Studies continue to evaluate for a subset of patients with DCIS:
Who may not require adjuvant radiation therapy following breast-conserving surgery
In a prospective non-randomized trial, ECOG E5194:
Evaluated two cohorts of patients:
Group 1 had ≤ 2.5-cm low- and intermediate-grade DCIS, and
Group 2 had ≤ 1 cm high-grade DCIS
Both cohorts had margins of at least 3 mm and did not:
Receive adjuvant radiation therapy
Tamoxifen was given to:
30% of patients
Local recurrence at 5 years was:
6.1% in group 1 and 15.3% in group 2
The rate at 12 years was:
14.4% in group 1 and 24.6% in group 2
There was no plateau in the incidence of local recurrence over time
The Radiation Therapy Oncology Group (RTOG) 9804 study:
Randomized patients with < 2.5 cm low- and intermediate-grade DCIS and margins ≥ 3 mm:
To adjuvant radiation or no radiation therapy following partial mastectomy
Seven-year outcomes demonstrated:
An increase in local recurrence with the omission of radiation therapy:
6.7% vs 0.9%
Tamoxifen was given to 62% of patients
Similar outcomes were also noted in the Dana Farber prospective trial of excision alone
REFERENCES
McCormick B, Winter K, Hudis C, et al. RTOG 9804: a prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J Clin Oncol. 2015;33:709-715.
Solin LJ, Gray R, Hughes LL, et al. Surgical excision without radiation for ductal carcinoma in situ of the breast: 12-year results from the ECOG-ACRIN E5194 study. J Clin Oncol. 2015;33:3938-3944.
Wong JS, Kaelin CM, Troyan SL, et al. Prospective study of wide excision alone for ductal carcinoma in situ of the breast. J Clin Oncol. 2006;24:1031-1036.
Several guidelines have been published to guide decision making for treating select patients with partial breast irradiation off protocol:
The American Society for Radiation Oncology consensus statement (Table 1) considers patients to be “suitable” if the following characteristics are met:
Age 50 years and older
BRCA 1 / 2 wild-type
Tumor size 2 cm or less:
Multi-focality is allowed:
Provided the total size is 2 cm or less
ER-positive
Invasive ductal (or other favorable) histology
Surgical margins 2 mm or greater
Absence of LVI
Pure ductal carcinoma in situ (DCIS) meeting trial criteria
Absence of an extensive intra-ductal component
The absence of lymph node involvement
American Society for Radiation Oncology consensus statement (Table 1) considers patients to be “unsuitable” if the following characteristics are met:
Age younger than 40 years
Presence of a BRCA 1 / 2 deleterious mutation
Tumor size greater than 3 cm:
Including multiple foci
Multi-centricity
Positive surgical margins
Extensive LVI
Lymph node involvement (or not assessed).
American Society for Radiation Oncology consensus statement (Table 1) considers patients to be “cautionary” if the characteristics fall between suitable and unsuitable
The recent American Brachytherapy Society (Table 2):
Defined acceptable criteria for partial breast irradiation as:
Age 50 years and older
Size ≤ 3 cm
All invasive subtypes
Pure DCIS
ER-positive
ER-negative
Negative surgical margins (“on ink”)
Negative lymph nodes
Absence of LVI
The Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO) consensus statement (Table 3) also classifies patients as “low risk” and good candidates for partial breast irradiation with the following criteria:
Age 50 years and older
ER-negative (or positive) disease
Tumors 3 cm or less
The American Society of Breast Surgeons current guidelines (Table 4) include:
Polgár C, Van Limbergen E, Potter R, et al; GEC-ESTRO breast cancer working group. Patient selection for accelerated partial-breast irradiation (APBI) after breast-conserving surgery: recommendations of the Groupe Européen de Curiethérapie-European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) Breast Cancer Working Group based on clinical evidence (2009). Radiother Oncol. 2010;94:264-273.
