The NATALEE trial was an open-label, multicenter, randomized phase III trial:
That evaluated the addition of ribociclib to standard endocrine therapy (ET) in patients with stage II to III hormone receptor-positive, HER2-negative early breast cancer
The trial included 2,549 patients receiving ribociclib (400 mg once daily, 3 weeks on, 1 week off) plus ET and 2,552 patients receiving ET alone
At a median follow-up of 27.7 months:
Ribociclib plus ET significantly improved invasive disease-free survival (IDFS) compared to ET alone (HR, 0.75; 95% CI, 0.62 to 0.91; P = .003), with 3-year IDFS rates of 90.4% versus 87.1%, respectively
Additionally, ribociclib plus ET improved distant disease-free survival (DDFS) (HR, 0.74; 95% CI, 0.60 to 0.91)[1]
The American Society of Clinical Oncology (ASCO) recommends:
Considering ribociclib in combination with ET for patients with stage II to III hormone receptor-positive, HER2-negative early breast cancer:
Particularly those with high-risk features
This recommendation is based on the significant IDFS benefit observed in the NATALEE trial
However, ASCO suggests that ribociclib may not provide meaningful clinical benefit to all eligible patients:
Especially those with lower-risk disease, and emphasizes the importance of individual patient factors in decision-making
The NATALEE trial was a pivotal phase III study that evaluated the efficacy and safety of ribociclib in combination with endocrine therapy (ET) in patients with stage II to III hormone receptor-positive, HER2-negative early breast cancer
The trial included 5,101 patients who were randomized to receive either ribociclib (400 mg/day, 3 weeks on/1 week off for 3 years) plus a nonsteroidal aromatase inhibitor (NSAI) or NSAI alone
Premenopausal women and men also received Goserelin
The primary endpoint of the trial was invasive disease-free survival (iDFS)
At a median follow-up of 33.3 months:
Ribociclib plus ET demonstrated a significant improvement in iDFS compared to ET alone:
With a hazard ratio (HR) of 0.749 (95% CI, 0.628-0.892; P = 0.0012)
The 3-year iDFS rates were 90.7% for the ribociclib plus ET group versus 87.6% for the ET alone group
This benefit was consistent across various subgroups, including those with different stages and nodal statuses[2][3][4]
Secondary endpoints, such as distant disease-free survival (DDFS) and recurrence-free survival (RFS), also favored the ribociclib plus ET group
No new safety signals were observed, and the treatment was generally well-tolerated [2][3][4]
Based on the NATALEE trial results, ribociclib in combination with ET is indicated for patients with stage II to III hormone receptor-positive, HER2-negative early breast cancer, particularly those at high risk of recurrence:
This includes patients with node-positive disease and those with additional high-risk features
The trial’s findings support the use of ribociclib as an effective adjuvant therapy to improve iDFS and reduce the risk of recurrence in this patient population [2][3][4]
Freedman RA, Caswell-Jin JL, Hassett M, Somerfield MR, Giordano SH. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2024;42(18):2233-2235. doi:10.1200/JCO.24.00886.
Is a malignancy arising from melanocytes of the skin:
Its incidence has been increasing globally:
Particularly in fair-skinned populations
The incidence of invasive cutaneous melanoma:
Continues to be a major public health concern in the United States:
It has been increasing faster than that of nearly any other cancer over the last 30 years
In 2020, there were an estimated 325,000 new cases and 57,000 deaths due to melanoma worldwide:
The highest incidence rates are observed in Australia and New Zealand:
With rates of 42 per 100,000 person-years for males and 31 per 100,000 person-years for females
Western Europe, North America, and Northern Europe also have high incidence rates
While melanoma remains rare in most African and Asian countries
The incidence of melanoma is closely linked to:
Ultraviolet (UV) radiation exposure:
Both from natural sunlight and artificial sources like tanning beds
This exposure is a significant risk factor, particularly in populations with lighter skin pigmentation
The incidence rates have been rising by approximately 3% to 7% annually over the past decades in white populations:
Driven by changes in outdoor activities and sun exposure behaviors
Mortality rates for melanoma:
Have shown stabilization or decline in some regions, such as the USA, Australia, and parts of Europe:
Likely due to early detection and advances in treatment:
Including the use of immune checkpoint inhibitors and targeted therapies
However, mortality rates remain highest in regions with the highest incidence, such as New Zealand, where they peak at 5 per 100,000 person-years
Projections indicate that if current trends continue:
