A “white plaque of questionable risk having excluded other known diseases or disorders that carry no increased risk for cancer”
It is the most common oral potentially malignant disorder (OPMD) in North America and Europe:
With a prevalence ranging from 0.1% to 33%
Definition:
Oral leukoplakia (OL) is a predominantly white patch or plaque on the oral mucosa:
That cannot be characterized clinically or pathologically as any other disorder
It is a diagnosis of exclusion:
Conditions such as:
Frictional keratosis, lichen planus, candidiasis, and other identifiable white lesions must be ruled out before the term is applied
A final diagnosis of leukoplakia in cases with an identifiable causative factor (e.g., friction, tobacco):
Can only be made in retrospect after failure to resolve within 4 to 8 weeks of eliminating the suspected cause
Pathophysiology:
Leukoplakia represents a spectrum of epithelial alterations:
Driven by accumulating somatic – genomic alterations
The molecular progression model involves:
Sequential loss of heterozygosity (LOH) at specific chromosomal loci:
Early losses at 9p21 (p16 inactivation) and 3p21, followed by 17p13 (p53 mutation), 11q13 (cyclin D1 amplification), and later losses at 4q, 8p, 13q, and 14q
Tumor progression from OL:
OIs promoted by somatic genomic alterations, immune evasion, and abrogation of effective immune responses against cancer cells
Overexpression of p53 and deletions /mutations in KMT2C, p16INK4a, and p14ARF genes have been identified:
Particularly in proliferative verrucous leukoplakia (PVL)
Microbial dysbiosis:
May also contribute to a chronic inflammatory microenvironment favoring epithelial transformation
Etiology and Risk Factors:
Tobacco and alcohol consumption:
Are the most common risk factors
However, OL can also occur in non-smokers — notably:
Most patients with PVL have never smoked:
Yet PVL carries the highest malignant transformation rates (70% to 100%)
Additional risk factors include:
Betel quid / areca nut use
Immunosuppression:
HIV-positive patients with OL are more likely to develop oral cancer
Clinical Presentation:
OL typically presents as:
A white, adherent plaque that cannot be scraped off:
Lesions are largely asymptomatic
Two clinical subtypes are recognized:
Homogeneous leukoplakia:
Uniformly white, flat, thin plaques with a smooth or slightly wrinkled surface
These carry a lower risk of malignant transformation
Nonhomogeneous leukoplakia:
Mixed red-and-white lesions (erythroleukoplakia), nodular, verrucous, or speckled variants
These carry a significantly higher risk of malignant transformation
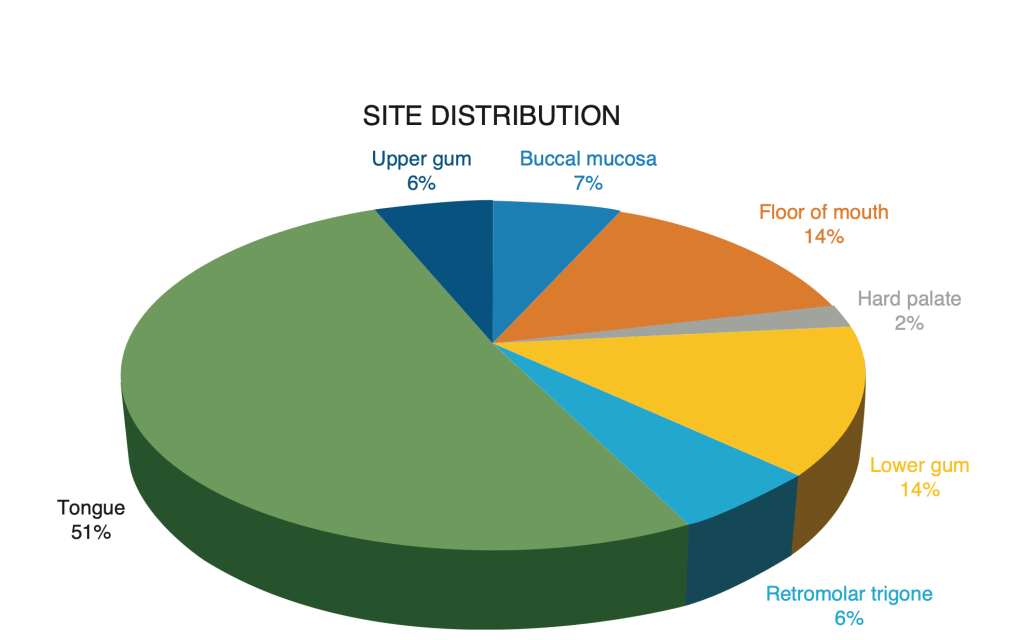
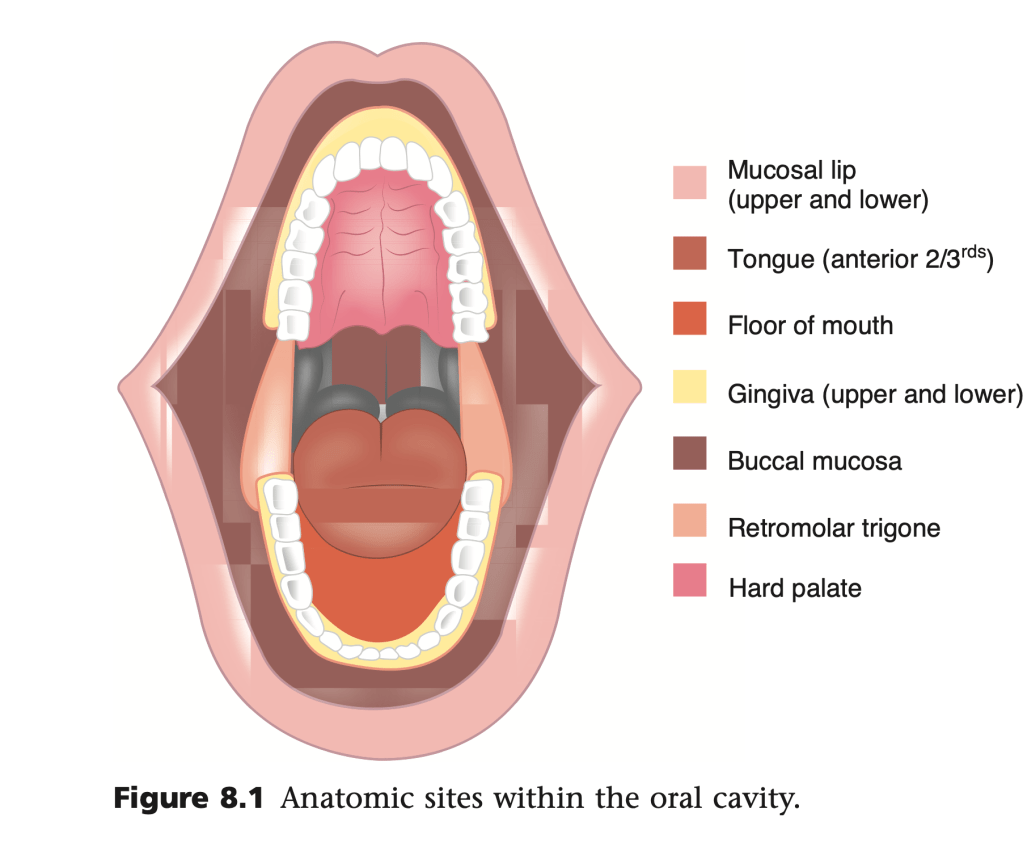
Common sites include:
The lateral / ventral tongue, floor of mouth, soft palate, buccal mucosa, and gingiva