Shah C, Vicini F, Wazer DE, Arthur D, Patel RR. The American Brachytherapy Society consensus statement for accelerated partial breast irradiation. Brachytherapy. 2013;12:267-277.
Smith BD, Arthur DW, Buchholz TA, et al. Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO). Int J Radiat Oncol Biol Phys. 2009;74:987-1001.
Is a well-recognized indication for palliative irradiation
Whole-brain irradiation:
May also be offered as the primary treatment modality for brain metastases or in combination with surgical resection or stereotactic radio-surgery
Studies have demonstrated an improvement in intracranial control:
With the addition of radiation following surgery
For patients with choroidal involvement:
Treatment of the globe with or without concomitant whole-brain irradiation:
May be offered for vision preservation
Locoregional radiation therapy:
In the setting of widely metastatic disease:
Is not otherwise indicated
REFERENCES
Chow E, Harris K, Fan G, Tsao M, Sze WM. Palliative radiotherapy for bone metastases: a systematic review. J Clin Oncol. 2007;25:1423-1436.
Kocher M, Soffietti R, Abacioglu U, et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952-26001 study. J Clin Oncol. 2011;29:134-141.
Le Scodan R, Stevens D, Brain E, et al. Breast cancer with synchronous metastases: survival impact of exclusive locoregional radiotherapy. J Clin Oncol. 2009;27:1375-1381.
Ly BH, Nguyen NP, Vinh-Hung V, Rapiti E, Vlastos G. Loco-regional treatment in metastatic breast cancer patients: is there a survival benefit? Breast Cancer Res Treat. 2010;119:537-545.
Patchell RA, Tibbs PA, Regine WF, et al. Postoperative radiotherapy in the treatment of single metastases to the brain: a randomized trial. JAMA. 1998;280:1485-1489.
The European Organisation for Research and Treatment of Cancer (EORTC) boost trial:
Enrolled patients with:
Stage I and II breast cancer
Treated with lumpectomy and axillary dissection
Patients with surgical margins free from invasive disease were randomized to receive:
Whole-breast irradiation:
With or without a subsequent boost targeting the tumor bed
The 20-year overall survival and breast cancer specific mortality:
Were similar between the two groups
The overall rate of ipsilateral breast tumor recurrence (IBTR) was lower in the boost group:
12% vs 16.4% at 20 years
The absolute risk reduction was greatest in younger patients:
Nearly a 12% difference for patients younger than age 40 years compared to a 3% difference in patients older than age 60 years
The local control conferred by a boost:
Translated into fewer salvage surgeries
Adding a boost:
Did not increase cardiac mortality, contralateral breast tumors, or second primary tumors
But did increase fibrosis and impacted cosmetic results
Similar results were noted:
In the randomized Lyon boost trial
REFERENCES
Bartelink H, Maingon P, Poortmans P, et al; European Organisation for Research and Treatment of Cancer Radiation Oncology and Breast Cancer Groups. Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. Lancet Oncol. 2015;16:47-56.
Romestaing P, Lehingue Y, Carrie C, et al. Role of a 10-Gy boost in the conservative treatment of early breast cancer: results of a randomized clinical trial in Lyon, France. J Clin Oncol. 1997;15:963-968.
Whole-breast irradiation (WBI) can be administered following delivery:
Uterine shielding can reduce the dose but in non-life threatening situations:
Radiation should be held until after delivery
Risks of radiation while pregnant can include:
Toxicity to the fetus
Increased risk of second malignancy in the child
Although hypofractionated WBI has been studied and found to be comparable to standard WBI:
Few patients enrolled were younger than age 50 years
Current American Society for Radiation Oncology guidelines:
Do not recommend:
Hypofractionated WBI for patients younger than age 50 years
Accelerated partial breast irradiation:
Has been shown to provide equivalent rates of local recurrence compared to standard WBI:
However, due to a paucity of young patients enrolled in such trials:
It is not currently recommended for patients younger age 50 years
REFERENCES
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233-1241.
