- Hypoparathyroidism (hypoPT):
- Is the most common complication of bilateral and re-operative thyroid operations
- The true incidence of postoperative hypoPT is debatable:
- Because of significant heterogeneity in how it has been studied:
- Different time points after surgery, diverse electrolyte supplementation protocols, thyroid operations of variable aggressiveness, by surgeons of varying expertise, and for a broad array of indications are further confounded by variable use of clinical criteria (symptomatic vs, asymptomatic hypocalcemia), biochemical criteria (serum parathyroid hormone [PTH] and / or calcium and / or ionized calcium), and treatment criteria (requirement for calcium and / or vitamin D supplementation)
- Because of significant heterogeneity in how it has been studied:
- According to a recent meta-analysis:
- The median incidence of temporary hypoPT following thyroidectomy ranges from:
- 19% to 38%
- The median incidence of permanent hypoPT following thyroidectomy ranges from:
- 0% to 3%
- The median incidence of temporary hypoPT following thyroidectomy ranges from:
- It is critically important for the thyroid surgeon to employ strategies for minimizing and preventing hypoPT, including:
- Carrying out the most appropriate extent of thyroidectomy for a specific patient
- Background:
- The short half-life of PTH (3 to 5 minutes), along with the fragile nature of the parathyroid glands:
- Sets the stage for their functional derangement following manipulation
- The etiology of hypoPT:
- Is related to dissection or removal of the vulnerable parathyroid glands during central neck operations:
- Resulting in a decline in circulating PTH
- Is related to dissection or removal of the vulnerable parathyroid glands during central neck operations:
- The short half-life of PTH (3 to 5 minutes), along with the fragile nature of the parathyroid glands:
- Definitions
- Biochemical hypoPT:
- Is defined as a low intact PTH level:
- Below the lower limit of the laboratory standard (usually 12 pg/mL):
- Ranges of normal PTH values vary:
- Depending upon the laboratory
- Ranges of normal PTH values vary:
- Below the lower limit of the laboratory standard (usually 12 pg/mL):
- Accompanied by hypocalcemia:
- Hypocalcemia is a total serum calcium level that is less than the lower limit of the center-specific reference range
- Transient serum calcium values outside the normal reference range:
- May reflect dynamic changes in electrolytes and state of hydration:
- Rather than true hypocalcemia
- May reflect dynamic changes in electrolytes and state of hydration:
- Hypocalcemia may occur independent of hypoPT, but untreated hypoPT always leads to hypocalcemia, even though time lag can range from hours to days.
- Is defined as a low intact PTH level:
- Clinical hypoPT:
- Is defined as biochemical hypoPT that is accompanied by symptoms and / or signs of hypocalcemia
- Parathyroid insufficiency, or relative hypoPT:
- May occur after central neck surgery
- Typically is manifested by clinical symptoms of hypoPT that require medical treatment:
- Despite measured laboratory values within normal ranges
- Transient or temporary hypoPT:
- Is defined as occurring for less than six months after surgery:
- Permanent hypoPT:
- Is defined as occurring beyond six months after surgery
- Biochemical hypoPT:
- Mechanisms:
- The mechanisms that underlie hypoPT:
- Are related to:
- Disruption of parathyroid gland arterial supply
- Disruption of parathyroid gland venous drainage
- Mechanical injury
- Thermal or electrical injury
