor staging (eighth edition) adopted by the Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC) are based upon:
Tumor size
The presence or absence of extra-thyroidal invasion
Local and regional nodal metastases
Distant metastases
Stage I :
Medullary thyroid cancers (MTCs) that are equal or less than 2 cm in diameter without evidence of disease outside of the thyroid gland
Stage II:
Tumors greater than 2 cm confined to the thyroid or tumors of any size without lymph node metastasis that demonstrate gross extrathyroidal extension invading only the strap muscles (sternohyoid, sternothyroid, thyrohyoid, or omohyoid muscles)
Stage III:
Tumors of any size demonstrating metastatic lymph node involvement in the central neck (levels VI or VII; pretracheal, paratracheal, or prelaryngeal/Delphian, or upper mediastinal lymph nodes) with or without gross invasion into the strap muscles (sternohyoid, sternothyroid, thyrohyoid, or omohyoid muscles)
Stage IV :
Any distant metastases, or lymph node involvement outside of the central neck (level VI/VII), or gross invasion into other structures of the neck (beyond just strap muscle involvement)
One study evaluated the prognostic significance of a previous TNM staging scheme in patients with MTC:
Most of whom were treated by total thyroidectomy and then followed for a median of four years:
Although the follow-up was short:
Mortality due to MTC was:
0% stage I
13% in stage II
56% in stage III
100% in stage IV
A subsequent analysis of MTC patients using the National Cancer Database and the SEER (Surveillance, Epidemiology, and End Results) data set demonstrated that the seventh and eighth editions of the AJCC staging system:
Were associated with five-year overall survival rates of:
95% in stage I
91% in stage II
89% in stage III
68% in stage IV
Furthermore:
Disease-specific survival rates were:
100% in stage I
99% in stage II
97% in stage III
82% in stage IV
Dynamic risk stratification:
Using the same concepts that were initially developed for differentiated thyroid cancer:
Dynamic risk stratification for MTC allows clinicians to modify initial AJCC staging risk estimates over time based on:
The biological behavior the tumor and the response to therapy in individual patients
For application in MTC, the definitions of the response to therapy categories needed to be modified to utilize calcitonin and carcinoembryonic antigen (CEA) as tumor markers (rather than thyroglobulin):
At each follow-up visit, patients are classified as having one of the following clinical outcomes:
Excellent response:
An undetectable calcitonin and normal-range CEA in the absence of structurally identifiable disease
Biochemical incomplete response:
A detectable calcitonin or elevated CEA in the absence of structurally identifiable disease
Structural incomplete response:
The presence of recurrent or persistentstructurally identifiable disease
In two retrospective studies examining MTC patients with a median of 5 to 7 years of follow-up:
An excellent response to therapy was associated with:
Structural disease recurrence rate of 1% to 4%
Biochemical recurrence rate of 11% to 15%
Disease-specific mortality of less than 3%
Patients with a biochemical incomplete response demonstrated a:
Structural disease recurrence rate of 32% to 37%
Biochemical recurrence rate of 51% to 53%
Disease-specific mortality of 11%
The poorest outcomes were seen in those patients with a structural incomplete response to initial therapy with:
Disease-specific mortality rates of 38% to 56%
The calcitonin and CEA doubling times:
Can also provide meaningful insights into:
Prognosis
Expected course of disease progression that can further refine these response to therapy assessments
What is Head and Neck Surgery?:
It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
The head and neck surgeon’s work area:
Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:
This is the neurosurgeon field.
Among the diagnostic procedures performed by the head and neck surgeon, are the following:
Nasopharyngolaryngoscopy:
Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions.