Proliferative verrucous leukoplakia (PVL):
A distinct aggressive subtype, is characterized by multifocal keratotic plaques with progressive expansion, high recurrence, and strong malignant potential
Histology:
Histopathology of leukoplakia can reveal a range of findings:
Hyperkeratosis (orthokeratosis or parakeratosis) without dysplasia:
Carcinoma in situ or invasive squamous cell carcinoma:
May be found on biopsy of clinically apparent leukoplakia
Importantly, frank dysplasia is more frequently found in isolated (unifocal) leukoplakia than in PVL:
Yet PVL has a much higher malignant transformation rate (~ 50% vs. ~ 9.5%), underscoring that histologic grade alone does not fully predict risk
Management:
Management is guided by histopathologic findings and clinical risk factors:
All leukoplakias should be biopsied regardless of clinical impression:
As the decision to biopsy based on visual assessment alone has low sensitivity (59.6%) and low specificity (62.1%) for identifying cancer
Benign (no dysplasia):
Active surveillance with periodic clinical examination, or treatment with topical therapy
Risk factor modification (tobacco and alcohol cessation) is essential
Dysplastic lesions:
Surgical excision:
Scalpel or laser ablation – is the standard approach
CO₂ laser ablation and photodynamic therapy have also been used
Chemoprevention:
Vitamin A, retinoids, beta-carotene, and lycopene have shown some short-term efficacy in clinical resolution of lesions but no treatment has been proven to prevent long-term malignant transformation in RCTs
Relapses and adverse effects are common
Close follow-up is mandatory regardless of treatment, as recurrence rates are high (37.5% in one series) and malignant transformation can occur even after complete excision:
The American Dental Association (2026) recommends routine clinical oral examination for all adults, including systematic visual inspection and palpation to detect OPMDs early
Prognosis and Malignant Transformation:
The mean malignant transformation rate of OL is approximately:
3.5% (range 0.13% to 34%) across studies:
With an estimated annual rate of ~1.5% to 2% per year
A large population-based cohort study (n = 4,886) found a 5-year absolute risk of oral cancer of 3.3% overall, stratified by dysplasia grade:
No dysplasia: 2.2%
Mild dysplasia: 11.9%
Moderate dysplasia: 8.7%
Severe dysplasia: 32.2%
Critically, 39.6% of cancers arose from biopsied leukoplakias without dysplasia:
Highlighting that absence of dysplasia does not eliminate risk
Risk factors for malignant transformation include:
Female sex
Lesion area > 200 mm²
Epithelial dysplasia
Nonhomogeneous type
Tongue location
Immunosuppression
References:
Common Tongue Conditions in Primary Care. Straub L, Schettini P, Myrex P. American Family Physician. 2024;110(5):467-475.
