The use of catheter-based, accelerated partial-breast irradiation (APBI) offers many potential advantages over routine whole-breast radiation therapy, including decreased treatment time and decreased radiation dose delivered to uninvolved portions of the breast and adjacent organs. This has resulted in significant interest in APBI, with more than 32,000 women in the United States having had treatment with a breast brachytherapy catheter.
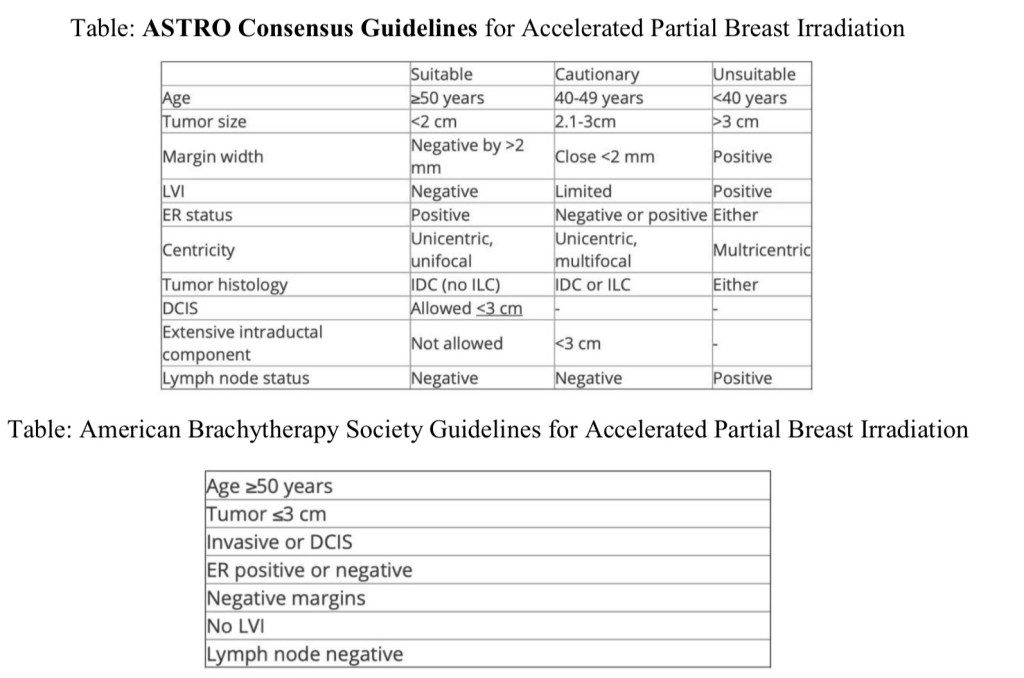
However, randomized clinical trials comparing APBI with conventional whole-breast radiation therapy have yet to be completed. In light of this, the American Society for Radiation Oncology (ASTRO) has issued a consensus statement regarding the appropriate use of APBI, categorizing potential patients for APBI into three groups: suitable, cautionary, and unsuitable. A similar, but somewhat more liberal guideline was put forth by The American Brachytherapy Society.
Accelerated partial breast irradiation includes multiple techniques such as: interstitial brachytherapy, applicator brachytherapy, external beam radiation therapy.
The Groupe Européen de Curie thérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO) trial randomized 1184 patients with low-risk invasive carcinoma or ductal carcinoma in situ (DCIS) treated with breast-conserving surgery to either whole-breast irradiation (WBI) or APBI using multi catheter brachytherapy. The cumulative incidence of local recurrence at 5 years was 1.44% with APBI and 0.92% with WBI.
The Florence trial randomized 520 patients to either WBI or APBI with intensity-modulated radiation therapy, with a mean follow-up of 5 years. The rate of local recurrence was 1.5% in both arms.
The American Society of Breast Surgeons’ Mammo Site Registry found 5-year rates of local recurrence were less than 4%.
An older randomized trial from Hungary using interstitial APBI and electrons found that the 5-year local recurrence rate of 4.7%.
It is important to recognize that these outcomes are likely due to the highly selected, low-risk patient populations included in many of the APBI trials as evidenced by the tables / guidelines: patients tend to be postmenopausal, tumors less than 3 cm, without DCIS, node negative, ER-positive.

Arthur D W, Vicini F A, Kuske RR, Wazer DE, American Brachytherapy Society. Accelerated partial breast irradiation: an updated report from the American Brachytherapy Society. Brachytherapy. 2003;2:124-130.
Hughes KS, Schnaper LA, Berry D, et al. Cancer and Leukemia Group B; Radiation Therapy Oncology Group; Eastern Cooperative Oncology Group. Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer. N Engl J Med. 2004;351:971-977.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Breast Cancer. Available at http://www.nccn.org.
Smith BD, Arthur DW, Buchholz TA, et al. Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO). J Am Coll Surg. 2009;209:269-277.
Giuliano AE, Ballman KV, McCall L, et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA. 2017; 318(10): 918-926. doi: 10.1001/jama.2017.11470.