The global burden of melanoma will increase to 510,000 new cases and 96,000 deaths by 2040, underscoring the need for effective prevention and early detection strategies
According to the analysis by Garbe et al:
Melanoma incidence among US whites is predicted to rise to 56.1 per 100,000 males and 36.2 per 100,000 females by 2036, with a significant portion of this increase expected to occur by 2025
This trend is driven by factors such as increased UV exposure and improved detection methods
Guy et al. projected that melanoma incidence rates would continue to increase for white males and females through 2019, with death rates remaining stable:
Although this projection does not extend to 2025, it supports the trend of rising incidence rates observed in other studies
Whiteman et al. also noted that melanoma rates in US whites increased at more than 3% annually between 1982 and 2011 and are projected to continue rising until at least 2022:
With annual new cases expected to rise significantly due to aging populations and high age-specific rates in the elderly
The American Cancer Society (ACS) projects that in 2025:
There will be approximately 106,110 new cases of melanoma and 7,180 deaths due to melanoma in the United States
The incidence rates for melanoma have been rising by about 2% to 3% annually, driven by changes in sun exposure behaviors and the aging population
Overall, the lifetime risk of being diagnosed with melanoma is about:
2.5% (1 in 40) for whites, 0.1% (1 in 1,000) for blacks, and 0.5% (1 in 200) for Hispanics
The major environmental risk factor, exposure to ultraviolet (UV) radiation, is reflected in geographic and ethnic patterns of melanoma rates
There have also been changes in the distribution and stage of melanoma at diagnosis:
With an overall trend toward thinner T1 / T2 melanomas
References:
Cancer Statistics, 2025. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. CA: A Cancer Journal for Clinicians. 2025 Jan-Feb;75(1):10-45. doi:10.3322/caac.21871
Epidemiology of Skin Cancer: Update 2019. Leiter U, Keim U, Garbe C. Advances in Experimental Medicine and Biology. 2020;1268:123-139. doi:10.1007/978-3-030-46227-7_6.
Targeted treatment with ribociclib plus hormone therapy:
Provided significant invasive disease–free survival benefits in patients with early-stage hormone receptor–positive, HER2-negative breast cancer at risk of disease recurrence
Results from the phase III NATALEE trial, led by researchers at The University of Texas MD Anderson Cancer Center, were presented at the 2023 San Antonio Breast Cancer Symposium (Abstract GS3-03)
Patients who received the combination regimen experienced significantly extended invasive disease–free survival compared to those who received hormone therapy alone:
Which corresponds to a 25% reduction in the risk of recurrence
The invasive disease–free survival rates at 3 years were:
90.7% with the combination and 87.6% with only hormone therapy
The current treatments we have for hormone receptor–positive, HER2-negative early-stage breast cancer:
Only help a small group of patients, which leaves many people with limited options to lower the chances of their cancer coming back
NATALEE trail shows the continued disease-free survival improvement for patients receiving ribociclib with hormone therapy and showed a benefit across clinically relevant subgroups
Study Background
According to the National Cancer Institute, hormone receptor–positive, HER2-negative breast cancer is the most common subtype of the malignancy:
Accounting for nearly 70% of all breast cancer cases in the United States
Approximately one-third of individuals diagnosed with stage II hormone receptor–positive, HER2-negative breast cancer:
Face a risk of recurrence:
Despite receiving standard-of-care treatment
Among those with stage III disease:
More than half experience a recurrence
Ribociclib:
Belongs to a category of targeted therapies known as:
Small-molecule inhibitors
It specifically targets the CDK4 and CDK6 proteins:
Which play a crucial role in regulating cell growth and promoting the growth of breast cancer cells
In 2018, the U.S. Food and Drug Administration granted approval for ribociclib’s use:
In treating advanced hormone receptor–positive, HER2-negative breast cancer
Whileprevious research demonstrated the survival advantages of ribociclib in treating metastatic breast cancer:
The NATALEE trial provided evidence that it could improve outcomes for patients with early-stage breast cancer that hasn’t spread to the lymph nodes
NATALEE Methodology:
The NATALEE trial (ClinicalTrials.gov identifier NCT03701334) enrolled 5,101 men and pre- and postmenopausal women from 20 different countries with:
Stage IIA, IIB, or III hormone receptor–positive, HER2-negative breast cancer at risk for recurrence
Participants were randomly assigned to receive either adjuvant ribociclib for 3 years with hormonal therapy for at least 5 years or hormonal therapy alone for at least 5 years.