The surgeries most commonly performed by the head and neck surgeon are:
Total or near total thyroidectomies
Hemithryoidectomies (lobectomies)
Comprehensive neck dissections
Selective neck dissections
Maxillectomies:
Total maxillectomy
Subtotal maxillectomy
Infrastructure maxillectomy
Suprastructure maxillectomy
Medial maxillectomy
Mandibulectomy:
Segmental
Marginal
Tracheostomy
Salivary gland surgeries:
Parotid gland operations:
Limited superficial parotidectomy with identification and preservation of the facial nerve
Superficial parotidectomy with identification and preservation of the facial nerve
Near total parotidectomy with identification and preservation of the facial nerve
Total parotidectomy
Submandibular gland resection
Sublingual gland resection
Resection of tumors of the oral cavity:
Glossectomy
Resection of the floor of the mouth tumors
Resection of tumors of the pharynx
Resection of tumors of the larynx
Split-thickness skin grafts
Full-thickness skin grafts
Sentinel lymph node mapping and sentinel lymph node biopsy
Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
The formation of the head and neck surgeon includes mastering the following subjects:
Surgical Anatomy
History and Basic Principles of Head and Neck Surgery
Epidemiology, Etiology, and Pathology of Head and Neck Diseases
Diagnostic Radiology of the Head and Neck Region
Tumors of the Scalp, Skin and Melanoma
Eyelids and Orbit
Nasal Cavity and Paranasal Sinuses
Skull Base and Temporal Bone
Lips and Oral Cavity
Pharynx and Esophagus
Larynx and Trachea
Cervical Lymph Nodes
Thyroid and Parathyroid Glands
Salivary Glands
Neurogenic Tumors and Paragangliomas
Soft Tissue Tumors
Bone Tumors and Odontogenic Lesions
Reconstructive Surgery
Oncologic Dentistry and Maxillofacial Prosthetics
Principles of Radiation Oncology
Principles of Chemotherapy
Molecular Oncology, Genomics and Immunology
Nutrition
Biostatistic
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
Rodrigo Arrangoiz MS, MD, FACS:
Is a member of the American Head and Neck Society
He is a member of the American Thyroid Association:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
Halsted mastectomy or extended mastectomy with IM node dissection:
After 30 years of follow-up, there was no difference in overall survival or disease-specific survival:
For the patients eligible with T1, T2, T3, N0, and N1 disease who underwent IM node dissection vs. no IM dissection
A 2019 retrospective review of 95 breast cancer patients with clinically detected IM nodes (IMNs) at diagnosis:
Were treated with surgery and radiation:
With median follow-up of 43 months
77 received neoadjuvant chemotherapy:
With IMN normalization in 67.5%, and partial IMN response in 24.6%
The 5-year IMN failure-free survival, disease-free survival, and overall survival were:
96%, 70%, and 84%, respectively
IMN failure-free survival was significantly affected by:
Resection margin status
Size of IMN
Receipt of IMN boost radiation
A recently published meta-analysis in the Annals of Surgery found that axillary staging following neoadjuvant chemotherapy:
Is best performed with a combination approach of:
Sentinel lymph node biopsy with excision of the pre-chemotherapy-marked positive node:
With a false negative rate of 2% to 4%:
The identification rate was 100%
ACOSOG Z1071 reported an overall false negative rate of 12.6%:
When sentinel node biopsy was performed after neoadjuvant chemotherapy with documented node-positive disease prior to treatment
The false-negative rate decreased to 6.8%:
When both sentinel node(s) and the clipped node were retrieved at the time of surgery
References
Veronesi U, Marubini E, Mariani L, Valagussa P, Zucali R. The dissection of internal mammary nodes does not improve the survival of breast cancer patients. 30-year results of a randomised trial. Eur JCancer. 1999;35(9):1320-1325.
Kim J, Chang JS, Choi SH, et.al. Radiotherapy for initial clinically positive internal mammary nodes in breast cancer. Radiat Oncol J. 2019;37(2):91-100.
Simons JM, van Nijnatten TJA, van der Pol CC, Luiten EJT, Koppert LB, Smidt ML. Diagnostic accuracy of different surgical procedures for axillary staging after neoadjuvant systemic therapy in node-positive breast cancer: a systematic review and meta-analysis. Ann Surg. 2019;269(3):432-442.
Boughey JC, Ballman KV, Le-Petross HT, et al. Identification and resection of clipped node decreases the false-negative rate of sentinel lymph node surgery in patients presenting with nodepositive breast cancer (T0-T4, N1-N2) who receive neoadjuvant chemotherapy: results from ACOSOG Z1071 (Alliance). Ann Surg. 2016;263(5):802-807.
Is a distinct histopathologic subtype of breast cancer:
Representing 1% to 2% of breast cancers diagnosed
It is a distinct entity:
From low-grade ductal carcinoma
The literature continues to suggest that is has an excellent prognosis:
With a very low likelihood of distant metastasis and excellent disease-free survival.
In select patients:
Adjuvant therapies may be omitted:
However, there is a still a risk of axillary nodal metastasis:
Sentinel lymph node biopsy is still recommended due to a 10% to 20% risk of lymphatic spread
Despite this finding, there is likely to be only one node involved:
This histopathologic subtype still conveys an excellent prognosis
Tubular carcinoma is more likely to be identified on:
Screening mammography and is more common in Caucasians than blacks
Emerging data suggest that adjuvant systemic therapy can likely be safely omitted, although it should still be discussed with the multidisciplinary team
References
Rakha EA, Lee AH, Evans AJ, et al: Tubular carcinoma of the breast: further evidence to support its excellent prognosis. J Clin Oncol. 2010;28(1):99-104.
