Several trials showed that extended adjuvant endocrine therapy beyond 5 years provides additional benefit in terms of reduction of disease recurrence
According to ASCO guidelines, all patients with node-positive disease should be offered 10 years of adjuvant ET
Guidelines from the European Society for Medical Oncology (ESMO) also note that 10 years of treatment is advantageous. Moreover, women with node-negative breast cancer may be offered extended adjuvant endocrine therapy for up to 10 years, on the basis of considerations of recurrence risk using established prognostic factors
Conversely, women with low-risk, node-negative tumors should notroutinely be offered extended therapy because the absolute reduction of recurrence risk is likely to be small in this category of patients
The ESMO notes that extended therapy should not be offered to those with a very low risk of relapse
Similarly, 5 years of ovarian function suppression with either tamoxifen or an aromatase inhibitor provides an additional benefit for this patient population. However, there is no evidence that continuing ovarian function suppression alone beyond 5 years provides additional benefit
Although most breast cancers do not present with any symptom and are diagnosed through screening mammograms, breast cancer may present with different signs and symptoms, including breast lumps, nipple inversion and discharge, and peau d’orange
Signs in palpable lumps that should raise concern include focal nodularity, hardness, irregularity, and asymmetry with the other breast
Treatment strategies for early-stage hormone receptor positive / human epidermal receptor 2 negative (HR+/HER2-) breast cancer comprise definitive local therapy (primary surgical management of the breast and axilla with or without adjuvant radiation), and adjuvant endocrine therapy with or without chemotherapy
Nearly all patients with early-stage, HR+ breast cancers should be considered as candidates for adjuvant endocrine therapy
Conversely, adjuvant chemotherapy is considered only in a subgroup of patients with HR+/HER2- early breast cancer, based on the predicted risk for recurrence; the expected benefit from chemotherapy; and patient-specific factors, such as comorbidities.
In very select cases, neoadjuvant endocrine therapy or chemotherapy may be an option for patients with early-stage HR+ disease prior to surgery.
Approximately 70% to 80% of all breast cancers are hormone receptor–positive (HR+), with tumor cells expressing either the estrogen receptor (ER), progesterone receptor (PR), or both.
Testing for human epidermal growth receptor 2 (HER2) protein overexpression and / or HER2 gene amplification is undertaken at diagnosis to guide treatment decisions
More than 80% of HR+ tumors are HER2-negative (HER2-) so that HR+/HER2- breast cancer is the most common subtype of invasive breast cancer
Adjuvant therapy for breast cancer aims to treat micrometastatic disease
A cornerstone of treatment for HR+/HER2- breast cancer is adjuvant endocrine therapy (eg, aromatase inhibitors and/or tamoxifen with or without ovarian suppression).
Cyclin-dependent kinase 4 / 6 (CDK4/6) inhibitors have become integral to the treatment of HR+ / HER2- breast cancer
Approved in 2015 for use in the metastatic setting and most recently in the adjuvant setting, CDK 4 / 6 inhibitors have revolutionized treatment in both endocrine-sensitive and endocrine-resistant settings and in premenopausal and postmenopausal women
Many questions remain regarding the optimal use of these medications in clinical practice.