Haviland JS, Owen JR, Dewar JA, et al; START Trialists’ Group. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early stage breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol. 2013;14:1086-1094.
Luis SA, Christie DR, Kaminski A, Kenny L, Peres MH. Pregnancy and radiotherapy: management options for minimizing risk, case series, and comprehensive literature review. J Med Imaging Radiat Oncol. 2009;53:559-568.
Smith BD, Arthur DW, Buchholz TA, et al. Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO). Int J Radiat Oncol Biol Phys. 2009;74:987-1001.
Smith BD, Bentzen SM, Correa CR, et al. Fractionation for whole breast irradiation: an American Society for Radiation Oncology (ASTRO) evidence-based guideline. Int J Radiat Oncol Biol Phys. 2011;81:59-68.
Strnad V, Ott OJ, Hildebrandt G, et al; Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO). 5-year results of accelerated partial breast irradiation using sole interstitial multicatheter brachytherapy versus whole-breast irradiation with boost after breast-conserving surgery for low-risk invasive and in-situ carcinoma of the female breast: a randomised, phase 3, non-inferiority trial. Lancet. 2016;387:229-238.
Whelan TJ, Pignol JP, Levine MN, et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med. 2010;362:513-520.
Leads to indistinct borders and a high incidence of multicentricity
Advanced lesions:
Can show hemorrhage or ulceration
Cervical lymphadenopathy:
Is found in approximately 10% of patients at the time of presentation
Natural history and prognosis:
The outlook for these tumors is poor:
With five-year survival:
Generally less than 40%:
As an example:
In a series of 133 angiosarcomas of the scalp and neck reported to the SEER database between 1973 and 2007:
Five and 10-year survival rates were:
34% and 14%, respectively:
Local recurrence is a major problem
But distant metastases are also frequent
The most important prognostic factor for survival in patients with head and neck angiosarcoma:
Is size and the ability to completely resect the tumor:
Patients with tumors less than 5 cm in diameter:
Have better overall survival and a lower risk of regional recurrence:
In addition:
Cellular epithelioid morphology:
Is emerging as a potentially adverse prognostic factor:
As is age 70 and older
Treatment:
There is limited evidence, other than case series:
Upon which to base treatment recommendations for angiosarcoma of the head and neck
Complete surgical resection with wide margins:
Is preferred for local and locoregional disease:
Although the risk of lymph node spread is higher with angiosarcomas than with other head and neck sarcomas:
The overall risk remains lower than what is generally considered an indication for elective lymph node dissection:
As a result, most surgeons reserve neck treatment for gross nodal disease only
Reconstruction is performed immediately following resection; even sizable deficits can be reconstructed using current techniques:
Radial forearm and rectus abdominis microvascular free flaps can cover large surface defects with minimal donor site morbidity
Smaller defects can be reconstructed using skin grafts, or local or regional flaps
Some surgeons perform small mapping biopsies along the proposed margins preoperatively:
So that disease with subclinical microscopic spread can be identified and appropriate ablative and reconstructive planning undertaken prior to definitive resection
Due to the propensity for insidious local infiltration:
Resection should be combined in nearly all cases by preoperative or postoperative RT:
Although randomized trials are not available, the benefits of RT are supported by several small reports
As examples:
In one series of 28 patients with angiosarcoma of the head and neck treated at the University of California, Los Angeles (UCLA):
Only 1 of 12 patients treated with surgery alone remained disease free compared with four of six who received postoperative RT, with or without chemotherapy
In a second report of 70 patients with non- metastatic angiosarcoma of the face and scalp:
Combined therapy with surgery plus RT (versus surgery alone or RT alone) was associated with:
Improved overall survival (68% versus 32%)
Disease-specific survival (76% versus 33%)
As well as better local control
The role of adjuvant chemotherapy, either alone or concurrent with RT, is unclear:
In the above cited series of 70 patients with non-metastatic angiosarcoma, outcomes were not significantly better in those who received any chemotherapy in addition to local therapy:
Five-year overall survival 45% versus 39%, p = 0.54)
However, interest is increasing in neoadjuvant chemotherapy and / or RT as a component of combined modality therapy, which may allow some patients to undergo potentially less mutilating surgery
For patients with unresectable tumors or those who refuse surgery, definitive RT or chemoradiation is an option
Systemic treatment for metastatic angiosarcoma generally follows the same principles as for other anthracycline-sensitive adult-type advanced soft tissue sarcomas:
However, in contrast to other soft-tissue sarcomas:
Angiosarcomas appear to be particularly responsive to taxanes
In addition, promising responses, occasionally dramatic, have been demonstrated in very limited number of angiosarcoma patients with various biologic molecules, including:
Bevacizumab, sunitinib, and sorafenib, either as single agents or in combination with chemotherapy
References:
Albores-Saavedra J, Schwartz AM, Henson DE, et al. Cutaneous angiosarcoma. Analysis of 434 cases from the Surveillance, Epidemiology, and End Results Program, 1973-2007. Ann Diagn Pathol 2011; 15:93.