Fedko MG, Scow JS, Shah SS, et al. Pure tubular carcinoma and axillary nodal metastases. Ann SurgOncol. 2010;17(Suppl 3):338-342.
Anderson WF, Chu KC, Chang S, Sherman ME. Comparison of age-specific incidence rate patterns for different histopathologic types of breast carcinoma. Cancer Epidemiol Biomarkers Prev. 2004;13(7): 1128-1135.
Which may allow some patients to safely avoid chemotherapy
However:
The presence of ER receptors on immunohistochemistry:
Does not necessarily mean that the tumor’s growth:
Is being driven by ER-related pathways
Additionally, other molecular features may influence the tumor cells’ sensitivity to hormonal therapy
The development of predictive molecular assays has been a major advancement in the field:
The assay measures mRNA expression of 21 genes:
Using reverse transcriptase-polymerase chain reaction techniques
It can be performed on formalin-fixed paraffin-embedded tumor specimens:
Obtained by core biopsy or surgery
It has been validated in ER+, node-negative women:
Who have not received any prior therapy
This assay is more reliable in predicting cancer recurrence than such clinical parameters as:
Size
Hormone receptor status
Nuclear grade
Ki-67
The assay measures:
Downstream ER-regulated genes:
To assess the functionality of the ER receptor
Patients with low scores (<18) are considered at low risk for disease recurrence:
May not receive any benefit from adjuvant chemotherapy:
These patients are now treated with hormonal therapy alone without cytotoxic chemotherapy
In fact, the recently published subset analysis of the prospective validation of the 21-gene expression assay in breast cancer:
Confirmed that 98.7% of women:
With 21-gene signature scores of less than 10:
Managed with endocrine therapy alone had no evidence of local, regional, or distant recurrence at 5 years
Patients with a high score (>31):
Have been shown to gain a large benefit from the addition of chemotherapy
While the assay is not performed on HER2-overexpressing tumors:
It does measure HER2 and other proliferative genes
It is currently only validated for:
Node-negative patients:
Although the RxPONDER (SWOG 1007) trial:
Is currently evaluating women with:
1 to 3 positive lymph nodes and an 21-gene signature score of less than 25
These patients were randomized to receive chemotherapy and endocrine therapy to endocrine therapy alone:
We are awaiting the results of this trial
References
Paik S. Development and clinical utility of a 21-gene recurrence score prognostic assay in patients with early breast cancer treated with tamoxifen. Oncologist. 2007;12(6):631-635.
Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817-2826.
Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol. 2006;24(23):3726-3734.
Sparano JA, Gray RJ, Makower DF, et al. Prospective validation of a 21-gene expression assay in breast cancer. New Engl J Med. 2015;373(21):2005-2014.
2019 International Clinical Practice Guidelines for the Treatment and Prophylaxis Of Venous Thromboembolism In Patients With Cancer
Initial treatment of established VTE – International Advisory Panel ranking (8.18 out of 9)
Low-molecular-weight heparin (LMWH):
Is recommended for the initial treatment of established VTE in patients with cancer:
When creatinine clearance is ≥ 30 mL per min (grade 1B)
LMWH:
Is easier to use than unfractionated heparin
A regimen of LMWH:
Taken once per day:
Is recommended, unless a twice-per-day regimen is required:
Because of patient characteristics (eg, fragile patients who are at risk of hemorrhage)
For patients who do not have a high risk of gastrointestinal or genitourinary bleeding:
A regimen of rivaroxaban (in the first 10 days) or edoxaban (started after at least 5 days of parenteral anticoagulation):
Can also be used for the initial treatment of established VTE:
In patients with cancer when creatinine clearance is ≥ 30 mL/min (grade 1B)
Unfractionated heparin:
Can also be used for the initial treatment of established VTE in patients with cancer:
When LMWH or direct oral anticoagulants are contraindicated, or not available (grade 2C)
Fondaparinux can also be used for the initial treatment of established VTE:
For patients with cancer (grade 2D)
Fondaparinux is easier to use than unfractionated heparin
Thrombolysis in patients with cancer with established VTE can only be considered on a case-by-case basis:
With specific attention paid to contraindications, especially bleeding risk eg, brain metastasis (guidance, based on evidence of very low quality and the high bleeding risk of thrombolytic therapy)
An expert opinion is recommended before using thrombolytics, and the procedure should be done in centers with health-care practitioners who have appropriate expertise
