Dou Y, Chen Y, Hu D, Su X 2021 The recovery of thyroid function in low-risk papillary thyroid cancer after lobectomy: A 3-year follow-up study. Front Endocrinol (Lausanne) 11:619841. PMID: 33633689.
Background
The incidence of low-risk papillary thyroid cancer has been increasing, due in part to the early diagnosis of thyroid nodules and thyroid cancer. For these low-risk tumors, the outcomes for lobectomy are similar to those for total thyroidectomy; lobectomy also has the advantage of a lower risk of complications such as vocal-fold palsy and hypoparathyroidism and likely a lower need for thyroid hormone replacement.
However, many studies have begun to show that a significant proportion of patients who undergo lobectomy will need hormone supplementation owing to high levels of serum thyrotropin (TSH) (>2 mIU/L), in line with recommendations for postthyroidectomy thyroid cancer treatment. This study evaluated the factors related to the maintenance of thyroid function after lobectomy for patients with low-risk papillary thyroid cancer and the proportion of these patients who recovered thyroid function in the first year after surgery.
Methods
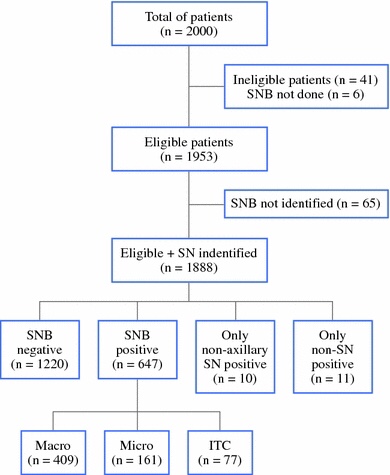
This is a retrospective study of 190 patients who underwent lobectomy for low-risk papillary thyroid cancer. The follow-up period ranged from 20 to 36 months. The clinicopathological variables analyzed were age, sex, tumor size, tumor location, body-mass index, thyroid lobe resected (left or right), Hashimoto’s thyroiditis, preoperative TSH, and postoperative TSH.
None of the patients received any thyroid hormone therapy in the immediate postoperative period; thyroid function was monitored. The authors evaluated thyroid function and related symptoms every 3 months in the first postoperative year and every 6 months in the second and third years. Patients with TSH levels >10 mlU/L or TSH levels > 5.9 mIU/L with marked signs of hypothyroidism were started on levothyroxine. Patients with subclinical hypothyroidism without symptoms were observed without hormone replacement until the subsequent follow-up visit. None of the patients showed any neck metastasis or disease recurrence in the remaining thyroid lobe during the follow-up period.
Results
Of all 190 subjects, 113 (47%) continued to have normal thyroid function, while 77 (53%) developed temporary or permanent hypothyroidism. The univariate analysis showed no difference in in the two groups regarding age, sex, tumor size or location, body-mass index, and serum thyroperoxidase (TPO) autoantibody positivity. Interestingly, the laterality of the resected lobe was significant in the development of postoperative hypothyroidism (70.1% of patients who underwent right lobectomy vs. 49.6% of patients who underwent left lobectomy).
High preoperative serum TSH levels (>2.62 mIU/L) was the most important independent risk factor for the development of postoperative hypothyroidism, followed by Hashimoto’s thyroiditis and right lobectomy.
High levels of serum thyroglobulin autoantibody were also associated with postoperative hypothyroidism, but not as an independent factor. Twenty-eight (36.4%) of the patients in the hypothyroidism group recovered normal thyroid function, and 49 (63.6%) remained hypothyroid. Only a high TSH preoperative level was associated with permanent hypothyroidism in this latter group. In the follow-up period, both the euthyroid and recovery groups maintained a relatively stable TSH level, in a range similar to that of the preoperative TSH level. An acute fluctuation in the TSH level was seen owing to initiation of or changes in levothyroxine therapy. The time to recover thyroid function varied from 3 to 9 months, and all patients who recovered normal thyroid function during this immediate period remained euthyroid during long-term follow-up.
Conclusions
In this cohort of patients who underwent thyroid lobectomy for low-risk thyroid cancer, higher levels of preoperative serum TSH (>2.62 mIU/L), Hashimoto’s thyroiditis, and right lobectomy were independent factors associated with postoperative hypothyroidism.
This study addresses a topic that is of great interest when caring for patients with low-risk papillary carcinoma who undergo partial thyroidectomies: anticipating the need for thyroid hormone replacement in the postoperative period.
The acceptance of thyroid lobectomy as an optimal surgical option for appropriate patients is expanding. This approach appears to have oncologic outcomes similar to those for total thyroidectomy, yet with a low level of complications such as recurrent laryngeal-nerve damage, hypoparathyroidism, and hypothyroidism. However, many lobectomy patients do develop transient or permanent hypothyroidism that requires hormone replacement. The factors that influence thyroid function after lobectomy remain unclear, as is the goal for serum thyroid function in this group of patients. Although the American Thyroid Association guidelines recommend the maintenance of TSH levels at <2.0 mlU/L, many studies suggest that in this group of patients, thyroid hormone replacement may not be a strong driver of preventing disease recurrence. Also, in some patients who develop hypothyroidism after lobectomy, thyroid function could still recover up to 1 year after surgery.
This study’s strength is its analysis of all the factors related to the increased incidence of postoperative hypothyroidism and those associated with the recovery of thyroid function. The study corroborates the findings by several other authors, who have reported that TSH levels slightly higher than those currently recommended did not increase the chance of recurrence of low-risk papillary cancers treated by lobectomy (1,2,7). Another important conclusion is that the most significant predictor of postoperative hypothyroidism is an elevated preoperative TSH, besides the presence of Hashimoto’s thyroiditis, which is similar to observations from our clinical practice. However, in contrast to the present study’s findings, we do not perceive a significative difference in serum thyroid function among patients who undergo a right or left lobectomy.
The overall message of the study is to show that in patients with low-risk papillary thyroid cancer who undergo lobectomy, waiting up to 1 year before starting hormone replacement, especially in patients with low preoperative TSH levels and no evidence of Hashimoto’s thyroiditis, may be reasonable. We have followed these principles in our daily practice as well, and have noted appropriate oncologic outcomes and good quality of life of our patients.
#Arrangoiz #ThyroidSurgeon