Oncological Outcomes of Patients With Oral Potentially Malignant Disorders. Villa A, Lodolo M, Ha P. JAMA Otolaryngology– Head & Neck Surgery. 2025;151(1):65-71. doi:10.1001/jamaoto.2024.3719.
Oral Leukoplakia, the Ongoing Discussion on Definition and Terminology. van der Waal I. Medicina Oral, Patologia Oral Y Cirugia Bucal. 2015;20(6):e685-92. doi:10.4317/medoral.21007.
Molecular Markers of the Risk of Oral Cancer. Lippman SM, Hong WK. The New England Journal of Medicine. 2001;344(17):1323-6. doi:10.1056/NEJM200104263441710.
Head and Neck Cancer. Forastiere A, Koch W, Trotti A, Sidransky D. The New England Journal of Medicine. 2001;345(26):1890-900. doi:10.1056/NEJMra001375.
Microbial Dysbiosis and Host-Microbe Interactions in Proliferative Verrucous Leukoplakia: Insights Into Carcinogenic Potential. Špiljak B, Ozretić P, Brailo V, et al. Archives of Microbiology. 2025;208(1):65. doi:10.1007/s00203-025-04611-w. Head and Neck Cancer. Dunn LA, Ho AL, Pfister DG. JAMA. 2025;:2842834. doi:10.1001/jama.2025.21733.
Oral Leukoplakia and Oral Cavity Squamous Cell Carcinoma. Bewley AF, Farwell DG. Clinics in Dermatology. 2017 Sep – Oct;35(5):461-467. doi:10.1016/j.clindermatol.2017.06.008.
Oral Potentially Malignant Disorders. Wetzel SL, Wollenberg J. Dental Clinics of North America. 2020;64(1):25-37. doi:10.1016/j.cden.2019.08.004.
Proliferative Verrucous Leukoplakia: An Expert Consensus Guideline for Standardized Assessment and Reporting. Thompson LDR, Fitzpatrick SG, Müller S, et al. Head and Neck Pathology. 2021;15(2):572-587. doi:10.1007/s12105-020-01262-9.
Leukoplakia-a Diagnostic and Management Algorithm. Villa A, Woo SB. Journal of Oral and Maxillofacial Surgery : Official Journal of the American Association of Oral and Maxillofacial Surgeons. 2017;75(4):723-734. doi:10.1016/j.joms.2016.10.012.
Potentially Malignant Disorders of the Oral Cavity and Oral Dysplasia: A Systematic Review and Meta-Analysis of Malignant Transformation Rate by Subtype. Iocca O, Sollecito TP, Alawi F, et al. Head & Neck. 2020;42(3):539-555. doi:10.1002/hed.26006.
Clinical Management Update of Oral Leukoplakia: A Review From the American Head and Neck Society Cancer Prevention Service. Gates JC, Abouyared M, Shnayder Y, et al. Head & Neck. 2025;47(2):733-741. doi:10.1002/hed.28013.
Oral Leukoplakia and Risk of Progression to Oral Cancer: A Population-Based Cohort Study. Chaturvedi AK, Udaltsova N, Engels EA, et al. Journal of the National Cancer Institute. 2020;112(10):1047-1054. doi:10.1093/jnci/djz238.