The primary endpoint was invasive disease–free survival, and the secondary efficacy endpoints were recurrence-free survival, distant disease–free survival, and overall survival
Results:
Researchers observed consistent benefits across patient subgroups, including those with:
Node-negative, stage II, and stage III disease
Analyses of secondary endpoints of distant disease–free survival and recurrence-free survival supported ribociclib with hormone therapy compared to ribociclib alone
The overall survival data remains incomplete as of now, with 84 events in the ribociclib plus hormone therapy group and a total of 88 events in the hormone therapy alone group
No new safety signals were observed since the prior interim analysis, and side effects were consistent with the known safety profile of ribociclib and nonsteroidal aromatase inhibitors
Researchers will continue to evaluate how adding ribociclib to hormonal therapy impacts quality of life and will follow patients to observe long-term outcomes
Are indicated in early breast cancer primarily for patients with:
Hormone receptor-positive
HER2-negative
Node-positive breast cancer:
At high risk of recurrence
The American Society of Clinical Oncology (ASCO) recommends:
The use of abemaciclib in combination with endocrine therapy (ET) for these patients:
Particularly those who meet the criteria of the intention-to-treat (ITT) population from the monarchE trial:
This includes patients with resected breast cancer with:
≥ 4 positive axillary lymph nodes (ALNs) or 1 to 3 positive ALNs plus additional high-risk features such as grade 3 disease, tumor size ≥ 5 cm, or a Ki-67 index ≥ 20% [1]
The rationale for this recommendation is based on the sustained improvement in invasive disease-free survival (IDFS) observed in the monarchE trial:
With a hazard ratio (HR) of 0.680 and a 5-year absolute improvement in IDFS of 7.6% compared to ET alone [1]
The FDA has expanded the approval of abemaciclib to include patients without the Ki-67 testing requirement:
Acknowledging benefits across the broader ITT population [1]
Ribociclib:
Is another CDK4/6 inhibitor evaluated in the NATALEE trial:
Which included patients with:
Stage II to III hormone receptor-positive
HER2-negative early breast cancer
However, ASCO’s panel suggests that ribociclib may not provide meaningful clinical benefit to all eligible patients:
Especially those with lower-risk disease, and recommends considering individual patient factors such as risks, benefits, costs, and preferences when deciding on its use [1]
The indications for cyclin-dependent kinase 4/6 (CDK4/6) inhibitors in early breast cancer are:
Primarily for patients with hormone receptor-positive (HR+), HER2-negative breast cancer who are at high risk of recurrence
This includes patients with:
Node-positive disease and additional high-risk features
The monarchE trial:
Demonstrated a significant invasive disease-free survival (iDFS) benefit with the use of abemaciclib in combination with endocrine therapy (ET) in patients with:
Node-positive early breast cancer, leading to its approval for this indication [2]
The NATALEE trial:
Evaluated ribociclib in combination with ET in a broad population of patients with:
Stage II or III HR+, HER2-negative early breast cancer
The trial showed a significant iDFS benefit:
With a 25.2% lower risk of invasive disease, recurrence, or death compared to ET alone [2]
Ribociclib was administered at a dose of 400 mg per day:
Which was associated with a lower incidence of dose-dependent toxic effects compared to the higher dose used in advanced breast cancer [2]
The efficacy of CDK4/6 inhibitors in early breast cancer has been variable across different trials:
While the PALLAS and PENELOPE-B trials did not show a significant benefit with palbociclib, the monarchE and NATALEE trials demonstrated significant iDFS benefits with abemaciclib and ribociclib, respectively [2][3]
These findings highlight the importance of patient selection and the specific characteristics of the trials in determining the benefit of CDK4/6 inhibitors in early breast cancer
Mechanisms of Action and Resistance in Estrogen Receptor (ER)–Targeted Therapy. Burstein HJ. Systemic Therapy for Estrogen Receptor-Positive, HER2-Negative Breast Cancer. The New England Journal of Medicine. 2020;383(26):2557-2570. doi:10.1056/NEJMra1307118. The mechanisms of action and resistance in estrogen receptor (ER)-targeted therapy, including the role of CDK4/6 inhibitors in inhibiting cell cycle progression in ER-positive breast cancer. This figure underscores the biological rationale for using CDK4/6 inhibitors in combination with endocrine therapy to improve outcomes in early breast cancer.