In the initial treatment of VTE:
Inferior vena cava filters may be considered when:
Anticoagulant treatment is contraindicated or
In the case of pulmonary embolism
When recurrence occurs under optimal anticoagulation
Periodic reassessment of contraindications for anticoagulation is recommended, and anticoagulation should be resumed when safe (guidance, based on evidence of very low quality and an unknown balance between desirable and undesirable effects)
Early maintenance (up to 6 months) and long term (beyond 6 months) – International Advisory Panel ranking (8.09 out of 9):
LMWHs are preferred over vitamin K antagonists:
For the treatment of VTE in patients with cancer:
When creatinine clearance is ≥ 30 mL/min (grade 1A)
Daily subcutaneous injection can represent a burden for patients
Direct oral anticoagulants:
Are recommended for patients with cancer:
When creatinine clearance is ≥ 30 mL/min in the absence of strong drug-to-drug interactions or gastrointestinal absorption impairment (grade 1A)
Use caution in patients with:
Gastrointestinal tract malignancies, especially upper gastrointestinal tract malignancies:
As the available data show increased risk of gastrointestinal tract bleeding with:
Edoxaban and rivaroxaban
Data for other direct oral anticoagulants are needed as it is not clear whether other direct oral anticoagulants will have the same risk profile
LMWH or direct oral anticoagulants should be used for:
A minimum of 6 months to treat established VTE in patients with cancer (grade 1A)
After 6 months:
Termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists):
Should be based on individual evaluation of the benefit–risk ratio, tolerability, drug availability, patient preference, and cancer activity (guidance in the absence of data)
Treatment of VTE recurrence in patients with cancer under anticoagulation – International Advisory Panel ranking (8.0 out of 9):
In the event of VTE recurrence, three options can be considered:
Increase LMWH by 20% to 25%
Switch to direct oral anticoagulants:
For direct oral anticoagulants:
Switch to LMWH
For vitamin K antagonists:
Switch to LMWH or direct oral anticoagulants (guidance based on evidence of very low quality and an unknown balance between desirable and undesirable effects)
Effect of therapy should be monitored:
By improvement of symptoms
Treatment of established catheter-related thrombosis – International Advisory Panel ranking (8.19 out of 9):
For the treatment of symptomatic catheter-related thrombosis in patients with cancer:
Anticoagulant treatment is recommended for a minimum of 3 months and as long as the central venous catheter is in place
In this setting:
LMWHs are suggested and direct comparisons between LMWHs, direct oral anticoagulants, and vitamin K antagonists have not been made (guidance)
In patients with cancer with catheter-related thrombosis:
The central venous catheter can be kept in place:
If it is functional, well positioned, and not infected:
With a good resolution of symptoms under close surveillance while anticoagulation therapy is administered
No standard approach in terms of duration of anticoagulation is established (guidance)
Overweight or obesity (particularly in postmenopausal women)
White race or Ashkenazi Jewish descent
Medical history:
BRCA1 or BRCA2 mutation
First-degree relative with breast or ovarian cancer
History of atypical hyperplasia or lobular carcinoma in situ
One prior breast biopsy (regardless of results)
Personal history of breast or ovarian cancer
Medications and diet:
Alcohol consumption (more than one drink per day)
Current or prior use of hormone therapy or oral contraceptives
Reproductive history: o Menarche before 12 years of age o Menopause after 55 years of age o Nulliparity or age older than 35 years at first delivery • Other: o High breast density on mammography o Prior thoracic radiation exposure
Is the standard of care in patients with early stage, clinically node negative breast cancer
Compared to axillary lymph node dissection (ALND),:
SLNB has lower morbidity, including a:
Lower risk of musculoskeletal limitations and lymphedema
In general, SLNB can be performed with the use of:
Blue dye
Technetium-99 (99mTc), or
Dual agents
The role of SLNB in pregnancy is not clearly defined:
Recently updated American Society of Clinical Oncology (ASCO) Guidelines:
Upholds its prior recommendation that SLNB should not be performed in pregnancy:
The strength of the recommendation, however;
Is described by the ASCO expert panel to be “weak,” as it is based on ”informal consensus” rather than quality evidence.