The three main studies that looked at the role of adjuvant CDK 4 / 6 inhibitors, including the PALLAS and PENELOPE-B trials, in which palbociclib showed no benefit in invasive disease-free survival
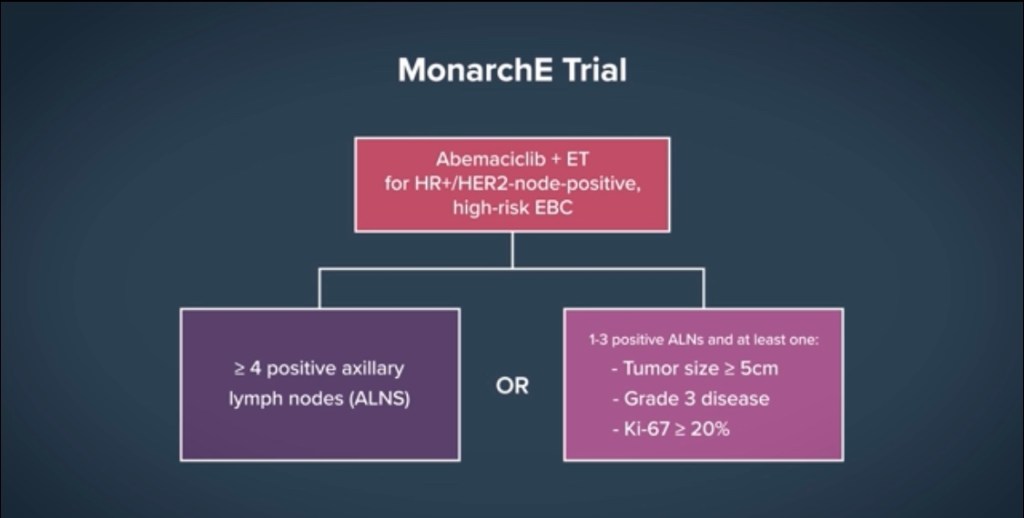
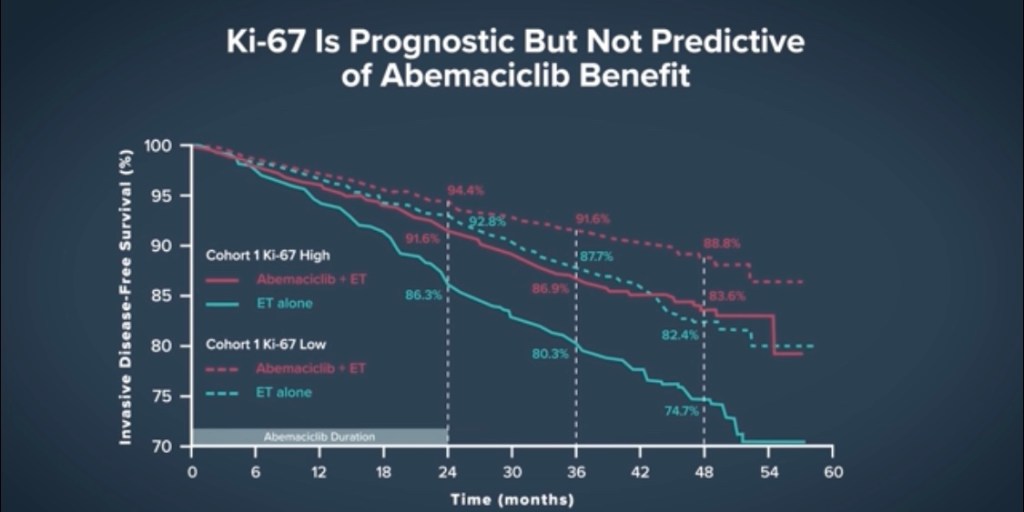
In contrast, in the monarchE trial, abemaciclib showed a robust benefit in preventing recurrence, which was sustained after longer follow-up, as reported at the San Antonio Breast Cancer Symposium 2022
The neoadjuvant or adjuvant chemotherapy options for patients with TNBC:
Are similar to the approaches used in other breast cancer phenotypes
The principles for the surgical management of and radiation therapy options for breast cancer are also applied in a similar way across breast cancer subtypes
Tumors equal or greater than 0.5 cm:
Chemotherapy:
Chemotherapy is recommended for women with:
TNBC equal or greater than 0.5 cm or with node-positive TNBC (regardless of tumor size):
These patients have a higher risk of relapse compared with other breast cancer phenotypes and are not candidates for other forms of targeted therapy (ie, HER2-directed treatment or endocrine therapy)
Neoadjuvant versus adjuvant administration:
Neoadjuvant chemotherapy (NACT) is the preferable approach in patients with:
Locally advanced breast cancer or for those who are not candidates for or unlikely to have a good cosmetic outcome with breast conservation
For patients receiving NACT:
Pathologic complete response:
Is associated with improvement in disease-free survival (DFS)
Additionally, patients with smaller (eg, T1c) TNBCs:
May be offered neoadjuvant therapy:
Particularly if they might be candidates for additional treatments in the adjuvant setting if residual disease is identified
Benefits:
Stage for stage, there is a larger absolute benefit to adjuvant chemotherapy among patients with TNBC compared with those with hormone-positive diseas:
In an analysis of three randomized trials that involved a total of 6644 women with node-positive breast cancer, compared with those with ER-positive breast cancer, patients with ER-negative breast cancer:
Had the following significant outcomes at five years following adjuvant chemotherapy:
A larger reduction in the risk of recurrence:
55% versus 26%:
This translated into a higher absolute improvement in DFS:
23% versus 7%
A larger reduction in the risk of death:
55% versus 23%:
This translated into a higher absolute improvement in overall survival (OS):
17% vs 4%
These data emphasize the importance of neoadjuvant chemotherapy for women with TNBC:
Who (unlike those with ER-positive or HER2-positive breast cancer) are not eligible for targeted therapies
Choice of regimen:
Preferred regimen:
Anthracycline-, alkylator-, and taxane-based chemotherapy regimens remain the standard regimens for TNBC:
For example, dose-dense doxorubicin and cyclophosphamide followed by paclitaxel (AC-T)
Taxanes have significant activity in the treatment of TNBC:
There are no meaningful data regarding regimens lacking alkylator-based therapy:
As an example of the benefits of a taxane:
In the GEICAM 9906 trial of adjuvant fluorouracil, epirubicin and cyclophosphamide (FEC) versus FEC followed by paclitaxel:
The addition of paclitaxel was associated with an improvement in DFS at seven years:
74% vs 56%
The ABC trials:
Tested anthracycline / taxane-based regimens versus docetaxel and cyclophosphamide (TC) given for the same duration:
Finding a benefit overall for incorporation of the anthracycline:
Particularly in TNBC in subset analysis:
However, the absolute benefit in node-negative TNBC appears modest
Non-anthracycline-based regimens:
Are an appropriate alternative for patients with lower-risk TNBC:
Node-negative
Less than 1 cm
Those with cardiac risk factors
Those who prefer to avoid the risks associated with anthracyclines
TC:
Is an alternative in low-risk disease
For example, in a randomized trial of nearly 650 patients with operable TNBC:
Those assigned to six cycles of adjuvant paclitaxel and carboplatin (administered on days 1, 8, and 15 every 28 days):
Had a longer DFS relative to those assigned to an anthracycline and taxane based regimen:
Five-year DFS 87% vs 80%:
With similar OS
Is there a role for an antimetabolite agent?
For patients with stage II or III TNBC, neoadjuvant regimens such as AC-T or TC are standard:
Followed by capecitabine for those with residual disease:
Given results of a randomized trial showing an OS benefit with the adjuvant addition of capecitabine when residual disease is present:
However, for patients with stage I disease, adjuvant rather than neoadjuvant treatment is appropriate:
Using standard regimens such as AC-T or TC
In general, for patients who have not received neoadjuvant chemotherapy:
Adding antimetabolite agents such as capecitabine or gemcitabine to adjuvant chemotherapy:
Has not improved OS outcomes in TNBC
A Chinese trial demonstrated improvement in DFS, but not OS, with capecitabine following standard adjuvant regimens:
Among 434 women with early-stage TNBC who received standard adjuvant treatment (94% of whom had not received neoadjuvant therapy):
Low-dose capecitabine maintenance therapy for one year improved five-year DFS compared with observation only:
83% versus 73%; hazard ratio [HR] 0.64, 95% CI 0.42-0.95)
The five-year OS was similar between the groups:
86% vs 81%:
With and without capecitabine, respectively; HR 0.75, 95% CI 0.47-1.19)
The trial had important limitations; notably, there was an imbalance in randomization, with a higher proportion of older women assigned to placebo, which could have favored the capecitabine group
In a separate phase III trial of 876 women with early-stage TNBC who had received standard adjuvant chemotherapy:
Subsequent treatment with capecitabine versus placebo resulted in numerically:
But not statistically, improved five-year DFS and OS (DFS, 80% versus 77%, HR 0.79, 95% CI 0.61-1.03; OS, 86.2% versus 85.9% , HR 0.92, 95% CI 0.66-1.28)
Similarly, trials looking at adjuvant gemcitabine have proven negative.
Given the sum of data, most medical oncologist opt for standard anthracycline- and/or taxane-based chemotherapy regimens as adjuvant therapy in patients with TNBC who have not received neoadjuvant treatment:
As discussed, in practice, only lower-risk patients (ie, stage I TNBC) are treated with adjuvant rather than neoadjuvant chemotherapy:
As most patients with higher-risk disease receive neoadjuvant therapy
Is there a role for platinums?