Lydiatt WM, Shaha AR, Shah JP. Angiosarcoma of the head and neck. Am J Surg 1994; 168:451.
Mark RJ, Tran LM, Sercarz J, et al. Angiosarcoma of the head and neck. The UCLA experience 1955 through 1990. Arch Otolaryngol Head Neck Surg 1993; 119:973.
Panje WR, Moran WJ, Bostwick DG, Kitt VV. Angiosarcoma of the head and neck: review of 11 cases. Laryngoscope 1986; 96:1381.
Holden CA, Spittle MF, Jones EW. Angiosarcoma of the face and scalp, prognosis and treatment. Cancer 1987; 59:1046.
Fury MG, Antonescu CR, Van Zee KJ, et al. A 14-year retrospective review of angiosarcoma: clinical characteristics, prognostic factors, and treatment outcomes with surgery and chemotherapy. Cancer J 2005; 11:241.
Maddox JC, Evans HL. Angiosarcoma of skin and soft tissue: a study of forty-four cases. Cancer 1981; 48:1907.
Morrison WH, Byers RM, Garden AS, et al. Cutaneous angiosarcoma of the head and neck. A therapeutic dilemma. Cancer 1995; 76:319.
Willers H, Hug EB, Spiro IJ, et al. Adult soft tissue sarcomas of the head and neck treated by radiation and surgery or radiation alone: patterns of failure and prognostic factors. Int J Radiat Oncol Biol Phys 1995; 33:585.
Lahat G, Dhuka AR, Hallevi H, et al. Angiosarcoma: clinical and molecular insights. Ann Surg 2010; 251:1098.
Köhler HF, Neves RI, Brechtbühl ER, et al. Cutaneous angiosarcoma of the head and neck: report of 23 cases from a single institution. Otolaryngol Head Neck Surg 2008; 139:519.
Patel SH, Hayden RE, Hinni ML, et al. Angiosarcoma of the scalp and face: the Mayo Clinic experience. JAMA Otolaryngol Head Neck Surg 2015; 141:335.
Aust MR, Olsen KD, Lewis JE, et al. Angiosarcomas of the head and neck: clinical and pathologic characteristics. Ann Otol Rhinol Laryngol 1997; 106:943.
Guadagnolo BA, Zagars GK, Araujo D, et al. Outcomes after definitive treatment for cutaneous angiosarcoma of the face and scalp. Head Neck 2011; 33:661.
Amato L, Moretti S, Palleschi GM, et al. A case of angiosarcoma of the face successfully treated with combined chemotherapy and radiotherapy. Br J Dermatol 2000; 142:822.
Lankester KJ, Brown RS, Spittle MF. Complete resolution of angiosarcoma of the scalp with liposomal daunorubicin and radiotherapy. Clin Oncol (R Coll Radiol) 1999; 11:208.
