- The term goiter refers to:
- An abnormal growth of the thyroid gland
- Depending on the etiology goiters can be:
- Diffuse
- Nodular
- May be associated with:
- Normal thyroid hormone production
- Decreased thyroid hormone production
- Increased thyroid hormone production
- The clinical manifestations vary with:
- Thyroid function and with the size and location of the goiter
- Anatomical Relationships:
- In healthy adults without iodine deficiency:
- A normal thyroid gland is approximately:
- 4.0 cm to 4.8 cm x 1.0 cm to 1.8 cm x 0.8 cm to 1.6 cm in size
- Mean sonographic volume of:
- 7 mL to 10 mL:
- Thyroid volume measured by ultrasonography:
- Is slightly greater in men than women
- Increases with age and body weight
- Decreases with increasing iodine intake
- Thyroid volume measured by ultrasonography:
- 7 mL to 10 mL:
- A normal thyroid gland is approximately:
- In healthy adults without iodine deficiency:
- Weight of the thyroid gland:
- 10 grams to 20 grams:
- As high as 30 grams is considered normal
- 10 grams to 20 grams:
- The normal thyroid gland:
- Is immediately caudal to the larynx and encircles the anterolateral portion of the trachea
- The thyroid gland is bordered by:
- The trachea and esophagus posteriorly
- The carotid sheath laterally
- Enlarging thyroid lobes:
- Usually grow outward:
- Because of their location in the anterior neck in front of the trachea:
- Covered only by the thin strap muscles, subcutaneous tissue, and skin
- Because of their location in the anterior neck in front of the trachea:
- As a result of this outward growth:
- Even very large goiters:
- May not compress the trachea or impinge on the great vessels lateral to the lobes:
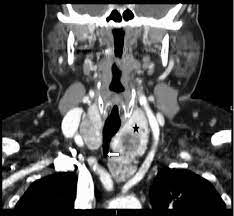
- However, in patients with substantial enlargement of one lobe or asymmetric enlargement of both lobes:
- The trachea, esophagus, or blood vessels:
- May be displaced or, less often, compressed
- The trachea, esophagus, or blood vessels:
- Bilateral lobar enlargement:
- Especially if the goiter extends posterior to the trachea:
- May cause either:
- Compression or concentric narrowing of the trachea
- Compression of the esophagus
- Compression of the jugular veins
- May cause either:
- Especially if the goiter extends posterior to the trachea:
- However, in patients with substantial enlargement of one lobe or asymmetric enlargement of both lobes:
- May not compress the trachea or impinge on the great vessels lateral to the lobes:
- Even very large goiters:
- Usually grow outward:
- The thoracic inlet:
- Is an ovoid area that measures approximately 5 cm x 10 cm:
- Boundaries:
- The sternum anteriorly
- The first thoracic vertebral body posteriorly
- The first ribs laterally
- Boundaries:
- The inlet is traversed by the:
- Trachea
- Esophagus
- Blood vessels
- Nerves
- The inferior pole of each thyroid lobe:
- Normally lies above the thoracic inlet:
- However, with some goiters, there is growth of one or both lobes through the inlet into the thoracic cavity:
- Which can result in obstruction of any of the structures in the inlet:
- Such goiters are called substernal:
- Although retrosternal is probably a more precise term
- Such goiters are called substernal:
- Which can result in obstruction of any of the structures in the inlet:
- However, with some goiters, there is growth of one or both lobes through the inlet into the thoracic cavity:
- Normally lies above the thoracic inlet:
- Is an ovoid area that measures approximately 5 cm x 10 cm:
- Most substernal goiters are in the:
- Anterolateral mediastinum:
- But approximately 10%:
- Are located primarily in the posterior mediastinum
- But approximately 10%:
- Anterolateral mediastinum:
- The prevalence of substernal goiter as a percentage of thyroidectomies:
- Ranges from 2% to 19%
#Arrangoiz #ThyroidSurgeon #HeadandNeckSurgeon #CancerSurgeon #MSMC #MountSinaiMedicalCenter #Miami #Mexico #Goiter #SubsternalGoiter