Several retrospective studies have described the safety of SLNB during pregnancy
The majority of patients in these studies underwent SLNB with 99mTc alone:
However, methylene blue dye was used in some patients
One recent retrospective review reported on 145 women with clinical node-negative disease who underwent SLNB during pregnancy:
The mapping agents utilized were:
99mTc alone (66%), methylene blue dye alone (9.7%), dual agents (10.3%), and the remainder was unknown
Sentinel lymph nodes were identified in 99.3% of patients, with excellent gestational outcomes
No neonatal adverse events related to the SLNB procedure were reported
Models of fetal radiation exposure have demonstrated that the use of 99mTc for SLNB:
Leads to a negligible dose to the fetus of 0.014 mGy or less:
Whereas risk of fetal malformation is associated with levels > 100 mGy
Lower doses of exposure can be achieved using a 1-day protocol rather than a 2-day protocol
The use of lymphazurin dye is not recommended:
Due to the 1% to 2% risk of anaphylaxis
Historically, the use of direct intra-amniotic injection of methylene blue dye for identification of ruptured membranes led to significant neonatal complications:
Recent pharmacokinetic data indicate that the absorption of methylene blue dye used during SLNB is minimal
Although the use of methylene blue dye for SLNB has been described, the data are limited in comparison to that of 99mTc
Thus, with respect to axillary staging, the risks and benefits of ALND vs. SLNB must be discussed with the patient prior to surgery
References
Giuliano AE, Kirgan DM, Guenther JM, Morton DL. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg. 1994;220(3):391-398.
Lyman GH, Somerfield MR, Bosserman LD, Perkins CL, Weaver DL, Giuliano AE. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology Clinical Practice Guideline Update.J Clin Oncol. 2017;35(5):561-564.
Han SN, Amant F, Cardonick EH, et al. Axillary staging for breast cancer during pregnancy: feasibility and safety of sentinel lymph node biopsy. Breast Cancer Res Treat. 2018;168(2):551-557.
Gropper AB, Calvillo KZ, Dominici L, et al. Sentinel lymph node biopsy in pregnant women with breast cancer. Ann Surg Oncol. 2014;21(8):2506-2511.
Gentilini O, Cremonesi M, Toesca A et al. Sentinel lymph node biopsy in pregnant patients with breast cancer. Eur J Nucl Med Mol Imaging. 2010;37(1):78-83.
Pandit-Taskar N, Dauer LT, Montgomery L et al. Organ and fetal absorbed dose estimates from 99mTc-sulfur colloid lymphoscintigraphy and sentinel node localization in breast cancer patients. J Nucl Med. 2006;47(7):1202-1208.