- Intentional or inadvertent partial or complete removal
- Are related to:
- Normal parathyroid function requires a rich blood supply:
- A normal parathyroid gland is composed of up to 30% capillary cells
- Parathyroid blood supply is both delicate and complex:
- Requires close attention during thyroidectomy to ensure its preservation
- While the inferior thyroid artery is typically the dominant blood vessel that supplies the parathyroid glands:
- Laser Doppler flowmetry has shown that:
- The superior thyroid artery and vessels within the thymo-thyroid cord (ligament) can dominate in some individuals
- Laser Doppler flowmetry has shown that:
- Impaired PTH secretion results in postoperative hypocalcemia through:
- Inhibition of bone resorption
- Reduction of 1,25-dihyroxyvitamin D synthesis by the kidneys
- Reduced intestinal absorption of calcium
- The mechanisms that underlie hypoPT:
- Symptoms and signs:
- Hypocalcemia causes:
- Neuromuscular excitability and cardiac electrical instability:
- Due to a reduced nerve and muscle cell depolarization threshold
- Neuromuscular excitability and cardiac electrical instability:
- Its most common early symptoms are:
- Paresthesias, or numbness and tingling, of the perioral region and the fingertips
- Muscle stiffness, cramps, and spasms are also common
- Neuropsychiatric symptoms include:
- Confusion, anger, depression, lightheadedness, and irritability
- More sustained muscle contraction may lead to:
- Laryngospasm
- More severe neural excitability:
- May lead to seizures
- Signs of hypocalcemia include:
- Observed or elicited tetany:
- Classic bedside findings are:
- A positive Chvostek sign:
- Facial muscle twitching upon tapping the preauricular region over the facial nerve:
- Present at baseline in up to 25% of people
- Facial muscle twitching upon tapping the preauricular region over the facial nerve:
- A positive Trousseau sign:
- Flexion of the wrist, thumb, and metacarpophalangeal joints and hyperextension of the fingers, upon brachial artery occlusion by inflation of a blood pressure cuff above systolic blood pressure)
- A positive Chvostek sign:
- Classic bedside findings are:
- Cardiovascular signs observed with progressive hypocalcemia include:
- Prolongation of the QT interval that can result in torsades de pointes:
- A form of ventricular tachycardia that may degenerate into ventricular fibrillation.
- Prolongation of the QT interval that can result in torsades de pointes:
- Observed or elicited tetany:
- Hypocalcemia causes:
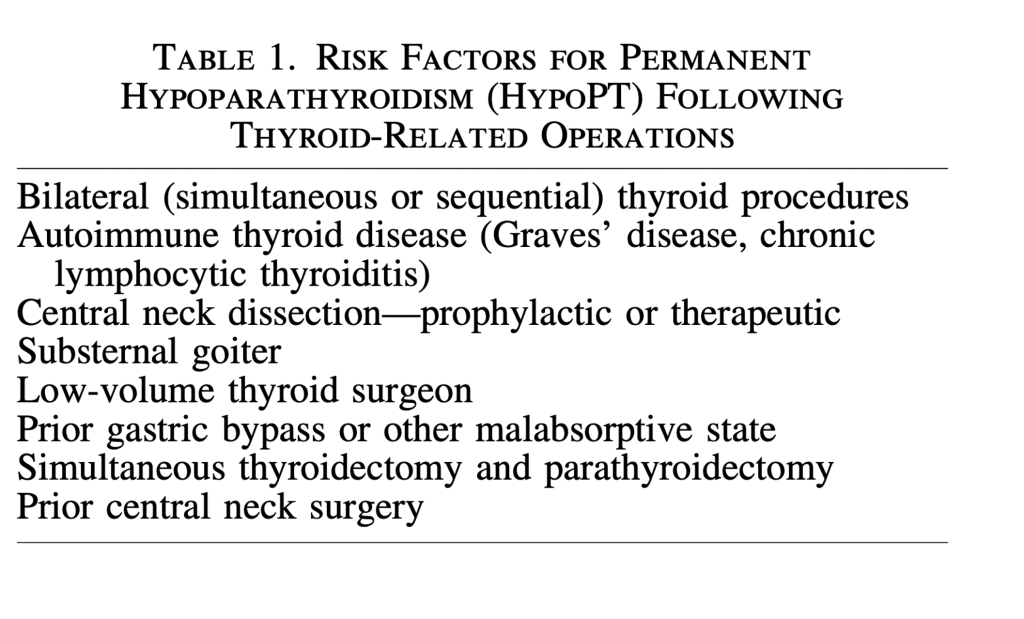
- Risk factors:
- HypoPT may follow any simultaneous or staged bilateral central neck operation
- Risk factors for both temporary and permanent hypoPT are presented in the following Table:
- A prior partial thyroid operation creates a potentially increased risk of hypoPT during completion thyroidectomy:
- Due to unknown status (presence or viability) of the parathyroid glands in the previously operated neck
- The most straightforward way to avoid hypoPT:
- Is to limit the extent of thyroidectomy to a unilateral approach
- Though the historical rationale for a near-total or subtotal thyroidectomy
- Instead of a total thyroidectomy, is in part preservation of the parathyroid glands:
- It has never been adequately studied whether this actually reduces the risk of hypoPT
- Instead of a total thyroidectomy, is in part preservation of the parathyroid glands:
- Parathyroid autotransplantation (PA):
- At the time of thyroidectomy has been associated with an increased risk of temporary hypoPT
