Per American Society of Clinical Oncology / College of American Pathologists (ASCO / CAP) guidelines:
Tumors with an immunohistochemical result of 2+ (equivocal):
HER2 / CEP 17 ratio of > 2.0 and copy number of > 4.0:
Are considered positive
References:
Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu PB, Bartlett JMS, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline focused update. J Clin Oncol. 2018;142(11):1364-1382.
Lin L, Sirohi D, Coleman JF, Gulbahce HE. American Society of Clinical Oncology/College of American Pathologists 2018 focused update of breast cancer HER2 FISH testing guidelines. results from a National Reference Laboratory. Am J Clin Pathol. 2019;152(4):479-485.
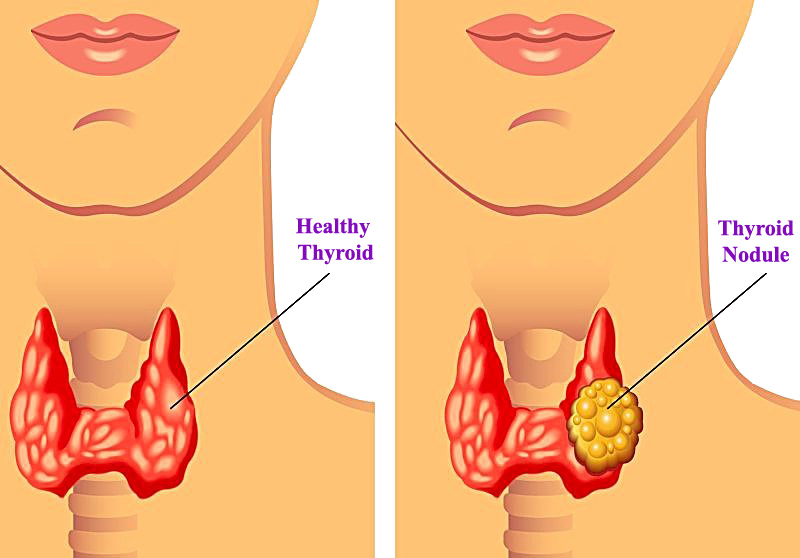
If you’re having thyroid surgery, it’s important to know how to best prepare for your procedure and what to expect while you recover. This includes any tests you’ll need before surgery, as well as what to avoid after surgery to help ensure its success.
How should I prepare for thyroid surgery?
After your thyroidectomy or thyroid lobectomy is scheduled, you’ll have a pre-operative evaluation with members of your thyroid surgery care team. That evaluation may include blood tests, an electrocardiogram (EKG), X-rays or other imaging studies.
We’ll give you specific instructions on when to stop eating, drinking and taking medications prior to surgery. It’s very important that you follow these guidelines for your own safety, and you’ll need to have an empty stomach before any surgical procedure that requires anesthesia. If you don’t follow the instructions, your thyroid surgery might be cancelled. Please contact us with any specific questions.
What is recovery like after thyroid surgery?
After your thyroidectomy or thyroid lobectomy, you may have a temporary sore throat, neck pain, difficulty swallowing or a weak voice.
Your diet will be restricted for the evening of your surgery, but in most cases, it can return to normal the next day.
Before you leave the hospital, we’ll schedule a follow-up appointment, give instructions for your at-home recovery and go over any prescribed medications.
Most people are ready to return home within one day of surgery, but take off about two weeks from work to recover. You’ll need to refrain from heavy lifting or other tasks that can strain your neck for up to three weeks after your surgery. Soaking or scrubbing the site of your incision is also discouraged for at least one week to allow it time to properly heal. Showering is generally allowed after about one day.
Pain at the site of your incision will improve after a few days but may continue for a week or so. If you notice sudden swelling in your neck, which could signify an infection, contact our office.
Due to disturbance of the parathyroid glands, which regulate calcium balance, your calcium level may drop after surgery. If it drops, you may notice numbness and tingling of your fingers or around your mouth. We’ll monitor your calcium levels through blood tests, and give you instructions about taking calcium replacements if needed.
What are the side effects of thyroid surgery?
After a total thyroidectomy, you will take lifelong thyroid hormone replacements. Because your entire thyroid gland is removed, it will no longer supply you with the hormone you need to control your body’s metabolic processes. You might also have to take supplements after thyroidectomy to balance your calcium levels.
After a thyroid lobectomy, you’ll need to have your thyroid hormone levels checked and will be prescribed a thyroid hormone replacement, if needed.
In the weeks after your thyroid surgery, you may have neck pain, soreness of your vocal chords or a weak voice. These symptoms are usually temporary.
Will I need to follow a special diet after thyroid surgery?
For most people, a special diet after a thyroidectomy or thyroid lobectomy isn’t necessary. You’ll likely be able to eat and drink normally the morning after your surgery, but you may prefer softer foods at first. We’ll let you know if and for how long you need to restrict your eating and drinking.
Decrease in ejection fraction in up to 20% of patients:
Although this is often reversible
Trastuzumab:
Can less commonly cause pneumonitis
Pertuzumab:
Can cause rash and diarrhea
References:
Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, Liu MC, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13(1):25-32.
Schneeweiss A, Chia S, Hickish T, Harvey V, Eniu A, Hegg R, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol. 2013;24(9):2278-2284.
What is the preferred adjuvant regimen for an invasive ductal carcinoma, ER positive, PR positive, HER2 positive by immunohistochemistry for a 0.9 cm grade tumor with 0/2 sentinel lymph nodes involved with tumor?