Common patient groups that experience a biochemical incomplete response in the context of dynamic risk stratification for differentiated thyroid cancer (DTC) include:
Low-Risk Patients:
Approximately 11% to 19% of patients initially classified as low-risk by the American Thyroid Association (ATA) experience a biochemical incomplete response
These patients typically have persistently abnormal thyroglobulin (Tg) values or rising anti-Tg antibodies without structural evidence of disease
Intermediate-Risk Patients:
This group has a higher incidence, with 21% to 22% of patients experiencing a biochemical incomplete response
These patients often have more aggressive disease features, such as larger tumor size or lymph node involvement, which contribute to the incomplete biochemical response
High-Risk Patients:
Even among high-risk patients, 16% to 18% experience a biochemical incomplete response
These patients are more likely to have advanced disease at diagnosis, including distant metastases or extensive lymph node involvement
Patients with BRAFV600E Mutation:
The presence of the BRAFV600E mutation is significantly associated with a biochemical incomplete response
This mutation is linked to more aggressive disease and a higher likelihood of persistent biochemical evidence of disease
Patients with Higher Preablative Stimulated Tg Levels:
Patients with higher preablative stimulated Tg levels (≥ 12.30 ng/mL) are more likely to experience a biochemical incomplete response
This marker is a robust predictor of persistent disease
These groups highlight the variability in response to initial therapy and underscore the importance of dynamic risk stratification in guiding follow-up and management strategies for DTC patients
Biochemical incomplete response (BIR) in thyroid cancer is characterized by persistently abnormal thyroglobulin (Tg) levels or rising anti-Tg antibodies without detectable structural disease. This response is seen in approximately 15% to 20% of patients with differentiated thyroid cancer (DTC).
The American Thyroid Association (ATA) guidelines define BIR as suppressed Tg ≥1 ng/mL, stimulated Tg ≥10 ng/mL, or rising anti-Tg antibody levels in the absence of structural disease.
Clinical outcomes for patients with BIR are generally favorable, with 56% to 68% eventually achieving no evidence of disease (NED) status, 19% to 27% maintaining persistently abnormal Tg levels without structural disease, and 8% to 17% developing structural disease over 5-10 years.
Risk stratification for patients with BIR involves dynamic risk assessment, which considers initial risk estimates and modifies them based on response to therapy. Factors predicting progression from BIR to structural disease include high post-ablation stimulated Tg levels, presence of lymph node metastasis, and male gender. The ATA and AJCC/TNM staging systems are useful in predicting the shift from BIR to structural disease.
Management of BIR typically involves continued observation with ongoing TSH suppression, especially if Tg levels are stable or declining. Rising Tg or anti-Tg antibody levels should prompt further investigations and potentially additional therapies.
In summary, biochemical incomplete response in thyroid cancer is a dynamic condition requiring careful monitoring and individualized management based on risk stratification and response to therapy.
Negative imaging with elevated thyroglobulin (Tg) or anti-Tg antibodies:
During follow-up after initial treatment for differentiated thyroid cancer (DTC)
This response category reflects persistent biochemical evidence of disease:
Without structural correlates
The prognosis for patients with a biochemical incomplete response:
Is generally favorable but variable:
Approximately 30% of patients spontaneously achieve no evidence of disease (NED)
An additional 20% achieve NED with further therapy
20% progress to structural disease
Disease-specific mortality is rare, occurring in less than 1% of cases
Risk Factors and Predictors:
Several factors influence the likelihood of a biochemical incomplete response and its progression:
BRAFV600E mutation:
Is significantly associated with biochemical incomplete response, with studies showing a higher prevalence of this mutation in affected patients
This mutation also correlates with an increased risk of progression to structural disease
Patients with a biochemical incomplete response have a higher recurrence risk compared to those with an excellent response:
But their risk is lower than that of patients with a structural incomplete response
Management Strategies:
Management of a biochemical incomplete response:
Is guided by the trend in Tg or anti-Tg antibody levels and the absence of structural disease
Observation with TSH suppression:
For patients with stable or declining Tg levels, continued observation with ongoing TSH suppression is recommended:
The degree of TSH suppression should be individualized based on the patient’s risk profile and comorbidities
Rising Tg or anti-Tg antibody levels:
If Tg or anti-Tg antibody levels increase, further evaluation with imaging (e.g., neck ultrasound, cross-sectional imaging, or functional imaging such as RAI SPECT/CT or PET-CT) is warranted
Additional therapies, such as radioactive iodine (RAI) therapy, may be considered in select cases:
Particularly if Tg levels remain persistently elevated or if there is evidence of iodine-avid disease
Additional RAI therapy:
While not universally required, additional RAI therapy may be beneficial in patients with persistent biochemical evidence of disease:
Especially if Tg levels are significantly elevated or rising
Approximately 20% of patients achieve NED with further RAI therapy
Clinical Outcomes and Long-Term Follow-Up:
Long-term outcomes for patients with a biochemical incomplete response are generally favorable:
Most patients either achieve NED or remain biochemically stable without progression to structural disease
Approximately 60% of patients with a biochemical incomplete response have no evidence of disease over long-term follow-up
Dynamic risk stratification (DRS) allows for individualized follow-up and management adjustments based on evolving risk
This approach ensures that patients with stable disease are not overtreated, while those with evidence of progression receive timely intervention
Gaps in Evidence:
Despite the utility of DRS, there are gaps in the evidence regarding the management of biochemical incomplete response:
Limited prospective studies:
Most data on biochemical incomplete response are derived from retrospective studies
Prospective studies are needed to validate management strategies, particularly in patients treated without RAI
– Patients treated without RAI:
The interpretation of Tg levels and the utility of DRS in patients treated with lobectomy or total thyroidectomy without RAI remain less well-defined, necessitating further research
In summary:
A biochemical incomplete response in DRS is associated with a generally favorable prognosis, though a subset of patients may progress to structural disease
Management involves close monitoring, TSH suppression, and selective use of additional therapies, with long-term outcomes guided by dynamic risk stratification
Ansart F, de Ponthaud C, Buffet C, et al. One- or two-step total thyroidectomy for cancer indications: a 20-year retrospective study from a referral center. Ann Surg Oncol 2024;32:2329-2334; doi: 10.1245/s10434-024-16707-6. PMID: 39739263.
Background:
Current guidelines for the management of differentiated thyroid cancer (DTC) recommend consideration of thyroid lobectomy unless there are clear indications to remove the contralateral lobe
Lobectomy carries fewer risks, including no risk of postoperative hypoparathyroidism, no risk of bilateral recurrent laryngeal nerve (RLN) injury, and lower risk of requiring thyroid hormone supplementation postoperatively
However, up to 20% of patients who undergo lobectomy have unfavorable characteristics on final pathology
Patients with high-risk DTC, such as extrathyroidal extension, multiple positive lymph nodes, or multifocal lesions, may require completion thyroidectomy
The risks of one-stage versus two-stage total thyroidectomy have not been studied thoroughly
This study aimed to compare the postoperative morbidity of patients with thyroid cancer who underwent total thyroidectomy in one stage versus two stages
Methods:
This retrospective study conducted at a high-volume endocrine surgery center included adult patients who underwent total thyroidectomy for DTC
Patients either underwent total thyroidectomy in one stage (TT1) or in two stages—thyroid lobectomy followed by completion thyroidectomy (TT2)
The primary outcome was postoperative morbidity within 30 days after surgery, which included hematoma requiring reoperation, wound infection or swelling, temporary or permanent RLN injury resulting in vocal cord immobility, and hypocalcemia
Transient hypocalcemia was defined as a postoperative serum calcium level lower than 8 mg/dl within the first 6 months, while permanent hypocalcemia was defined as PTH <15 pg/ml or the need for oral calcium supplementation after 6 months
For patients in the TT2 group, postoperative complications were quantified as the sum of those observed after each procedure
Results:
The study cohort consisted of 5693 patients, 5009 in the TT1 group and 684 in the TT2 group
The majority of patients in both groups were female, though the rate was higher in the TT1 group than the TT2 group (79% vs. 69.3%, P<0.001)
TT1 patients were significantly older (mean [±SD], 49.9±14.7 years) than TT2 patients (45.4±4.5 years, P<0.001)