- Paradoxically, routine PA may be associated with a reduced risk of permanent hypoPT
- While data supporting propyhylactic PA are not definitive:
- The risk of permanent hypoPT is very low in patients who have undergone autotransplantation of at least one parathyroid gland
- Preoperative vitamin d deficiency:
- When the planned thyroid operation is bilateral:
- Preoperative testing of baseline serum calcium, PTH, and 25-hydroxy vitamin D blood levels can be helpful
- If the baseline calcium is low normal, or below normal:
- The risk of hypoPT is increased:
- It may be appropriate to initiate scheduled oral calcium supplementation preoperatively
- The risk of hypoPT is increased:
- If the baseline calcium level is elevated:
- Then the PTH level should be measured in order to evaluate for occult primary hyperparathyroidism, which could be definitively treated during thyroidectomy
- A preoperatively elevated PTH level is commonly due to secondary hyperparathyroidism from vitamin D deficiency:
- Vitamin D increases the absorption of calcium from the intestinal tract, and supplementation may be helpful to patients with hypoPT:
- Assuming no underlying malabsorptive condition is present
- Vitamin D also increases bone resorption and decreases renal excretion of calcium and phosphate
- Vitamin D deficiency can be:
- Severe – below the lowest recordable level, less than 10 ng/mL
- Moderate – 10 to less than 20 ng/ mL
- Mild (20 to 30 ng/mL
- Vitamin D increases the absorption of calcium from the intestinal tract, and supplementation may be helpful to patients with hypoPT:
- To optimize postoperative oral calcium absorption:
- It is prudent to treat vitamin D deficiency preoperatively:
- The Food and Drug Administration (FDA) approved regimen is:
- 50,000 IU of vitamin D3 (cholecalciferol) weekly or 6000 IU daily for eight weeks
- More aggressive regimens and other vitamin D supplements are available, but their utilization should be considered off-label
- The Food and Drug Administration (FDA) approved regimen is:
- It is prudent to treat vitamin D deficiency preoperatively:
- Not all studies have substantiated improved postoperative calcium levels with higher preoperative vitamin D levels:
- Lang et al. found the rate of clinically significant hypocalcemia after total thyroidectomy to be similar in patients with severe, moderate, and mild vitamin D deficiency, whereas Al-Khatib et al. found that severe 25-hydroxyvitamin D deficiency was an independent predictor of hypoPT in patients undergoing total thyroidectomy:
- However, a large meta-analysis reported that the perioperative PTH level, the preoperative vitamin D level, and postoperative changes of calcium were biochemical predictors of post-thyroidectomy hypocalcemia
- Given the present evidence, it would appear preferable to diagnose vitamin D deficiency and initiate appropriate corrective supplementation prior to surgery
- In cases of elective bilateral thyroid surgery:
- It may be prudent to delay surgery in order to correct severe vitamin D deficiency
- Lang et al. found the rate of clinically significant hypocalcemia after total thyroidectomy to be similar in patients with severe, moderate, and mild vitamin D deficiency, whereas Al-Khatib et al. found that severe 25-hydroxyvitamin D deficiency was an independent predictor of hypoPT in patients undergoing total thyroidectomy:
- When the planned thyroid operation is bilateral:
- References:
- Ho TW, Shaheen AA, Dixon E, Harvey A 2011 Utilization of thyroidectomy for benign disease in the United States: a 15-year population-based study. Am J Surg 201:570–574.