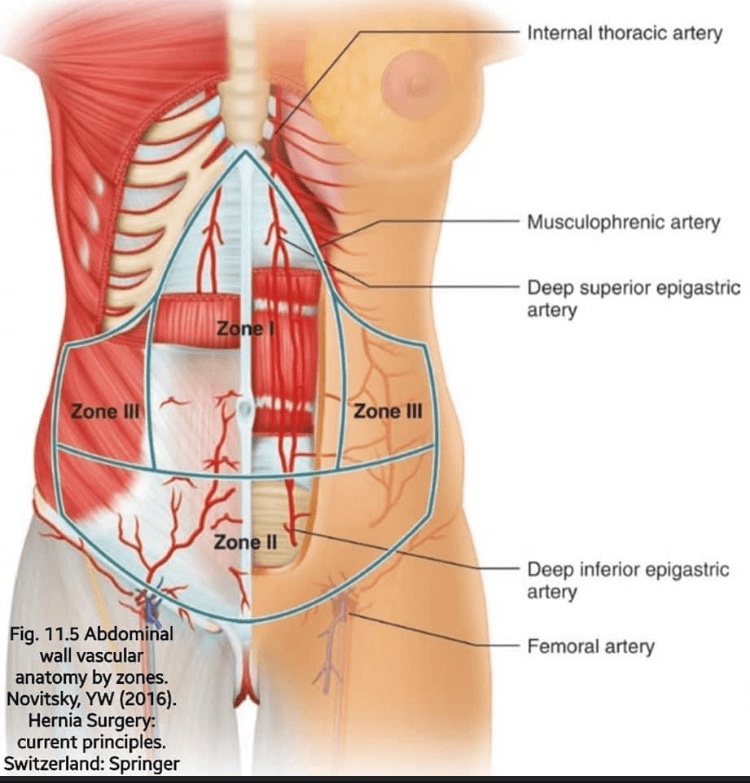
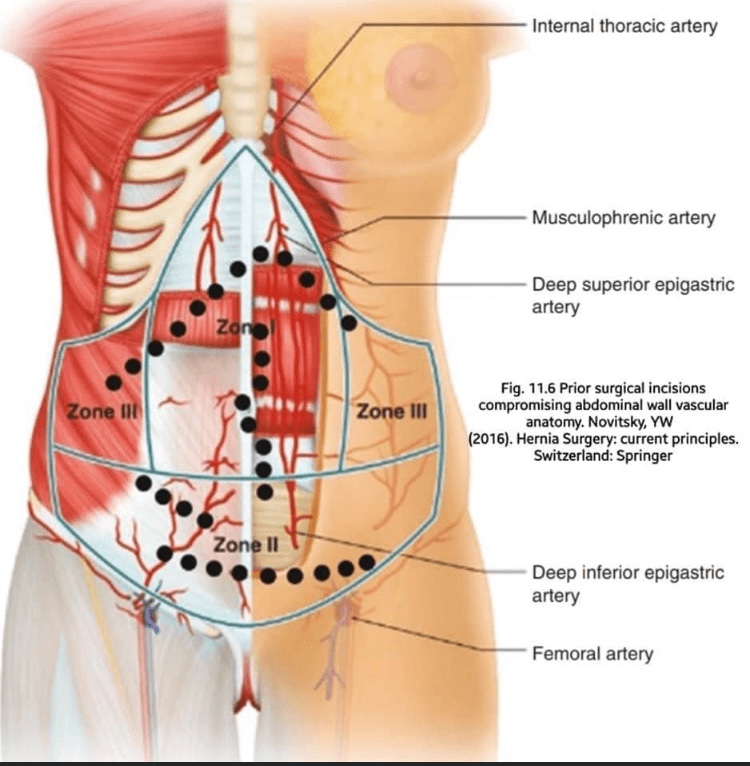
👉The vascular anatomy of the abdominal wall is divided into three zones based on the origin of the blood suppl
𝗭𝗼𝗻𝗲 1 is the central upper abdomen
Superiorly it receives blood supply from the descending superior epigastric artery, a branch of the internal mammary artery
Inferiorly it is supplied by the ascending inferior epigastric artery, a branch of the external iliac artery
As the superior and inferior epigastric arteries run posterior to the rectus abdominis muscle, they supply musculocutaneous perforating vessels (the so-called periumbilical perforator vessels) to the overlying tissues
The superior and inferior epigastric arteries converge in the supraumbilical region
𝗭𝗼𝗻𝗲 2 encompasses the suprapubic area below the arcuate line
The area is supplied medially by the superficial and deep branches of the inferior epigastric artery
Laterally, blood supply comes from the superficial circumflex iliac artery as a branch of the external iliac
𝗭𝗼𝗻𝗲 3 is the area superior the arcuate line and lateral to the linea semilunaris
It is perfused superiorly by the musculophrenic artery as a lateral branch of the internal mammary artery
Inferiority by the deep circumflex iliac artery
When evaluating a patient who requires ventral herniorrhaphy, the blood supply to each zone should be considered as it may be comprised by prior surgical incisions (such as a panniculectomy or paramedian incision) or prior surgical procedure (such as epigastric ligation or abdominal aortic aneurysm repair)
𝗖𝗹𝗶𝗻𝗶𝗰𝗮𝗹 𝗶𝗺𝗼𝗽𝗿𝘁𝗮𝗻𝗰𝗲:
𝗭𝗼𝗻𝗲𝘀 1 and 3:
Kocher and Chevron incisions generally divide the right and potentially left superior epigastric artery and must be considered in patients who have had open cholecystectomy, liver resection, or liver transplantation
In addition, patients who have had the internal mammary artery harvested for coronary bypass grafting, mediastinal dissection, or mediastinal chest tubes can disrupt the internal mammary, superior epigastric artery, or musculophrenic blood supply to Zones 1 and 3
𝗭𝗼𝗻𝗲 2:
Blood supply is at risk with prior paramedian, Mcburney, Rockey-Davis, and Pfannenstiel incisions
Additionally the periumbilical region is a watershed area with tenuous blood supply in patients with large umbilical hernias and previous midline scars
Failure to excise compromised skin or scar can lead to wound breakdown and surgical site infections
𝗥𝗲𝗳:SAGES manual of hernia surgery, 2019. By: Hesham Wageh