Patients with papillary thyroid cancer primarily underwent TT1 (92.1%), whereas those with follicular or oncocytic cancers underwent TT1 and TT2 equally (P<0.001)
There was no difference in lymph node dissection rates between TT1 and TT2; however, on average, there were more nodes removed (18.1±13.4 vs. 12.2±9.5, P<0.001) and more positive results (29.8% vs. 14.3%, P<0.001) in TT1 patients than TT2
Tumors in TT2 patients were significantly larger (14.4±13.8 mm vs. 28.2±18.4 mm, P<0.001) but there was no difference in tumor stage
TT2 patients had significantly lower rates of all surgical complications (11.7% vs. 22.6% for TT1), transient hypocalcemia (3.2% vs. 14.5%), and permanent hypocalcemia (1.3% vs. 3.1%) (P<0.01 for all)
There were no differences in the rate of hematoma, RLN injury, or wound infection between the two groups
After propensity-score matching, TT1 patients experienced higher rates than TT2 patients for overall surgical complications (22% vs. 11.7%), transient hypocalcemia (14.1% vs. 3.2%)(P<0.01 for both), and permanent hypocalcemia (2.9% vs. 1.3%, P = 0.024) and there were no differences in the rates of RLN injury, hematoma, or infection
Conclusions:
Patients undergoing one-stage total thyroidectomy for thyroid cancer experienced higher rates of postoperative hypocalcemia and overall complications as compared with patients undergoing a two-stage operation
However, there were no differences in the rates of RLN injury, hematoma, or infection between the two treatment groups
Two-stage total thyroidectomy for thyroid cancer may be performed safely, with similar complication rates to those for one-stage surgery
This retrospective study demonstrates the safety of thyroid lobectomy followed by completion thyroidectomy as necessitated by pathology results, supporting the trend toward less aggressive surgical management of small DTCs
These results are concordant with both a retrospective study of over 70,000 patients in a national database, which found that completion thyroidectomies are associated with lower rates of complications, and a single-center study that reported that completion thyroidectomy was less likely to result in hypocalcemia and poses no additional risk of RLN injury, hematoma, or permanent hypoparathyroidism
Thyroid lobectomy also avoids the potential need for lifelong thyroid hormone replacement, and there is no difference in overall prognosis for DTCs < 4 cm in size
With higher complication rates identified in the TT1 group in the present study, there is further evidence that initial management of DTC < 4 cm with thyroid lobectomy may be preferred despite the potential need for completion thyroidectomy
Applying these results to practice, there is significant evidence to support offering lobectomy to patients with DTC < 4 cm, with the knowledge that it is both therapeutic and diagnostic but also that this approach may necessitate a completion thyroidectomy
Although there are some instances where upfront total thyroidectomy may be desired, initial lobectomy offers a less invasive option with lower complication rates even if completion thyroidectomy is needed
Encouragingly, complication rates are low for both total and two-stage thyroidectomy, supporting either surgical approach based on patient or treatment team preference
For patients with lower-risk thyroid cancers, lobectomy is a safe initial management choice given the favorable outcomes of two-stage thyroidectomy
References:
Haugen BR, Sawka AM, Alexander EK, et al. American Thyroid Association guidelines on the management of thyroid nodules and differentiated thyroid cancer task force review and recommendation on the proposed renaming of encapsulated follicular variant papillary thyroid carcinoma without invasion to noninvasive follicular thyroid neoplasm with papillary-like nuclear features. Thyroid 2017;27:481–483; Crossref. PubMed.
Ansart F, de Ponthaud C, Buffet C, et al. One- or two-step total thyroidectomy for cancer indications: a 20-year retrospective study from a referral center. Ann Surg Oncol 2024;32:2329-2334; Crossref. PubMed.
Brauer PR, Reddy CA, Burkey BB, et al. A national comparison of postoperative outcomes in completion thyroidectomy and total thyroidectomy. Otolaryngol. Head Neck Surg 2021;164(3):566-573; Crossref. PubMed.
Dedhia PH, Stoeckl EM, McDow AD, et al. Outcomes after completion thyroidectomy versus total thyroidectomy for differentiated thyroid cancer: a single-center experience. J Surg Oncol 2020;122(4):660-664; Crossref.PubMed.
Barney BM, Hitchcock YJ, Sharma P, et al. Overall and cause-specific survival for patients undergoing lobectomy, near-total, or total thyroidectomy for differentiated thyroid cancer. Head Neck 2011;33(5):645-649; Crossref.PubMed.