- Hauch A, Al-Qurayshi Z, Randolph G, Kandil E 2014 Total thyroidectomy is associated with increased risk of complications for low- and high-volume surgeons. Ann Surg Oncol 21:3844–3852.
- Brandi ML, Bilezikian JP, Shoback D, Bouillon R, Clarke BL, Thakker RV, Khan AA, Potts JT Jr 2016 Management of hypoparathyroidism: summary statement and guide- lines. J Clin Endocrinol Metab 101:2273–2283.
- Bollerslev J, Rejnmark L, Marcocci C, Shoback DM, Sitges-Serra A, van Biesen W, Dekkers OM 2015 Euro- pean society of endocrinology clinical gideline: treatment of chronic hypoparathyroidism in adults 2015. Eur J En- docrinol 173:G1–20.
- Stack BC Jr, Bimston DN, Bodenner DL, Brett EM, Dralle H, Orloff LA, Pallota J, Snyder SK, Wong RJ, Randolph GW 2015 American Association of Clinical Endocrinologists and American College of Endocrinology disease state clinical review: postoperative hypoparathyroidism—definitions and management. Endocr Pract 21:674–685.
- Lorente-Poch L, Sancho JJ, Mun ̃ oz-Nova JL, Sa ́ nchez- Vela ́zquez P, Sitges-Serra A 2015 Defining the syndromes of parathyroid failure after total thyroidectomy. Gland Surg 4:82–90.
- Mehanna HM, Jain A, Randeva H, Watkinson J, Shaha A 2010 Postoperative hypocalcemia—the difference a defi- nition makes. Head Neck 32:279–283.
- Edafe O, Antakia R, Laskar N, Uttley L, Balasubramanian SP 2014 Systematic review and meta-analysis of predic- tors of post-thyroidectomy hypocalcaemia. Br J Surg 101: 307–320.
- Shoback DM, Bilezikian JP, Costa AG, Dempster D, Dralle H, Khan AA, Peacock M, Raffaelli M, Silva BC, Thakker RV, Vokes T, Bouillon T 2016 Presentation of hypoparathyroidism: etiologies and clinical features. J Clin Endocrinol Metab 101:2300–2312.
- Anastasiou OE, Yavropoulou MP, Papavramidis TS, Tzouvara C, Triantafyllopoulou K, Papavramidis S, Yo- vos JG 2012 Secretory capacity of the parathyroid glands after total thyroidectomy in normocalcemic subjects. J Clin Endocrinol Metab 97:2341–2346.
- Nawrot I, Woz ́ niewicz B, Tołłoczko T, Sawicki A, Go ́ rski A, Chudzin ́ski W, Wojtaszek M, Grzesiuk W, Sladowski D, Karwacki J, Zawitkowska T, Szmidt J 2007 Allo- transplantation of cultured parathyroid progenitor cells without immunosuppression: clinical results. Transplan- tation 83:734–740.
- Johansson K, Ander S, Lennquist S, Smeds S 1994 Human parathyroid blood supply determined by laser-Doppler flowmetry. World J Surgery 18:417–420.
- Shoback D 2008 Clinical practice. Hypoparathyroidism. New Engl J Med 359:391–403.
- Kiernan CM, Schlegel C, Kavalukas S, Isom C, Peters MF, Solorzano CC 2016 Does concomitant thyroidectomy in- crease risks of parathyroidectomy? J Surg Res 203:34–39.
- Thomusch O, Machens A, Sekulla C, Ukkat J, Lippert H, Gastinger I, Dralle H 2000 Multivariate analysis of risk factors for postoperative complications in benign goiter surgery: prospective multicenter study in Germany. World J Surg 24:1335–1341.
- Chiang FY Lin JC, Wu CW, Lee KW, Lu SP, Kuo WR, Wang LF 2006 Morbidity after total thyroidectomy for benign thyroid disease: comparison of Graves’ disease and non-Graves’ disease.Kaohsiung J Med Sci 22:554–559.
- Ebrahimi H, Edhouse P, Lundgren CI, McMullen T, Sidhu S, Sywak M, Delbridge L 2009 Does autoimmune thyroid disease affect parathyroid autotransplantation and surviv- al? ANZ J Surg 79:383–385.