Young RJ, Brown NJ, Reed MW, et al. Angiosarcoma. Lancet Oncol 2010; 11:983.
DeMartelaere SL, Roberts D, Burgess MA, et al. Neoadjuvant chemotherapy-specific and overall treatment outcomes in patients with cutaneous angiosarcoma of the face with periorbital involvement. Head Neck 2008; 30:639.
Estimates which patients with DCIS can be managed by:
Excision alone vs
Excision plus radiation vs
Those who require mastectomy
There are three groups of patients in the index:
Group 1 patients have:
Non-high nuclear grade DCIS without necrosis
Group 2 patients have:
Non-high nuclear grade DCIS with necrosis
Group 3 patients have:
High nuclear grade DCIS with or without necrosis
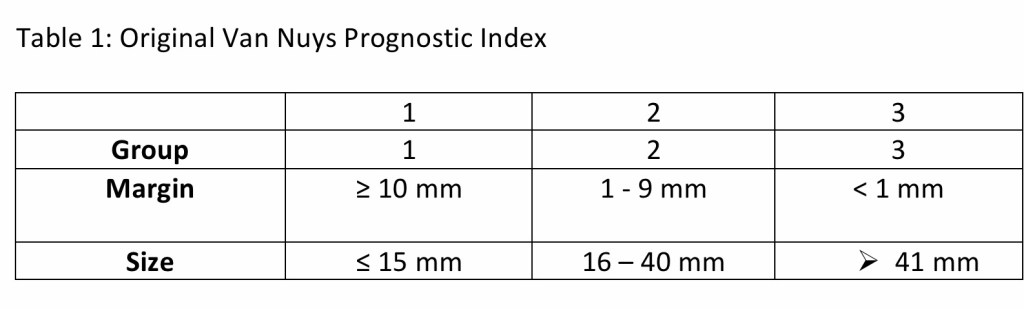
The original Van Nuys Prognostic Index:
Introduced in 1996, had two additional variables:
They were:
Size of DCIS and margin width
A score from 3 to 9 was derived by:
Assigning 1, 2, or 3 points to each of the 3 variables as shown below in the Table 1:
Patients who scored 3 or 4:
Derived little benefit from radiation
Patients who scored 5, 6, or 7:
Derived substantial benefit from radiation
Patients who scored 8 or 9:
Had a high risk of relapse despite radiation and are best managed:
By mastectomy
In 2003:
The name became the University of Southern California / Van Nuys Prognostic Index
A 4th variable was added to the score:
Patients who were younger than age 40 years:
Received a score of 3
Patients from ages 40 to 60 years:
Received score of 2
Patients older than age 60 years:
Received a score of 1
The range of possible scores then became 4 to 12:
Patients with a score of 4, 5, or 6:
Did not receive a statistically significant benefit from radiation
Patients with scores of 7, 8, and 9:
Who were treated with radiation:
Received a significant reduction in local disease-free recurrence:
Of 12% to 15%
Patients with scores of 10, 11, and 12:
Had a local recurrence rate of almost:
50% at five-years despite radiation
By 2010 the number of patients was large enough to allow analysis by individual scores as opposed to groups of scores, and the following was reported:
To achieve a local recurrence rate of less than20% at 12 years:
These data support excision alone:
For all patients scoring 4, 5, or 6 and patients who score 7 but have margin widths ≥ 3 mm
Excision plus radiation therapy achieves the less than 20% local recurrence requirement at 12 years for patients:
Who score 7 and have margins < 3 mm, patients who score 8 and have margins ≥ 3 mm, and for patients who score 9 and have margins ≥ 5 mm
Mastectomy is suggested for patients:
Who score 8 and have margins < 3 mm, who score 9 and have margins < 5 mm, and for all patients who score 10, 11, or 12 to keep the local recurrence rate less than 20% at 12 years
REFERENCES
Silverstein MJ. The University of Southern California/Van Nuys Prognostic Index for ductal carcinoma in situ of the breast. Am J Surg. 2003;186:337-343.