Mendelsohn AH, Elashoff DA, Abemayor E, et al. Surgery for papillary thyroid carcinoma: is lobectomy enough? Arch Otolaryngol Head Neck Surg 2010;136(11):1055; Crossref. PubMed
Provide both structural and functional information and can be very useful in determining the etiology of biochemical hyperthyroidism:
In contrast, thyroidal nuclear imaging is not recommended in the evaluation of a patient with hypothyroidism
For nuclear imaging, scans using radioactive iodine isotopes are most preferred:
Because these directly reflect the active accumulation (trapping) of iodine by the thyroid follicular cell and covalent attachment (organification) of iodine to thyroglobulin
The preferred radionuclide for diagnostic nonthyroid cancer imaging:
Is 123I, because this isotope emits only gamma rays that pass through tissue without significant cellular damage:
In contrast, 131I emits both gamma rays for imaging, as well as damaging beta particles:
So it can be used for the treatment of hyperthyroidism and thyroid cancer:
To destroy iodine-avid thyroid tissue
For diagnostic imaging:
123I is administered orally:
With the measurement of iodine uptake and gamma scintigraphy images:
Obtained 4 hours and / or 24 hours later
Measured thyroidal uptake depends on the activity of NIS and overall iodine status as determined by the amount of circulating nonradioactive iodine:
When there is an excess of nonradioactive iodine:
The measured radioactive iodine uptake is reduced due to the competition between radioactive and nonradioactive iodine uptake by the thyroid follicular cells:
Sources of excess nonradioactive iodine include kelp, seaweed, seafood, iodine-rich medications and agents (amiodarone, saturated solution of potassium iodide [SSKI], Lugol’s solution, povidone iodine, tincture of iodine, iodoform gauze), and radiographic contrast media used commonly in computed tomography (CT) scans and gallbladder studies
An alternate radionuclide is technetium99m pertechnetate (99mTc):
Which is administered intravenously
Images are obtained much more rapidly than 123I:
Usually on the order of 30 to 60 minutes after the administration of the radionuclide tracer
Although 99mTc will be trapped by the thyroid follicular cells:
There is no iodine moiety for attachment to thyroglobulin, and therefore does not as accurately mimic the thyroidal uptake of iodine as radioiodine nuclides:
Thus 123I thyroid scans have 5% to 8% fewer false negative results than 99mTc scans:
However, because 99mTc scans are easier, faster, more readily available and less expensive to perform, they have largely replaced 123I scans at some institutions
Studies of direct comparison of radioiodine and 99mTc thyroid scans have been highly concordant in patients without nodules and in those with cold nodules:
One study reported that of 273 patients with thyroid nodules, only two had increased uptake with pertechnetate and no uptake with radioiodine:
However, if the results of the 99mTc scan are not in agreement with the clinical picture, an 123I scan should be performed
Although nuclear scans are useful in the differential diagnosis of biochemical hyperthyroidism:
Other radiologic modalities (e.g., ultrasonography, CT, and magnetic resonance imaging [MRI]) provide information regarding structural anatomy of the thyroid and provide no functional data
The primary role of thyroid ultrasound is in the initial evaluation of thyroid nodules:
As recommended by the American Thyroid Association and the American Association of Clinical Endocrinologists
Although thyroid ultrasound does not have a role in the initial evaluation of biochemical thyroid dysfunction:
It may demonstrate changes that are consistent but are not necessarily diagnostic of chronic lymphocytic thyroiditis, subacute granulomatous thyroiditis, and postpartum thyroiditis
Some individuals with subclinical hypothyroidism and sonographic features suggestive of chronic thyroiditis:
Are at significant risk for developing overt hypothyroidism requiring thyroid hormone replacement therapy
Before the implementation of routine screening mammography:
Most patients with DCIS presented with a:
Palpable mass
Nipple thickening
Nipple discharge
Paget disease of the nipple
Occasionally, DCIS was an incidental finding:
In an otherwise benign breast biopsy specimen
In patients with palpable lesions:
Up to 25% demonstrated foci of invasive disease
Now that screening mammography is more prevalent:
The incidence of DCIS has increased dramatically and currently comprises:
Approximately 20% of all breast cancers
Most cases of DCIS are diagnosed:
When the tumor is still clinically occult
Patients with abnormalities detected by screening mammography:
Should always undergo diagnostic imaging of the contralateral breast:
Because 0.5% to 3.0% of patients have:
Synchronous occult abnormalities or cancers in the contralateral breast
Mammographic images should be compared with previous images, if available, to establish interval changes
Mammographic features:
On a mammogram, DCIS can present as:
Microcalcifications:
80% to 90% of mammographic manifestations
A soft-tissue density
Both
Microcalcifications:
Are the most common (80% to 90%) mammographic manifestation of DCIS:
Which, in turn, accounts for 80% of all breast carcinomas:
Presenting with calcifications
Any interval change from a previous mammogram:
Is associated with malignancy in 15% to 20% of cases:
Most often indicates in situ disease
Holland et al. (1990):
Described two different classes of microcalcifications:
Linear branching-type microcalcifications:
Which are more often associated with:
High–nuclear-grade lesions
Comedo-type lesions
Fine, granular calcifications:
Which are primarily associated with:
Micropapillary or cribriform lesions:
Of lower nuclear grade and that do not show necrosis
Although the morphology of microcalcifications:
Suggests the architectural type of DCIS:
It is not always reliable
Holland et al:
Also demonstrated that the mammographic findings:
Significantly underestimated the pathologic extent of disease:
Particularly in cases of:
Micropapillary DCIS:
Lesions were more than 2 cm larger by histologic examination than by mammographic estimation:
In 44% of cases of micropapillary lesions, compared with only 12% of cases of the pure comedo subtype
However, when magnification views were used in diagnostic mammographic examination:
The extent of disease was underestimated in only 14% of cases of micropapillary tumors
Hence, magnification views increase the image resolution and are better able to delineate the shape, number, and extent of microcalcifications when compared with mammography alone:
And should be used routinely in the evaluation of suspicious mammographic findings
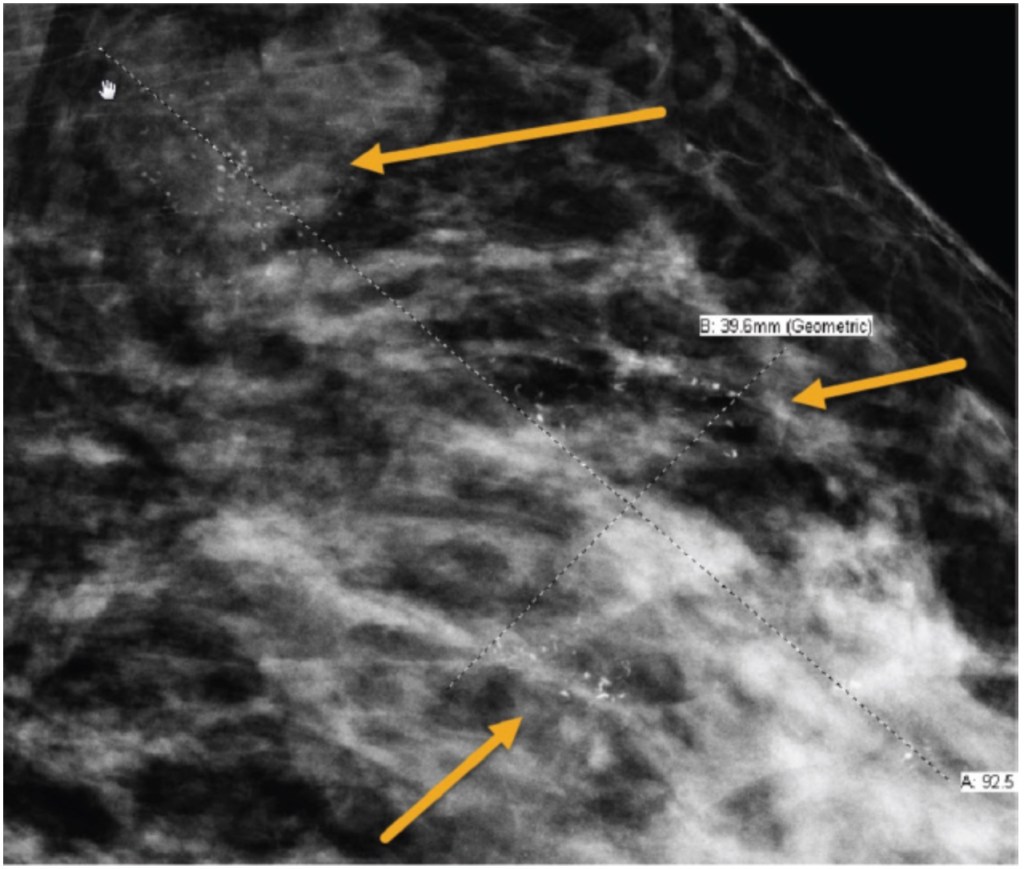
Calcifications seen on diagnostic mammography associated with ductal carcinoma in situ (DCIS). Magnification view is shown to demonstrate calcifications spanning approximately 9 cm.