There is controversy as to whether adding platinum-based chemotherapy should be “standard” in stage II or III TNBC:
Trials have shown that adding platinum-based chemotherapy to neoadjuvant regimens can improve the rate of complete pathologic response:
However, to date, this has not improved OS in women also receiving anthracycline-, alkylator-, and taxane-based treatment
PARP inhibitors for BRCA carriers:
The poly(ADP-ribose) polymerase (PARP) inhibitor olaparib:
Has regulatory approval by the US Food and Drug Administration for the adjuvant treatment of adult patients with deleterious or suspected deleterious germline breast cancer susceptibility gene (BRCA)-mutated, HER2-negative, high-risk early breast cancer:
Who have been treated with neoadjuvant or adjuvant chemotherapy
Is there a role for immunotherapy?
Pembrolizumab has regulatory approval with chemotherapy for the neoadjuvant treatment of patients with high-risk, early-stage TNBC
Triple-negative means cancers that have less than 1 percent expression of ER and PR as determined by immunohistochemistry (IHC), and that are either 0 to 1+ by IHC, or IHC 2+ and fluorescence in situ hybridization (FISH)-negative (not amplified):
According to American Society of Clinical Oncology / College of American Pathologists (ASCO/CAP) guidelines
Receptor testing and the cut-offs used to determine ER, PR, and HER2 statuses:
Were developed to determine the odds of response to endocrine and HER2-directed therapy, respectively:
They were not developed to distinguish a distinct biologic subtype of breast cancer:
Such as the “triple-negative” phenotype
In support of this definition of ER and PR receptor-negative status:
An analysis of cooperative group studies with centrally determined ER, PR, and molecular subtype suggests that this group is molecularly heterogeneous, including both luminal and nonluminal subtypes
Staging:
The clinical staging of breast cancer is identical across breast cancer subtypes using the American Joint Committee on Cancer and the International Union for Cancer Control (AJCC-UICC) Tumor, Node, Metastasis (TNM) breast cancer staging system
Are more likely to be diagnosed clinically rather than mammographically than ER-positive cancers
Are more likely to be diagnosed as interval cancers between mammograms:
However, intrinsic differences in the density of breast tissue among women diagnosed with TNBC may also explain these differences in presentation
Pathologic characteristics:
TNBC are usually:
High grade
The most common histology is:
Infiltrating ductal carcinoma:
Although a rare histologic subtype:
Medullary carcinoma:
Is generally triple negative
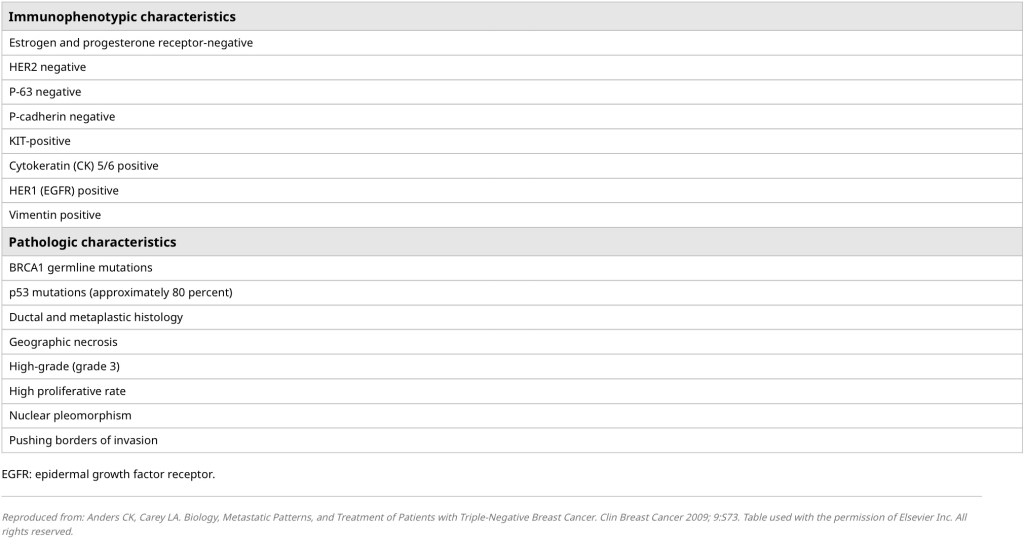
TNBCs can exhibit geographic necrosis, a pushing border of invasion, and a stromal lymphocytic response (Table)
Immunophenotypic and pathologic features of triple negative breast cancer
An uncommon subgroup of TNBCs:
Is defined histopathologically as metaplastic:
However, this is a diverse group of cancer types ranging from squamous to stromal in nature
By definition:
TNBC lacks immunohistochemical (IHC) expression of the:
ER, PR, and HER2
Since these three biomarkers represent the only known approved targets for breast cancer treatment:
Considerable effort has been made to better understand other biologic forces driving TNBC
Molecular classification of TNBC:
The triple-negative clinical phenotype:
Mostly comprises the basal-like molecular subtype:
Although triple-negative and basal breast cancers are not synonymous and there is substantial heterogeneity within TNBCs:
As examples, in one study of utilizing DNA and RNA profiling of TNBCs:
Four stable subtypes were identified:
Luminal androgen receptor