Randomized Controlled Trials for Oral Leukoplakia. Lodolo M, Valor J, Villa A. Oral Diseases. 2025;. doi:10.1111/odi.15399.
Management of Oral Leukoplakia by Ablative Fractional Laser-Assisted Photodynamic Therapy: A 3-Year Retrospective Study of 48 Patients. Yao YL, Wang YF, Li CX, Wu L, Tang GY. Lasers in Surgery and Medicine. 2022;54(5):682-687. doi:10.1002/lsm.23534.
Interventions for Treating Oral Leukoplakia to Prevent Oral Cancer. Lodi G, Franchini R, Warnakulasuriya S, et al. The Cochrane Database of Systematic Reviews. 2016;7:CD001829. doi:10.1002/14651858.CD001829.pub4.
Living evidence-informed guideline on the early detection of oral squamous cell carcinoma and potentially malignant disorders. Olivia Urquhart. American Dental Association (2026).
Long-Term Outcome of Non-Surgical Treatment in Patients With Oral Leukoplakia. Kuribayashi Y, Tsushima F, Morita KI, et al. Oral Oncology. 2015;51(11):1020-1025. doi:10.1016/j.oraloncology.2015.09.004.
Changed adjuvant decision-making for patients with HR-positive, HER2-negative early breast cancer with 1 to 3 positive axillary nodes:
By showing that the value of chemotherapy depends heavily on menopausal status:
When the 21-gene recurrence score (Oncotype DX RS) is 0 to 25
The key practice-changing message is that postmenopausal women with RS 0 to 25:
Generally do not benefit from adjuvant chemotherapy:
Whereas premenopausal women with the same RS range do appear to benefit
Trial design:
RxPONDER was a prospective randomized phase III trial enrolling more than 5,000 women with HR-positive, HER2-negative breast cancer, 1 to 3 positive lymph nodes, and an RS of 25 or lower
Patients were randomized to endocrine therapy alone or chemoendocrine therapy
The central goal was to determine whether recurrence score could identify node-positive patients who could safely avoid chemotherapy
Main result:
In the overall study population, the effect of chemotherapy differed by menopausal status:
Among postmenopausal women:
Adding chemotherapy did not improve invasive disease–free survival
Among premenopausal women:
Chemotherapy did improve invasive disease–free survival and distant relapse–free survival:
This interaction is the most important clinical takeaway from the study
Postmenopausal patients:
For postmenopausal patients with 1 to 3 positive nodes and RS 0 to 25:
Chemotherapy can usually be omitted without compromising outcomes:
This is the group in which RxPONDER most clearly supports de-escalation
For the surgeon, this means that limited nodal positivity alone no longer automatically implies a chemotherapy recommendation in HR-positive / HER2-negative disease
Premenopausal patients:
For premenopausal patients with 1 to 3 positive nodes and RS 0 to 25:
Chemotherapy was associated with a statistically significant benefit
The trial did not prove whether that benefit came from cytotoxic therapy itself, chemotherapy-induced ovarian suppression, or both:
So multidisciplinary interpretation remains important
Current NCCN educational guidance reflects this nuance:
Noting that in premenopausal patients the assay may help frame discussion of alternatives such as ovarian function suppression, but chemotherapy and ovarian suppression are not yet proven interchangeable
What it means for the surgical oncologist:
RxPONDER matters because it directly affects postoperative counseling after lumpectomy or mastectomy when final pathology shows 1 to 3 positive nodes
The surgeon should anticipate genomic testing in appropriate ER-positive / HER2-negative patients and should understand that:
Node-positive does not automatically mean chemotherapy
Menopausal status is central to interpretation:
In postmenopausal patients with RS 0 to 25:
Chemotherapy can often be avoided
In premenopausal patients with RS 0–25:
Chemotherapy is still generally recommended unless the medical oncology discussion supports a different endocrine-based strategy
Practical surgical takeaway:
For a surgical oncologist:
RxPONDER shifts the conversation from “How many nodes are positive?” to “What is the biology, and is the patient premenopausal or postmenopausal?”
In modern breast practice, a patient with 1 to 3 positive nodes and favorable genomics may still avoid chemotherapy if she is postmenopausal:
But a similar premenopausal patient usually still merits strong consideration of chemotherapy
Bottom line:
RxPONDER showed that for HR-positive, HER2-negative early breast cancer with 1 to 3 positive nodes and Oncotype DX RS 0 to 25, postmenopausal women do not derive meaningful chemotherapy benefit, while premenopausal women do:
That is the key message that should guide surgical counseling and multidisciplinary adjuvant planning
Key references:
Kalinsky K, Barlow WE, Gralow JR, et al. 21-Gene Assay to Inform Chemotherapy Benefit in Node-Positive Breast Cancer. N Engl J Med. 2021;385:2336-2347.
