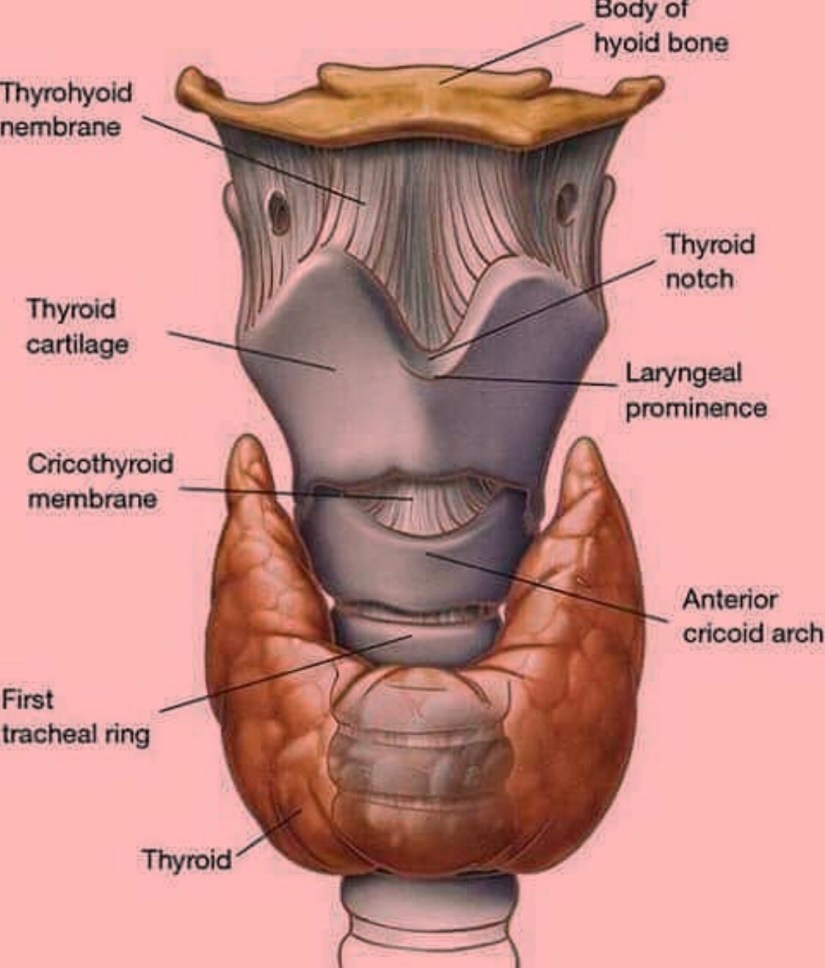
El hiperparatiroidismo primario (HPTP) se produce cuando alguna de las cuatro glándulas paratiroideas empiezan a funcionar anormalmente debido a que desarrollan un tumor benigno (adenoma) o se encuentran crecidas (hiperplasia de las cuatro) llevando a la secreción anormal y sin regulación de la hormona que producen (hormona paratiroidea). El hiperparatiroidismo primario (HPTP) es una enfermedad benigna con un potencial de causar problemas importantes a la salud de la persona:
-
El HPTP aumenta el riesgo de desarrollar enfermedades cardiovasculares como: -
-
Presión elevada (hipertensión arterial) -
Crecimiento del lado izquierdo del corazón (hipertrofia ventricular izquierda) -
Alteraciones del ritmo cardiaco (arritmias cardiacas) -
Infarto / embolia cerebral (enfermedad cerebrovascular)
-
-
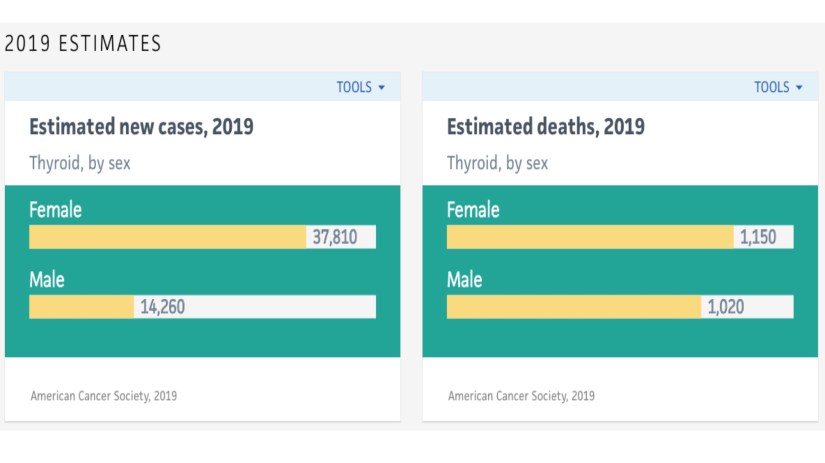
El HPTP aumenta el riesgo de desarrollar cierto tipos de cáncer comparado con la población general: -
-
Cáncer de colon, cáncer de recto, cáncer renal, cáncer de próstata, y cáncer de mama
-
Los pacientes con HPTP suelen vivir en promedio de 5.6 años menos de lo esperado comparado con la población en general. La gran mayoría de la gente conoce alguna persona que tiene hiperparatiroidismo primario (HPTP):
-
Desafortunadamente alrededor del 70% de los pacientes con hiperparatiroidismo primario no saben que tienen la enfermedad: -
-
Tienen niveles altos de calcio (arriba de 10 mg/dl), pero sus médicos no saben lo que esto significa. -
-
Muchas veces los médicos no piensan en esta enfermedad hasta que las consecuencias del hiperparatiroidismo se vuelven evidentes: -
-
Cálculos renales, osteoporosis, depresión severa, fatiga, dolores musculares, insomnio etc.
-
-
-
El hiperparatiroidismo primario es mas común en las mujeres que en los hombres:
-
75% de los casos se diagnostica en mujeres comparado a 25% en los hombres. -
La edad media en el momento del diagnostico es de 59 años de edad: -
-
Pero la enfermedad puede presentarse a cualquier edad.
-
La incidencia del hiperparatiroidismo primario:
-
Affecta una de cada 250 personas: -
34 a 120 casos por 100,000 personas años -
Esta tasa es mucho mayor en las mujeres mayores de 50: -
-
1 en cada 75 mujeres.
-
Yeh MW. J Clin Endocrinol Metab 2013 Mar;98(3):1122-9..
Almquist M. Cancer Causes Control 2007;18:595-602.
Norenstedt S. Clin Epidemiol 2011;25:103-10
👉Encuentre más información: http://www.hiperparatiroidismo.info
#Arrangoiz
#ParathyroidExpert
#ParathyroidSurgeon
#Hiperparatiroidismo
#Hipercalcemia
#CheckYourCalcium
#HeadandNeckSurgeon
#EndocrineSurgeon
https://rodrigoarrangoizmd.wordpress.com/2019/07/01/mes-de-concienca-de-paratiroides/