Mesenchymal
Basal-like immunosuppressed
Basal-like immune-activated
In another study, 172 triple-negative tumors based on IHC staining were correlated with gene expression profiles that defined the basal subtype:
Only 71% of TNBCs were assigned the basal subtype
In a converse analysis (where subtype was identified and correlated with IHC staining) of 160 tumors:
77% of basal tumors were triple negative by IHC
Other evidence from copy number variation and mutational analyses has also suggested wide variability and breadth of clonal spectra in TNBC
Basal breast cancer:
Is characterized by the genomic expression of the “basal cluster,”:
A unique cluster of genes that includes the epidermal growth factor receptor (EGFR, also called HER1), basal cytokeratins 5/6, c-Kit, the proliferation cluster, and low expression of the hormone receptor- and HER2-related genes
Separate subtypes of TNBC have been characterized by gene expression, including:
Two basal-like subtypes (BL1 and BL2)
Immunomodulatory
Mesenchymal
Mesenchymal stem-like
Luminal androgen subtypes
Additional subtypes that have been characterized include:
Claudin-low
Interferon-rich subtypes
Gene expression analysis:
Has also revealed that the tumor suppressor gene p53 (TP53) and several DNA repair genes:
Particularly the breast cancer susceptibility genes (BRCA):
Are either mutated or aberrantly expressed in TNBC
These molecular features may have implications for chemotherapy sensitivity to platinum and other directly DNA-damaging agents
Taken together, these studies have produced mixed results with varying conclusions among the different investigators:
None has reached the level of providing clinical considerations at present
TNBC accounts for approximately 15% of breast cancers diagnosed worldwide:
Which amounts to almost 200,000 cases each year
Compared with hormone receptor-positive breast cancer:
TNBC is more commonly diagnosed in women younger than 40 years:
In one study, there was a twofold higher attributable risk of TNBC in women under 40 years compared with women over 50 years (odds ratio [OR] 2.13, 95% CI 1.34-3.39) [5].
In addition, TNBC appears to be relatively more common among Black women compared with White women (OR 2.41, 95% CI 1.81-3.21)
Risk factors associated with the diagnosis of TNBC include:
Positive BRCA mutation status:
Up to 20% of patients with TNBC harbor a breast cancer susceptibility gene (BRCA) mutation:
Particularly in BRCA1
By contrast, less than 6% of all breast cancers are associated with a BRCA mutation
Given this finding, any patient with triple-negative disease should be offered a referral to a genetic counselor to discuss BRCA germline testing:
Moreover, any patient age 60 years or younger with TNBC should undergo BRCA germline testing
Race / ethnicity:
Several population-based studies have found that African American women have a higher risk of TNBC compared with White women:
However, African American women can certainly have ER-positive and / or HER2-positive disease:
Testing their tumors for these markers is essential
Premenopausal status:
Premenopausal status has been associated with increased incidence of TNBC diagnosis as compared with postmenopausal status
As with African American women:
Premenopausal women can frequently have ER-positive and / or HER2-positive disease:
Testing their tumors for these markers is essential
Other factors:
Studies have suggested relationships between other factors such as obesity and a young age of first pregnancy with an increased risk of TNBC:
While breastfeeding and parity may be associated with lower risks:
However, these factors are less well validated and rarely factor into clinical considerations