- Viola D, Materazzi G, Valerio L, Molinaro E, Agate L, Faviana P, Seccia V, Sensi E, Romei C, Piaggi P, Torre- grossa L, Sellari-Franceschini S, Basolo F, Vitti P, Elisei R, Miccoli P 2015 Prophylacti central compartment lymph node dissection in papillary thyroid carcinoma: clinical
- implications derived from the first prospective renadomized controlled single institution study. J Clin Endocrinol Metab 100:1316–1324.
- Lang BHH, Ng SH, Lau LLH, Cowling BJ, Wong KP, Wan KY 2013A systematic review and met-analysis of prophylactic central neck dissection on short-term locor- egional recurrence in papillary thyroid carcinoma after total thyroidectomy. Thyroid 23:1087–1098.
- Wang TS, Cheung K, Farrokhyar F, Roman SA, Sosa JA 2013 A meta-analysis of the effect of prophylactic central compartment neck dissection on locoregional recurrence rates in pateints with papillary thyroid cancer. Ann Surg Oncol 20:3477–3483.
- Zetoune T, Keutgen X, Buitrago D, Aldailami H, Shao H, Mazumdar M, Fahey III TJ, Zarnegar R 2010 Prophylactic central neck dissection and local recurrence in papillary thyroid cancer: a meta-analysis. Ann Surg Oncol 17:3287– 3293.
- Giordano D, Valcavi R, Thompson GB, Pedroni C, Renna L, Gradoni P, Barbieri V 2012 Complications of central neck dissection in patients with papillary thyroid carci- noma: results of a study on 1087 patients and review of the literature. Thyroid 22:911–917.
- deCarvalho A, Chulam TC, Kowalski LP 2015 Long- term results of observation vs prophylactic selective le- vel VI neck dissection for papillary thyroid carcinoma at a cancer center. JAMA Otolaryngol Head Neck Surg 141:599–606.
- Kwan WY, Chow TL, Choi CY, Lam SH 2015 Compli- cation rates of central compartment dissection in papillary thyroid cancer. ANZ J Surg 85:274–278.
- Moo TA, Umunna B, Kato M, Butriago D, Kundel A, Lee JA, Zarnegar R, Fahey TJ III 2009 Ipsilateral versus bilat- eral central neck l ymph node dissection in papillary thyroid carcinoma. Ann Surg 250:403–408.
- Barczyn ́ski M, Konturek A, Stopa M, Nowak W 2013 Prophylactic central neck dissection for papillary thyroid cancer. Br J Surg 100:410–418.
- Testini M, Gurrado A, Avenia N, Bellantone R, Biondi A, Brazzarola P, Calzolari F, Cavallaro G, De Toma G, Guida P, Lissidini G, Loizzi M, Lombardi CP, Piccinni G, Portincasa P, Rosato L, Sartori N, Zugni C, Basile F 2011 Does mediastinal extension of the goiter increase mor- bidity of total thyroidectomy? A multicenter study of 19,662 patients. Ann Surg Oncol 18:2251–2259.
- Randolph GW, Shin JJ, Grillo HC, Mathisen D, Katlic MR, Kamani D, Zurakowski D 2011 The surgical man- agement of goiter: Part II. Surgical treatment and results. Laryngoscope 121:68–76.
- Karakas E, Osei-Agyemang T, Schlosser K, Hoffmann S, Zielke A, Rothmund M, Hassan I 2008 The impact of parathyroid auto transplantation during bilateral surgery for Graves’ disease on postoperative hypocalcemia. En- docr Regul 42:39–44.
- Sosa JA, Bowman HM, Tielsch JM, Powe NR, Gordon TA, Udelsman R 1998 The importance of surgeon expe- rience for clinical and economic outcomes from thyroid- ectomy. Ann Surg 228:320–330.
- Kandil E, Noureldine SI, Abbas A, Tufano RP 2013 The impact of surgical volume on patient outcomes following thyroid surgery. Surgery 154:1346–1352.
#Arrangoiz #ThyroidSurgeon #ParathyroidSurgeon #HeadandNeckSurgeon #CancerSurgeon