NCCN educational update on biomarkers in early-stage breast cancer, summarizing current use of the 21-gene assay in node-positive disease.
Was the first large prospective randomized trial to test whether the 70-gene signature (MammaPrint):
Could help spare adjuvant chemotherapy in patients with early breast cancer:
Especially when clinical risk and genomic risk disagreed
Its key contribution was showing that some patients who appear high-risk by traditional clinicopathologic criteria:
Still have an excellent outcome without chemotherapy if they are genomically low-risk
Trial design:
MINDACT enrolled 6,693 women with early-stage breast cancer
Patients were assigned both a clinical risk estimate and a genomic risk estimate:
Clinical risk was based on:
A modified Adjuvant! Online tool
Genomic risk was based on:
The 70-gene signature
Patients with concordant low risk generally avoided chemotherapy
Those with concordant high risk received it
Those with discordant risk:
Were randomized to treatment decisions based on either the clinical or genomic result:
The primary test population was the clinical high-risk / genomic low-risk group
Primary finding:
In patients with high clinical risk but low genomic risk:
Who did not receive chemotherapy:
The 5-year distant metastasis-free survival (DMFS) was 94.7% (95% CI 92.5–96.2):
Which met the study’s predefined benchmark for safety
This was the practice-changing result:
It supported omission of chemotherapy in selected patients despite unfavorable conventional features
Longer-term follow-up:
With longer follow-up, the benefit of chemotherapy in the clinical high-risk / genomic low-risk group remained small overall
The 2021 update reported that the 8-year DMFS for this group was 92.0% with chemotherapy vs 89.4% without chemotherapy, an absolute difference of 2.6 percentage points
The authors concluded that the 70-gene signature continues to identify a group with excellent outcomes and only a limited average chemotherapy benefit
Age-related nuance:
The most important nuance for multidisciplinary decision-making is age
In the updated analysis, the apparent chemotherapy benefit was not seen in women older than 50 years, while a potentially clinically relevant benefit appeared in women 50 years or younger
This raises the same question seen in other adjuvant trials:
How much of the effect reflects true cytotoxic benefit versus ovarian suppression / menopausal effect in younger patients
For the surgeon, this means a low-genomic-risk result should still be interpreted in the context of menopausal status and age
Node-positive relevance:
A major practical strength of MINDACT is that it included not only node-negative disease but also patients with 1 to 3 positive nodes:
Making it more broadly relevant than node-negative-only genomic trials
For surgical oncologists, this is especially useful after lumpectomy or mastectomy when pathology shows limited nodal disease and the team is deciding whether anatomy alone should drive chemotherapy recommendations
Ultralow-risk subgroup:
A later MINDACT analysis identified an ultralow-risk subgroup by the 70-gene assay
These patients had exceptionally favorable outcomes:
Including an 8-year distant metastasis-free interval of 97.0% and 8-year breast cancer-specific survival above 99%
This supports even more confidence in de-escalation discussions in carefully selected patients with highly favorable biology
What this means for the surgical oncologist:
MINDACT matters because it reinforces that postoperative planning in early breast cancer is no longer based on tumor size, grade, and nodal status alone:
A patient with a large tumor or limited nodal involvement may still have a genomically low-risk cancer with only modest absolute chemotherapy benefit
In practical terms:
A surgeon should think about which ER-positive / HER2-negative patients may benefit from genomic testing as part of adjuvant planning
A clinical high-risk / genomic low-risk result can support a discussion about omitting chemotherapy, particularly in older than 50 patients
In younger / premenopausal patients, especially with higher tumor burden or limited node-positive disease:
The discussion remains more nuanced and should be individualized
Bottom line:
MINDACT showed that biology can meaningfully refine risk beyond standard pathology
For the surgical oncologist, the main takeaway is that a patient who looks high-risk on anatomic grounds may still have a sufficiently favorable genomic profile to justify avoiding adjuvant chemotherapy:
Particularly if she is older than 50 years and has ER-positive / HER2-negative early breast cancer
Key references:
Cardoso F, van’t Veer LJ, Bogaerts J, et al. 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. N Engl J Med. 2016;375:717-729.
