Why Not All Thyroid Cancers Need Aggressive Treatment
Not all thyroid cancers behave the same. Modern care is personalized—the goal is to treat what matters while avoiding unnecessary treatment.
🧠 The key concept: Risk-adapted management
Many thyroid cancers—especially low-risk papillary thyroid cancers—are:
Slow-growing Unlikely to spread Associated with excellent long-term survival
Because of this, more treatment is not always better.
⚖️ Treatment options today
Depending on risk, options may include:
Active surveillance (careful ultrasound follow-up, no immediate surgery) Thyroid lobectomy instead of total thyroidectomy Selective use of radioactive iodine (not routine for everyone)
➡️ These approaches are evidence-based and safe for appropriately selected patients.
📉 Why avoid overtreatment?
Unnecessary aggressive treatment can:
Increase risk of hypocalcemia and voice changes Require lifelong thyroid hormone replacement Affect quality of life without improving outcomes
🦋 What matters most
Treatment decisions should be guided by:
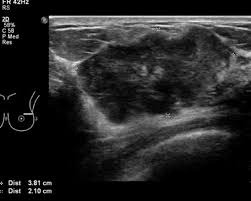
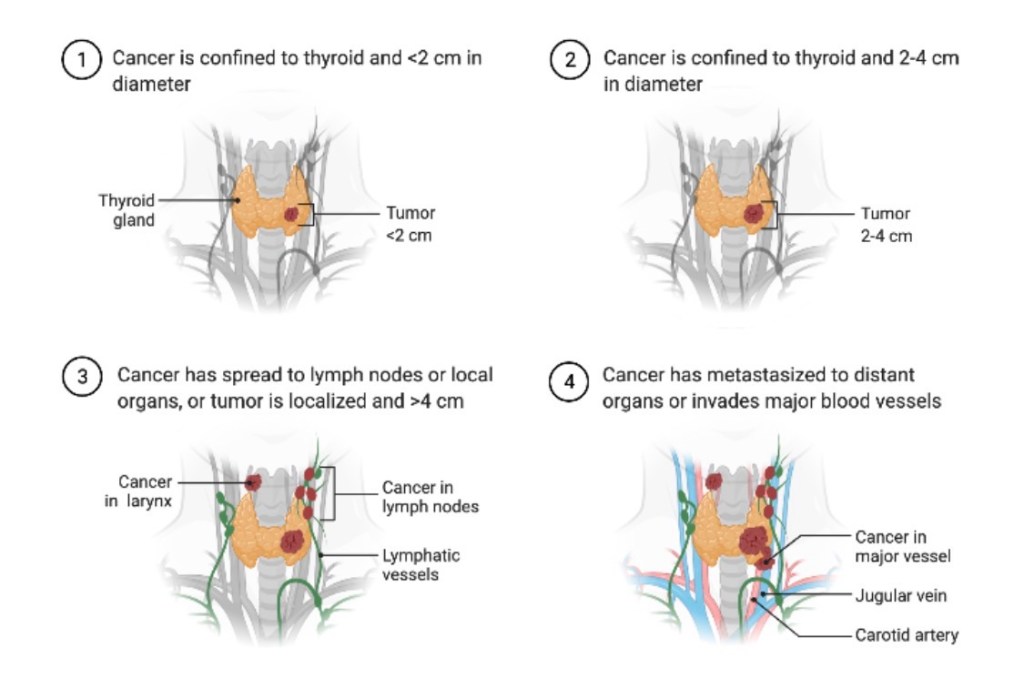
✔️ Tumor size and ultrasound features
✔️ Pathology and risk of recurrence
✔️ Patient age, preferences, and values
✔️ Expertise of a multidisciplinary thyroid team
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
The best thyroid cancer treatment is the right treatment for the right patient—not the most aggressive one.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Tuttle RM et al. Active surveillance for low-risk papillary thyroid cancer. JAMA Brito JP et al. Overdiagnosis and overtreatment of thyroid cancer. BMJ