- The USC / VNPI:
- Estimates which patients with DCIS can be managed by:
- Excision alone vs
- Excision plus radiation vs
- Those who require mastectomy
- There are three groups of patients in the index:
- Group 1 patients have:
- Non-high nuclear grade DCIS without necrosis
- Group 2 patients have:
- Non-high nuclear grade DCIS with necrosis
- Group 3 patients have:
- High nuclear grade DCIS with or without necrosis
- Group 1 patients have:
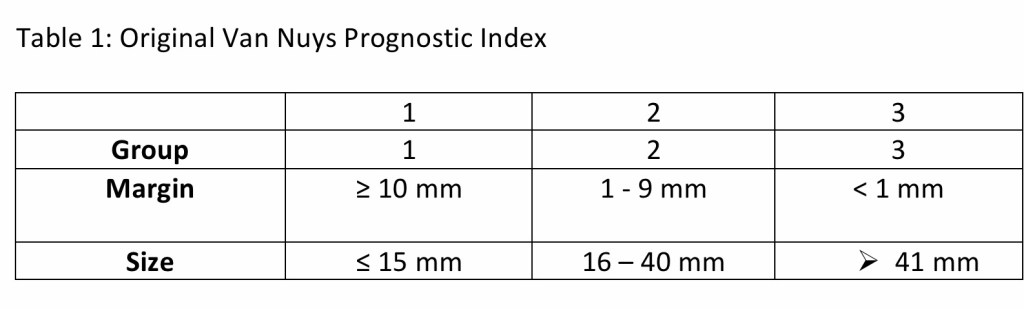
- The original Van Nuys Prognostic Index:
- Introduced in 1996, had two additional variables:
- They were:
- Size of DCIS and margin width
- They were:
- A score from 3 to 9 was derived by:
- Assigning 1, 2, or 3 points to each of the 3 variables as shown below in the Table 1:
- Introduced in 1996, had two additional variables:
- Patients who scored 3 or 4:
- Derived little benefit from radiation
- Patients who scored 5, 6, or 7:
- Derived substantial benefit from radiation
- Patients who scored 8 or 9:
- Had a high risk of relapse despite radiation and are best managed:
- By mastectomy
- Had a high risk of relapse despite radiation and are best managed:
- In 2003:
- The name became the University of Southern California / Van Nuys Prognostic Index
- A 4th variable was added to the score:
- Patients who were younger than age 40 years:
- Received a score of 3
- Patients from ages 40 to 60 years:
- Received score of 2
- Patients older than age 60 years:
- Received a score of 1
- Patients who were younger than age 40 years:
- The range of possible scores then became 4 to 12:
- Patients with a score of 4, 5, or 6:
- Did not receive a statistically significant benefit from radiation
- Patients with scores of 7, 8, and 9:
- Who were treated with radiation:
- Received a significant reduction in local disease-free recurrence:
- Of 12% to 15%
- Received a significant reduction in local disease-free recurrence:
- Who were treated with radiation:
- Patients with scores of 10, 11, and 12:
- Had a local recurrence rate of almost:
- 50% at five-years despite radiation
- Had a local recurrence rate of almost:
- Patients with a score of 4, 5, or 6:
- By 2010 the number of patients was large enough to allow analysis by individual scores as opposed to groups of scores, and the following was reported:
- To achieve a local recurrence rate of less than 20% at 12 years:
- These data support excision alone:
- For all patients scoring 4, 5, or 6 and patients who score 7 but have margin widths ≥ 3 mm
- Excision plus radiation therapy achieves the less than 20% local recurrence requirement at 12 years for patients:
- Who score 7 and have margins < 3 mm, patients who score 8 and have margins ≥ 3 mm, and for patients who score 9 and have margins ≥ 5 mm
- Mastectomy is suggested for patients:
- Who score 8 and have margins < 3 mm, who score 9 and have margins < 5 mm, and for all patients who score 10, 11, or 12 to keep the local recurrence rate less than 20% at 12 years
- These data support excision alone:
- To achieve a local recurrence rate of less than 20% at 12 years:
- REFERENCES
- Silverstein MJ. The University of Southern California/Van Nuys Prognostic Index for ductal carcinoma in situ of the breast. Am J Surg. 2003;186:337-343.
- Silverstein MJ, Lagios MD. Choosing treatment for patients with ductal carcinoma in situ: fine tuning the University of Southern California/Van Nuys Prognostic Index. J Natl Cancer Inst Monogr. 2010;2010:193-196.
- Silverstein MJ, Lagios MD. Treatment selection for patients with ductal carcinoma in situ (DCIS) of the breast using the University of Southern California/Van Nuys (USC/VNPI) Prognostic Index. Breast J. 2015;21:127-132.
- Silverstein MJ, Lagios MD, Craig PH, et al. A prognostic index for ductal carcinoma in situ of the breast. Cancer. 1996;77:2267-2274.
#Arrangoiz #BreastSurgeon #CancerSurgeon #BreastCancer #SurgicalOncologist