Piccart M, van’t Veer LJ, Poncet C, et al. 70-gene signature as an aid for treatment decisions in early breast cancer: updated results of the phase 3 randomised MINDACT trial with an exploratory analysis by age. Lancet Oncol. 2021;22:476-488.
Lopes Cardozo JMN, Drukker CA, Rutgers EJT, et al. Outcome of Patients With an Ultralow-Risk 70-Gene Signature in the MINDACT Trial. J Clin Oncol. 2022;40:1335-1345.
TAILORx (Trial Assigning Individualized Options for Treatment):
Was the landmark prospective trial that validated use of the 21-gene recurrence score (Oncotype DX):
To guide adjuvant chemotherapy decisions in women with:
HR-positive, HER2-negative, axillary node-negative early breast cancer
Its main practice-changing contribution was showing that:
Most women with an intermediate recurrence score:
Do not benefit from adjuvant chemotherapy:
Particularly those older than 50 years
Study design:
The trial enrolled:
9,719 women with HR-positive, HER2-negative, node-negative breast cancer
Patients with a recurrence score (RS) 0 to 10 received endocrine therapy alone; those with RS 26 to 100 received chemoendocrine therapy; and those with RS 11 to 25 were randomized to endocrine therapy alone versus chemoendocrine therapy
Primary result:
Among women with RS 11 to 25:
Endocrine therapy alone was noninferior to chemoendocrine therapy for invasive disease–free survival:
At 9 years:
Invasive disease–free survival was 83.3% with endocrine therapy alone versus 84.3% with chemoendocrine therapy
Distant recurrence rates were also very similar:
This established that for the overall randomized group:
Adding chemotherapy did not provide a clinically meaningful benefit
Age-specific nuance:
The critical nuance from TAILORx is age
In women 50 years or younger:
There appeared to be some chemotherapy benefit in subsets with RS 16 to 25:
Especially at the upper end of that range
By contrast, women older than 50 with RS 11 to 25 generally did not benefit from chemotherapy
The NCI summary estimated that chemotherapy can be safely avoided in about 70% of women with this common breast cancer subtype, including:
Any age with RS 0 to 10
Age > 50 with RS 11 to 25
Age ≤ 50 with RS 11 to 15
Low-score group (RS 0 to 10):
The earlier prospective TAILORx report showed that women with RS 0 to 10 treated with endocrine therapy alone had very low recurrence rates:
Supporting omission of chemotherapy in this low-risk group
High-score group (RS 26 to 100):
Patients with RS 26 to 100 were assigned to chemotherapy plus endocrine therapy
Follow-up analyses supported the standard recommendation to offer chemotherapy to this high-risk group:
NCI reported that women in this category had strong 5-year outcomes with chemoendocrine therapy:
Reinforcing that these patients should still be considered for systemic intensification rather than endocrine therapy alone
Clinical risk analysis:
A secondary analysis integrating clinical risk (tumor size and grade) found that clinical risk adds prognostic information:
But was not clearly predictive of chemotherapy benefit in the overall population:
However, in women 50 years or younger, chemotherapy benefit was more apparent in those with RS 16 to 20 and high clinical risk, and in those with RS 21 to 25 regardless of clinical risk
Practical takeaways for the surgical oncologist:
TAILORx matters because it reframes postoperative discussions after definitive surgery in node-negative HR+ / HER2- disease:
Genomic testing is central to adjuvant planning after surgery in appropriate patients
TAILORx made the recurrence score part of standard decision-making:
Not just a prognostic adjunct
Chemotherapy can often be omitted in postmenopausal or older patients with RS 11 to 25:
Which is highly relevant when counseling patients after lumpectomy or mastectomy
In premenopausal or younger patients, especially ≤v50 years with RS 16 to 25:
The conversation is more nuanced:
These patients may derive benefit from chemotherapy:
Though some experts note that part of this benefit may reflect ovarian function suppression rather than direct cytotoxic effect alone
TAILORx applies to node-negative disease
For 1 to 3 positive nodes:
The more relevant prospective trial is RxPONDER, not TAILORx
Bottom line:
TAILORx changed practice by showing that adjuvant chemotherapy is unnecessary for most women with node-negative HR-positive / HER2-negative early breast cancer who have a midrange Oncotype DX recurrence score, particularly those older than 50
The major exception is the younger / premenopausal subgroup with RS 16 to 25:
Where chemotherapy may still offer benefit and multidisciplinary discussion remains essential
Key references:
Sparano JA, Gray RJ, Makower DF, et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N Engl J Med. 2018;379:111-121.
Sparano JA, Gray RJ, Ravdin PM, et al. Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer. N Engl J Med. 2019;380:2395-2405.