The APT trial:
Showed a 3-year survival free rate from invasive disease of 98.7% for node negative tumors up to 3 cm in size:
With use of weekly paclitaxel / trastuzumab
References:
Tolaney SM, Barry WT, Dang CT, Yardley DA, Moy B, Marcom PK, et al. Adjuvant paclitaxel and trastuzumab for node-negative, HER2-positive breast cancer. New Engl J Med. 2015;372(2):134-141.
Tolaney SM, Guo H, Pernas S, Barry WT, Dillon DA, Ritterhouse L. Seven-year follow-up analysis of adjuvant paclitaxel and trastuzumab trial for node-negative, human epidermal growth factor receptor 2-positive breast cancer.J Clin Oncol. 2019;37(22):1868-1875.
Neutropenia is found in up to 79.5% of patients on palbociclib:
Neutropenia and the risk for infections must be discussed with patients prior to initiation of treatment
Other common adverse effects of this drug include:
Fatigue (37.4%)
Nausea (35.1%)
Alopecia (32.9%)
References:
Finn RS, Martin M, Rugo HS, Jones S, Im SA, Gelmon K, et al. Palbociclib and Letrozole in advanced breast cancer. New Engl J Med. 2016;375(20):1925-1936.
Finn RS, Crown JP2, Lang I3, Boer K4, Bondarenko IM5, Kulyk SO, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol. 2015;16(1):25-35.
The use of an aromatase inhibitor (letrozole) with an inhibitor of the cyclin dependent kinases 4 and 6 (ribociclib):
Was compared with aromatase inhibitor alone in postmenopausal women with hormone receptor positive, HER2-negative metastatic breast cancer:
In the MONALEESA-2 study:
Results showed an improvement in:
Progression-free survival (PFS):
From 42.2% to 63%
Overall response rate:
From 37.1% to 52.7%
With the addition of ribociclib to letrozole alone
This regimen was also investigated in pre menopausal women with advanced, hormone receptor-positive breast cancer:
Improved PFS compared with placebo plus endocrine therapy
References:
Hortobagi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, Paluch-Shimon S, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375(18)1738-1748.
Tripathy D, Im SA2, Colleoni M3, Franke F4, Bardia A5, Harbeck Nm et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised phase 3 trial. Lancet Oncol. 2018;19(7):904-915.
Chemotherapy for a Young Patient with Triple Negative Breast Cancer
The best choice for chemotherapy for a young patient with a node-positive triple negative breast cancer:
Would be dose-dense doxorubicin and cyclophosphamide, followed by paclitaxel, each given for 4 cycles 2 weeks apart with growth factor support:
This regimen is supported by results of the:
CALGB 9741 study
For triple negative breast cancer and node positive disease:
The use of an anthracycline-containing regimen is favored compared to a non-anthracycline containing regimen
References:
Citron ML, Berry DA, Cirrincione C, Hudis C, Winer EP, Gradishar WJ, et al. Randomized trial of dose-dense versus conventionally scheduled and sequential versus concurrent combination chemotherapy as postoperative adjuvant treatment of node-positive primary breast cancer: first report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J Clin Oncol. 2003;21(8):1431-1439.
Blum JL, Flynn PJ, Yothers G, Asmar L, Geyer CE Jr, Jacobs SA et al. Anthracyclines in early breast cancer: The ABC Trials-USOR 06-090, NSABP B-46-I/USOR 07132, and NSABP B-49 (NRG Oncology). J Clin Oncol. 2017;35(23):2647-2655.
Suppression of Ovarian Function Trial (SOFT) Trial
In the Suppression of Ovarian Function Trial (SOFT) trial:
Ovarian function suppression given for five yearsreduced disease-free survival (DFS) eventswhen added to 5 years of adjuvant tamoxifen:
78.9% to 83.2% DFS at 8 years, hazard ratio (HR) of 0.76, P = .009
One-third of women entered in the SOFT trial were randomized to receive the aromatase inhibitor exemestane plus ovarian function suppression:
They had an even better disease-free survival
References:
Francis PA, Pagani O, Fleming GF, Walley BA, Colleoni M, Lang I, et al. Tailoring adjuvant endocrine therapy for premenopausal breast cancer. N Eng J Med. 2018;379(2):122-137.
Francis PA, Regan MM, Fleming GF, Lang I, Ciruelos E, Bellet M, et al. Adjuvant ovarian suppression in premenopausal breast cancer. N Engl J Med. 2015;372(5):436-446.
With HER2 negative breast cancer and residual disease after undergoing neoadjuvant chemotherapy to:
Standard postsurgical treatment and capecitabine or placebo
The primary end point was:
Disease-free survival (DFS)
Secondary end points included:
Overall survival (OS)
DFS was longer in the capecitabine group than in the control group:
74.1% vs. 67.6% of the patients were alive and free from recurrence or second cancer at 5 years
Among patients with triple-negative disease:
DFS was 69.8% in the capecitabine group versus 56.1% in the control group
The OS rate was 78.8% versus 70.3%
Residual disease after completion of neoadjuvant chemotherapy:
Is associated with worse outcomes
References:
Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Eng J Med. 2017;376(22):2147-2159.
Symmans WF, Wei C, Gould R, Yu X, Zhang Y, Liu M, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35(10):1049-1060.