Silverstein MJ, Lagios MD. Choosing treatment for patients with ductal carcinoma in situ: fine tuning the University of Southern California/Van Nuys Prognostic Index. J Natl Cancer Inst Monogr. 2010;2010:193-196.
Silverstein MJ, Lagios MD. Treatment selection for patients with ductal carcinoma in situ (DCIS) of the breast using the University of Southern California/Van Nuys (USC/VNPI) Prognostic Index. Breast J. 2015;21:127-132.
Silverstein MJ, Lagios MD, Craig PH, et al. A prognostic index for ductal carcinoma in situ of the breast. Cancer. 1996;77:2267-2274.
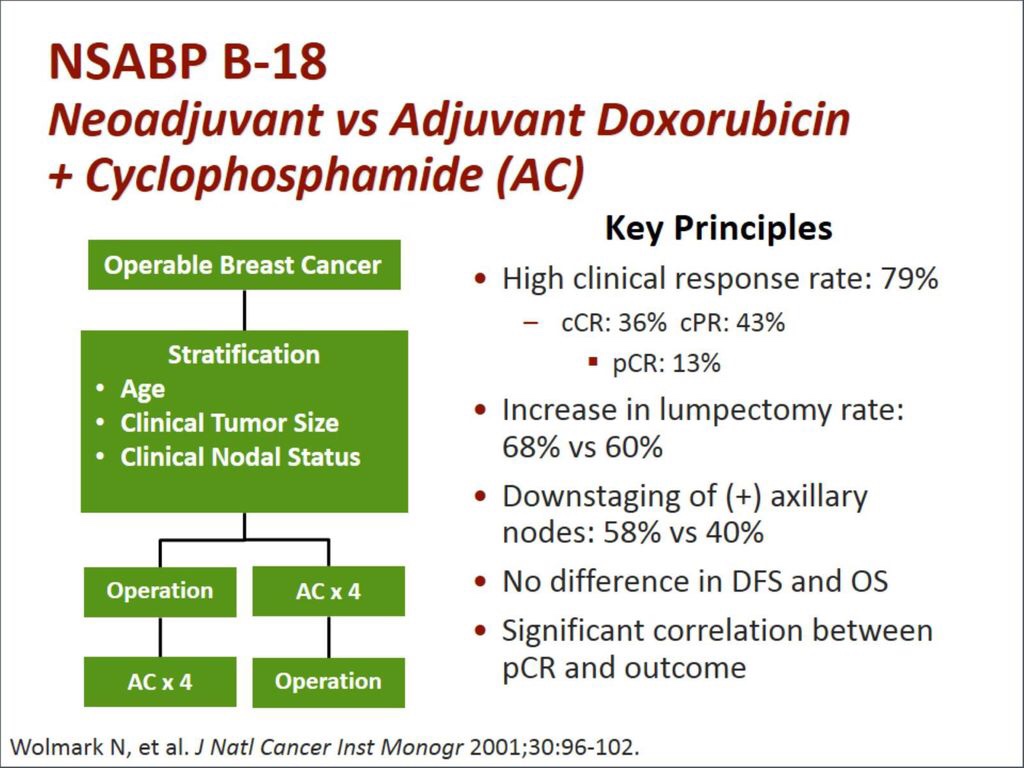
The National Surgical Adjuvant Bowel and Breast Project B-18:
Was designed to determine whether preoperative chemotherapy:
Would result in improved survival:
Compared to postoperative chemotherapy
Secondary aims included:
Evaluation of pCR rates
Comparison of breast conservation rates and ipsilateral recurrence rates between the two groups
Between 1988 and 1993:
1523 patients with:
Clinical T1 to T3, N0 to N1 operable breast cancer were enrolled in the trial
763 were randomized to preoperative therapy while
760 were randomized to postoperative therapy
At 16-years of follow-up:
There was no difference in:
Disease-free survival:
HR = 0.93, 95% CI, 0.81 to 1.06
p = 0.27 or
Overall survival:
HR = 0.99, 95% CI, 0.85 to 1.16
p = 0.90
Between the postoperative and preoperative chemotherapy groups
In the preoperative group:
A pCR was documented in:
13% of patients
Preoperative chemotherapy patients had a:
Significantly increased incidence of having:
Pathologically negative nodes compared to postoperative chemotherapy patients:
58% vs. 42%, respectively
p<0.0001
The rate of breast conservation was higher:
Among women who received neoadjuvant chemotherapy compared to women who received postoperative chemotherapy:
68% versus 60%, respectively
p = 0.001
The significant downstaging of tumors greater than 5 cm in the preoperative chemotherapy arm:
Primarily drove this breast conservation trend
There was a trend toward a higher rate of:
Ipsilateral breast tumor recurrence with preoperative vs postoperative chemotherapy:
13% of 506 patients vs 10% of 450 patients, respectively:
Although this difference was not statistically significant (p = 0.21)
Retrospective series later found:
No difference in surgical complications:
Between women who received preoperative or postoperative chemotherapy
REFERENCES
Fisher B, Bryant J, Wolmark N, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol. 1998;16(8):2672-2685.
Boughey JC, Peitinger F, Meric-Bernstam F, et al. Impact of preoperative versus postoperative chemotherapy on the extent and number of surgical procedures in patients treated in randomized clinical trials for breast cancer. Ann Surg. 2006;244(3):464–470.
Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol. 2008;26(5):778-785.
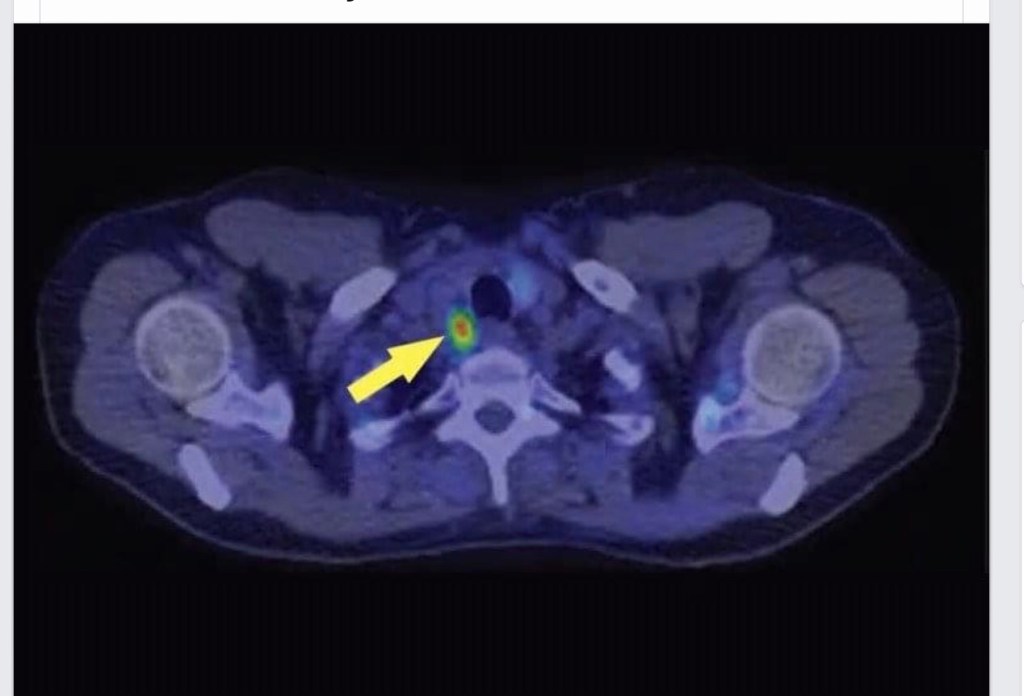
👉In patients with failure to localize on traditional imaging studies, PET choline may be an option and is offered at select centers around the country.