National Cancer Institute. TAILORx trial finds most women with early breast cancer do not benefit from chemotherapy. 2018. National Cancer Institute PDQ. Breast Cancer Treatment (PDQ®), updated 2025.
🧬 Interesting biology Good responders showed reduction in FOXP3+ Tregs, suggesting immune-microenvironment modulation.
⚠️ Safety Grade ≥3 toxicity: 14.7% No treatment-related deaths.
💡 Why this matters
Borderline OSCC often fails surgery after standard NACT. This low-dose IO + metronomic + chemo strategy may offer an affordable outpatient approach in LMIC settings.
But this is single-arm Phase II → randomized validation needed.
Context: Patients with elevated parathyroid hormone (PTH) and consistently normal serum calcium levels, in whom secondary causes of hyperparathyroidism have been excluded, may represent the earliest presentation of primary hyperparathyroidism (PHPT).
Objective: The objective of the study was to characterize patients with normocalcemic PHPT referred to a bone disease unit.
Design: This was a longitudinal cohort study.
Setting: Ambulatory patients were referred to the metabolic bone disease unit.
Patients: The study population included 37 patients [aged 58 yr, range 32–78; 95% female; serum calcium, 9.4 ± 0.1 (SEM) mg/dl (2.3 ± 0.02 mmol/liter), reference range, 8.5–10.4 (2.1–2.6 mmol/liter); PTH, 93 ± 5 pg/ml].
Interventions: Interventions included yearly (median 3 yr; range 1–8 yr) physical examination, biochemical indices, and bone mineral density (BMD).
Main Outcome Measures: We measured the development of features of PHPT.
Results: Evaluation for classical features of PHPT revealed a history of kidney stones in five (14%), fragility fractures in four (11%), and osteoporosis in 57% [spine (34%), hip (38%), and/or distal one third radius (28%)]. BMD did not show preferential bone loss at the distal one third radius (T scores: spine, −2.00 ± 0.25; hip, −1.84 ± 0.18; one third radius, −1.74 ± 0.22). Further signs of PHPT developed in 40% (seven hypercalcemia; one kidney stone; one fracture; two marked hypercalciuria; six had >10% BMD loss at one or more site(s) including four patients developing World Health Organization criteria for osteoporosis). Seven patients (three hypercalcemic, four persistently normocalcemic) underwent successful parathyroidectomy.
Conclusions: Patients seen in a referral center with normocalcemic hyperparathyroidism have more substantial skeletal involvement than is typical in PHPT and develop more features and complications over time. These patients may represent the earliest form of symptomatic, rather than asymptomatic, PHPT.
Lowe, Hyesoo et al. “Normocalcemic primary hyperparathyroidism: further characterization of a new clinical phenotype.” The Journal of clinical endocrinology and metabolism 92 8 (2007): 3001-5 .
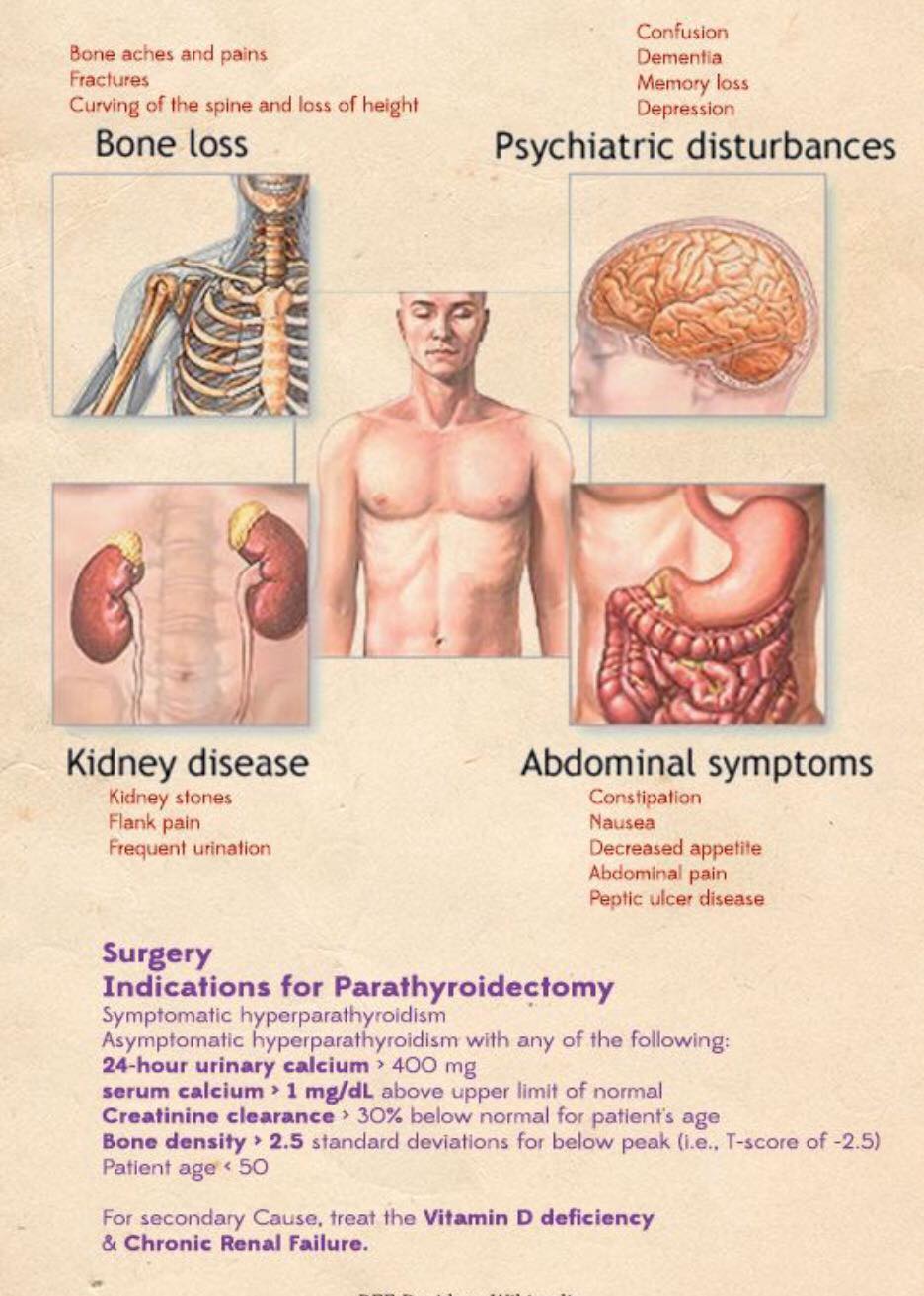
Thinning of the hair (specially in women in the frontal region)
Pruritus
Patients with PHPT also tend to score lower than healthy controls when evaluated by general multidimensional health assessment tools such as the Medical Outcomes Study Short-Form Health Survey(SF-36) and other specific questionnaires.
PHPT that is truly “asymptomatic” is a rare occurrence:
Seen in less than five percent of patients:
This is important when talking about management based on current guidelines
Patients with PHPT have some degree of renal dysfunction or symptoms:
In approximately 80% of the cases:
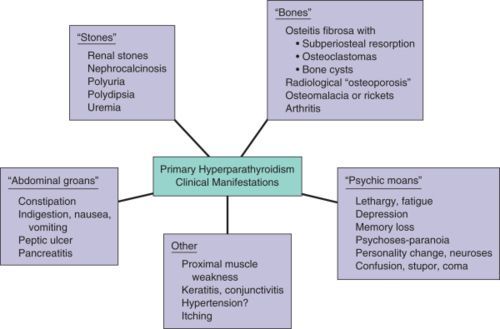
The renal manifestations implicated with PHPT are:
Decreased glomerular filtration rate
Hypercalciuria
Nephrolithiasis:
Nephrolithiasis was previously reported in approximately 40% to 80% of patients but now occur only in about 20% to 25% of the cases:
The pathophysiology is thought to be related to the filtered load of calcium in the glomerulus that increases proportionately with the degree of hypercalcaemia
Most renal stones in patients with PHPT are composed of calcium oxalate, although slightly alkaline urine may favor the precipitation of calcium phosphate stones:
Stone formers are more likely to be hypercalciuric, but less than one-third of the hypercalciuric patients with PHPT actually develop renal stones
Hypercalciuria is not a predictor of nephrolithiasis in patients with PHPT and is no longer considered as an indication for surgery
Nephrocalcinosis
Impaired urinary concentrating ability sometimes leading to polyuria, polydipsia, and nocturia
Reduced fractional phosphate reabsorption leading to hypophosphatemia
Increased urinary exertion of magnesium
Rodrigo Arrangoiz MS, MD, FACS, FSSO head and neck surgeon that specializes in parathyroid diseases that is a member of Mount Sinai Medical Center
Rodrigo Arrangoiz MS, MD, FACS, FSSO is a member of the American Thyroid Association: