Breast Cancer Screening in Women Over 74 Years of Age
Women over age 74:
Should be educated on the possible harms of screening mammogram:
Such as:
Overdiagnosis and false positives vs. the potential benefits
They should be offered the choice to stop or continue mammogram screening in the context of:
Their life expectancy
Comorbidities
Personal beliefs
Controversy exists and data are limited for using screening mammogram in women over age 74:
Healthy women in this age group of women are likely to have a lifespan of 15 years or more
Using Medicare claims and Surveillance, Epidemiology, and End Results (SEER) program data:
Patients age between 69 to 84 who elected for annual mammograms in the four years prior to breast cancer diagnosis:
Had lower 5- and 10-year death rates compared to those who elect for irregular or no mammograms during that interval
“Framing cancer screening conversations in terms of increasing harms in relation to decreasing benefits has been found to be most acceptable to older patients and may maintain or promote trust more than citing national guideline recommendations to stop screening based on age cutoffs for women with less than a 5 to 10 year life expectancy, recommendations to stop screening mammography should be framed around how a woman’s health problems increase the harms of screening (e.g., overdiagnosis) and shift the focus to interventions likely to be beneficial over a shorter time frame (e.g., falls prevention, depression screening).”
No screening breast imaging:
Is required for asymptomatic patients with a normal breast exam who have a life expectancy less than 5 years
Conversations regarding cessation of mammogram should be focused on risk of harm such as false positives and the significance of this in relation to the patient’s medical condition
Interestingly, the number of false positives actually decreases with age:
However, the number of lives saved is 2 / 1000, compared to 39% of women harmed by overdiagnosis or false positives
References
Walter LC, Schonberg MA. Screening mammography in older women: a review. JAMA. 2014;311(13): 1336-1347.
Sanderson M, Levine RS, Fadden MK, Kilbourne B, Pisu M, Cain V, et al. Mammography screening among the elderly: a research challenge. Am J Med. 2015;128(12):1362.e7-1362.e14
Sharpe RE Jr, Levin DC, Parker L, Rao VM. The Effect of the Controversial US Preventive Services Task Force Recommendations on the Use of Screening Mammography.J Am Coll Radiol. 2016 Nov;13(11S):e58-e61.
Oeffinger KC, Fontham ET, Etzioni R, Herzig A, Michaelson JS, Shih YC, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599-1614.
Is one of the most serious complications in endocrine surgery:
It is related to significant morbidity and frequent malpractice litigation
The recurrent laryngeal nerve:
Originates from the:
Trunk of the vagus nerve
Upon reaching the larynx:
It is renamed the inferior laryngeal nerve
It innervates all the intrinsic muscles of the same side:
With the exception of the cricothyroid muscles
It supplies sensory innervation to the laryngeal mucosa:
Below the true vocal folds
While ascending:
The nerve on the right and on the left side:
Delivers branches that supply the trachea and the esophagus
The morphologic appearance and course of the recurrent laryngeal nerve:
Are subject to great anatomic variability
In addition, it may often be overlooked:
That the nerve most frequently does not consist only of a single trunk but exhibits a network of smaller branches
On the right side:
It usually loops around and behind the subclavian artery and then ascends into the neck in the tracheoesophageal groove:
To enter the larynx distal to the inferior cornu of the thyroid cartilage
In instances of embryologic malformation of the aortic arch:
In terms of retroesophageal right subclavian artery:
The nerve passes with a more median course directly to the larynx (non-recurrent laryngeal nerve):
Although the reported incidence of non-recurrent laryngeal nerve is less than 1%:
The surgeon has to be aware of the existence of this rare anatomic condition
The left recurent laryngeal nerve:
Courses upward around the ligamentum arteriosum and the aortic arch and runs vertically toward the tracheoesophageal groove:
On their way to the cricothyroid muscle where they enter the larynx
Both nerves run close to the capsule of the lateral aspect of the thyroid and cross the inferior thyroid artery:
Several variations of the relationship between the nerve and the artery, particularly on the right side, can be observed:
The nerve may pass superficially to the artery, deep to it, or between the branches of the vessel
After running into the laryngeal wall:
The nerve separates into two branches that supply the innervation of various laryngeal muscles:
A third branch that serves as a connection with the superior laryngeal nerve
During cervical exploration the recurrent laryngeal nerve can be exposed at different levels:
Caudally:
At the crossing with the common carotid artery
In the neighborhood of the inferior thyroid artery
Cranially:
At Berry’s ligament:
A dense condensation of the posterior thyroid capsule near the cricoid cartilage and upper tracheal rings
In addition to visual identification:
The nerve can be located by direct palpation of the tracheal wall below the lower thyroid pole
Considerable debate has long existed concerning the necessity of deliberate exposure of the recurrent laryngeal nerve during thyroid surgery:
Kocher commented on postoperative hoarseness and stated that:
Following his technique of thyroid dissection, injury to the nerve can with certainty be avoided without the direct exposure
The first surgeon who advocated routine dissection and demonstration of the nerves in 1911 was:
August Bier of Berlin
He was followed by Frank Lahey of Boston in 1938
Others advocated that exposure itself:
Is a risk due to potential induction of local edema by dissection of adjacent tissues and hemorrhage
Following these initial experiences, several studies revealed that depending upon the skill of an individual surgeon principal identification of the nerve reduces the risk of permanent laryngeal nerve injuries from over 5% to less than 1%
Nowadays, the practice of visual identification of the nerve represents the gold standard
To alleviate the visual identification of the nerve and to provide an intraoperative tool to prove its functional integrity, diverse monitoring methods, i.e., intramuscular vocal cord electrodes inserted either through the cricothyroid membrane or placed endoscopically, endotracheal tube surface electrodes, endoscopic visualization of the vocal cords in combination with nerve stimulation, and palpation of the cricoarytenoid muscle with simultaneous neural stimulation, have been developed
Although intraoperative neuromonitoring might be of use in the presence of extended thyroid surgery, particularly in a patient with a preoperatively documented vocal cord paralysis or in difficult anatomic situations:
It does not further reduce the low risk of permanent recurrent nerve lesions and it fails to reliably predict the outcome:
This experience has been found not only in primary but also in reoperative thyroid and parathyroid procedures
Damage to the recurrent laryngeal nerve may be caused by different mechanisms:
Cutting
Clamping
Stretching of the nerve
Nerve skeletonization
Local compression of the nerve:
Due to edema or hematoma
Thermal injury by electrocoagulation
Transient cord paresis:
Which is often caused by edema or axon damage by excessive nerve stretching:
Seldom lasts more than 4 to 6 weeks
When no restitution of function is notable within 6 to 12 months postoperatively:
Permanent damage should be assumed
Accidental injury to the recurrent laryngeal nerve is not recognized during surgery in most of the cases:
If the surgeon is aware of this complication intraoperatively:
Primarily repair of the nerve using microsurgical techniques and epineural sutures or a cable graftfrom the greater auricular nerve can be attempted
Even if the nerve is reanastomosed, the dysfunctioning vocal cord will probably never completely recover
Delayed nerve repairs are virtually always ineffective in restoring cord function
When a paralyzed vocal cord stays in the paramedian position:
The patients frequently remain asymptomatic:
This phenomenon is due to compensatory overadduction of the intact cord and consecutive constriction of the glottic chink
The majority of asymptomatic patients need no special treatment but close observation
Unless routine indirect laryngoscopy or videostroboscopy is performed:
Many cases of vocal cord paresis will remain unrecognized
The some authors recommend preoperative and postoperative laryngoscopic examination of the vocal cord function:
Not only for medicolegal reasons but also to document potential preexisting pathologies and consecutively adapt the surgical approach
If the paretic cord moves to the lateralized position:
Hoarseness or aspiration can occur
The prognosis considering gain of normal function is favorable in cases of delayed onset of symptoms:
In symptomatic patients either treatment by a speech and language pathologist or invasive interventions such as injection laryngoplasty or medialization laryngoplasty are necessary
References:
Beldi G, Kinsbergen T, Schlumpf R (2004) Evaluation of intraoperative recurrent nerve monitoring in thyroid surgery. World J Surg 28:589–591
Hermann M, Hellebart C, Freissmuth M (2004) Neuromonitoring in thyroid surgery: prospective evaluation of intraoperative electrophysiological responses for the prediction of recurrent laryngeal nerve injury. Ann Surg 240:9–17
Dralle H, et al (2004) Risk factors of paralysis and func- tional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery 136:1310–1322
Post-operative bleeding will characteristically be prefaced by:
Respiratory distress
Pain
Cervical pressure
Dysphagia
Increased blood drainage
No specific perioperative risk factors:
That would allow identification of the high-risk patient population for this potentially lethal complication are known
High surgical volume:
Does not reduce the incidence of hematoma formation:
Consequently, the key issue of prevention is:
Attention to anatomic detail and careful hemostasis during surgery
If the surgeon is uncertain about the dryness of the operative field:
A Valsalva maneuver:
Which elevates the intrapulmonary pressure to 40 cm H20:
Facilitates recognition of bleeding vessels:
Can be performed prior to wound closure
Routine use of suction drains:
Does not prevent postoperative cervical bleeding
In the majority of patients, symptomatic hemorrhage:
Occurs between 6 and 12 hours after the initial operation
Since in approximately 20% of cases the onset of hematoma symptoms:
Is reported beyond 24 hours postoperatively:
Ambulatory surgery with a 4- to 8-hour observation period might harbor risk of delayed intervention
Once recognized:
The wound should be deliberately re-opened, and the hematoma evacuated
In case of significant respiratory distress:
Emergency bedside hematoma evacuation, if necessary, in combination with endotracheal intubation, is required
The requirement for tracheotomy either in the emergency setting or due to persisting airway obstruction after hematoma removal is generally a rare event
Reference:
Burkey SH, et al (2001) Reexploration for symptomatic he- matomas after cervical exploration. Surgery 130:914–920
Wound infections, usually caused by Staphylococcus or Streptococcus species are considered to be rare events in thyroid surgery:
Occurring in 0.3% to 0.8% of cases
Antibiotic prophylaxis:
Is recommended only in immunocompromised patients or in those with valvular cardiac disorders
While mild neck cellulitis frequently regresses under conservative treatment:
Abscesses require rapid incision and evacuation:
Delay of invasive treatment can result in devastating mediastinitis
Clinically evident seromas:
Respond well to percutaneous aspiration
References:
Sosa JA, et al (1998) The importance of surgeon experience for clinical and economic outcomes from thyroidectomy. Ann Surg 228:320–330
Rosato L, et al (2004) Complications of thyroid surgery: analysis of a multicentric study on 14,934 patients oper- ated on in Italy over 5 years. World J Surg 28:271–276
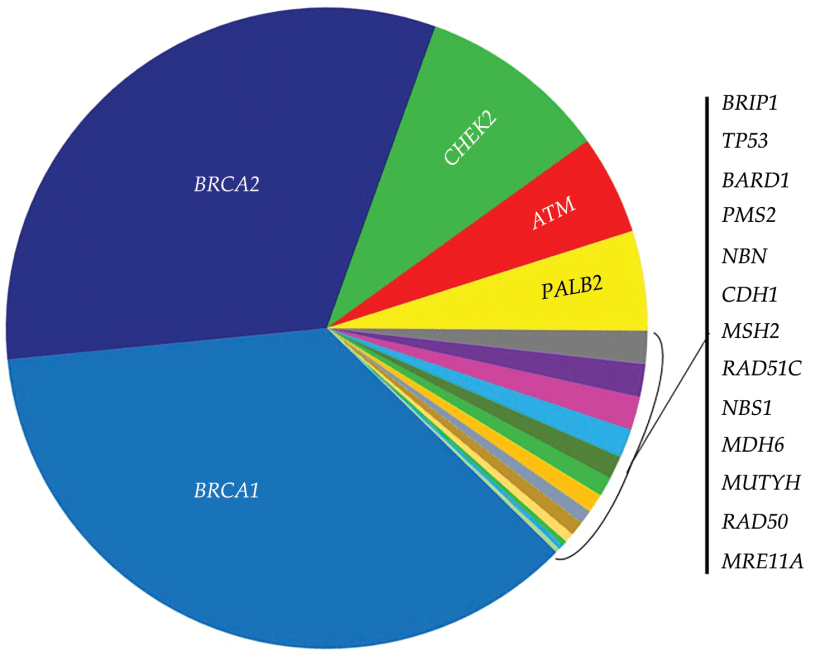
Factors associated with increased contralateral breast cancer risks include:
Genetic mutations:
Such as:
BRCA1 mutations
BRCA 2 mutations
Chek2 mutations
Atm mutations
Palb2 mutations
History of mantle radiation
First-degree relative with breast cancer
Young age at diagnosis
Hormone negative disease
To consider contralateral prophylactic mastectomy (CPM):
The disease burden of the primary tumor needs to be lower than the risk of contralateral breast cancer
For an average risk patient:
Contralateral cancer risk ranges from 1% to 5%
Markov models for stage 1 and 2 breast cancer patients:
Showed overall survival benefit of less than 1% in patients who had CPM
CPM may offer a survival advantage for:
Women less than 50 years of age who are diagnosed with triple negative breast cancer
References
Deshmukh AA, Cantor SB, Crosby MA, Dong W, Shen Y, Bedrosian I, et al. Cost of contralateral prophylactic mastectomy. Ann Surg Oncol. 2014;21(9):2823-2830.
Roberts A, Habibi M, Frick KD. Cost-effectiveness of contralateral prophylactic mastectomy for prevention of contralateral breast cancer. Ann Surg Oncol. 2014;21(7):2209-2217.
Frost MH, Hoskin TL, Hartmann LC, Degnim AC, Johnson JL, Boughey JC. Contralateral prophylactic mastectomy: long-term consistency of satisfaction and adverse effects and the significance of informed decision-making, quality of life, and personality traits. Ann Surg Oncol. 2011;18(11):3110-3116.
Barton MB, West CN, Liu IL, Harris EL, Rolnick SJ, Elmore JG, et al. Complications following bilateral prophylactic mastectomy. J Natl Cancer Inst Monogr. 2005;(35):61-66.
Grann VR, Jacobson JS, Whang W, Hershman D, Heitjan DF, Antman KH, et al. Prevention with tamoxifen or other hormones versus prophylactic surgery in BRCA1/2-positive women: a decision analysis. Cancer J Sci Am. 2000;6(1):13-20.
Portschy PR, Kuntz KM, Tuttle TM. Survival outcomes after contralateral prophylactic mastectomy: a decision analysis. J Natl Cancer Inst. 2014;106(8).
Once a patient undergoes breast-conserving surgery:
The pathology report is reviewed to determine any need for additional surgery
If the sentinel node biopsy was negative:
No additional axillary surgery is warranted
Margins assessed next:
Historically, the definition of what was considered an adequate margin in patients undergoing breast-conserving surgery was left to the interpretation of the treating physicians
In 2013, the Society of Surgical Oncology and the American Society for Radiation Oncology released consensus guidelines to assist physicians and patients in decisions regarding margins:
These guidelines were based on:
A meta-analysis of 33 studies evaluating in-breast tumor recurrence (IBTR) in relation to margin width
The results of the meta-analysis reported:
Positive margins were associated with 2-fold risk of IBTR:
Routine re-excision is recommended for those patients
For those with negative margins (defined as “no ink on tumor”), the meta-analysis reported that:
Increasing margin widths were not associated with a reduction in IBTR.
Is the patient a candidate for adjuvant therapy?
The 21-gene recurrence assay:
Has been shown to accurately predict risk of distant recurrence and benefit of adjuvant chemotherapy:
In women with ER positive tumors
Adjuvant chemotherapy is a category 1 recommendation for women with:
ER negative tumors greater than 1 cm
Does this patient need genetic studies?
The incidence of BRCA mutations in women with triple negative breast cancers:
Ranges in the literature from 10% to 31%
Current guidelines state that women who present with triple negative histology prior to age 60 should be considered for testing
References
Moran MS, Schnitt SJ, Giuliano AE, Harris JR, Khan SA, Horton J, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole breast irradiation in Stage I and II invasive breast cancer. Int J Radiat Oncol BiolPhys. 2014;88(3):553–564.
Greenup R, Buchanan A, Lorizio W, Rhoads K, Chan S, Leedom T, et al. Prevalence of BRCA mutations among women with triple negative breast cancer in a genetic counseling cohort. Ann Surg Oncol. 2013;20:3254-3258.
Pseudoangiomatous stromal hyperplasia (PASH) of breast:
Is a benign proliferative breast disease
It was first described by Vuitch, Erlandson, and Rosen:
In 1986
This lesion is characterized by:
A dense, collagenous proliferation of mammary stroma:
Forming inter-anastomosing capillary-like spaces
The age of presentation of PASH is usually:
12 to 70 years:
With most cases appearing in women:
In their late 30s to 40s
Both males and females are affected:
In men, PASH may occur with gynecomastia
It is seen in all racial and ethnic groups
PASH is usually discovered incidentally:
During screening mammography:
It may resemble a fibroadenoma on imaging
It usually appears as:
An oval, hypoechoic, or mixed echogenic mass without posterior shadowing
PASH may also occur as a:
Firm, painless, often rubbery and mobile mass in the breast:
Small tumors may be asymptomatic
Usually only one breast is affected:
Though it may be bilateral
May present as multifocal nodules in 60% of cases
When PASH occurs as a mass:
It is usually a firm and painless mass
It may occur occasionally in a pregnant woman:
In which case it can enlarge rapidly
Observation of asymptomatic PASH is appropriate:
Excision is not required
If PASH occurs as a mass and is symptomatic:
A simple excision may be performed:
However, not all PASH lesions need to be excised
With an asymptomatic and incidentally identified lesion diagnosed pathologically as PASH:
Routine follow-up is the appropriate treatment
On gross examination:
PASH is usually a well-circumscribed fibrous mass
Cysts may occasionally be found within the lesion
Microscopically:
PASH consists of a network of slit-like spaces lined by myofibroblasts that resemble ectatic vessels, with intervening stromal collagen fibers
The term “pseudoangiomatous” is used to describe this lesion:
As it has been confused and occasionally misdiagnosed as low-grade angiosarcoma
Though a new finding on mammogram or examination would be evaluated to rule out breast cancer:
There is no increased risk of breast cancer associated with the diagnosis of PASH
PASH may be mistaken for mammary angiosarcoma:
But is not associated with an increased risk of developing:
Angiosarcoma
Invasive ductal carcinoma, or
Other breast malignancies
There is no indication for genetic counseling or testing:
Based on a diagnosis of PASH
Excisional biopsy is not required:
With concordant and benign findings on mammography and core biopsy
It is thought that hormonal factors play an important role in PASH:
According to Anderson et al:
This lesion represents an important hyper-response to progesterone and estrogen
PASH is a common histological finding in breast biopsy specimens and can also be found in a normal breast that is in association with proliferative or non-proliferative fibrocystic changes:
But it is rarely a symptomatic lesion
PASH can be found in:
Teenage girls as well as in postmenopausal women with or without hormonal therapy replacement
It is important to recognize this entity because it can be easily confused with:
Other benign tumors, such as:
Fibroadenoma
Phyllode tumor
With malignant tumors, such as:
Angiosarcoma
Unfortunately, imaging features of PASH are non-specific:
On mammography:
The most common appearance described is:
A well-defined, uncalcified mass, with regular borders
Spiculated borders, suspicious borders, and architectural distortion can also be seen:
But are uncommon
On ultrasound:
PASH tends to be:
An oval, round hypoechoic mass or
Can presents as a heterogeneous mass with cystic areas
According to Cohen et al:
When a focal lesion with well-defined borders, containing no calcifications on mammography or a well-defined hypoechoic mass on ultrasound is seen:
PASH can be considered and included in the differential diagnosis
Clinically and on imaging, the differential diagnosis include:
Fibroadenoma:
Especially in young patient
Phyllode tumor:
In older women
Histologically:
PASH can be very similar to low-grade angiosarcoma
Definitive diagnosis is based on histology:
But unlike low-grade angiosarcoma:
PASH lacks of invasive features and contains no necrosis, mitoses, and no destruction of mammary epithelial structures
Management of PASH depends on presentation:
When PASH is incidentally discovered or when it is asymptomatic:
It can be followed up yearly by ultrasound or mammography for a period of 36 months
Surgical procedures are indicated for:
Symptomatic lesion with mechanical complaints, pain or apprehension for an alternative malignant lesion
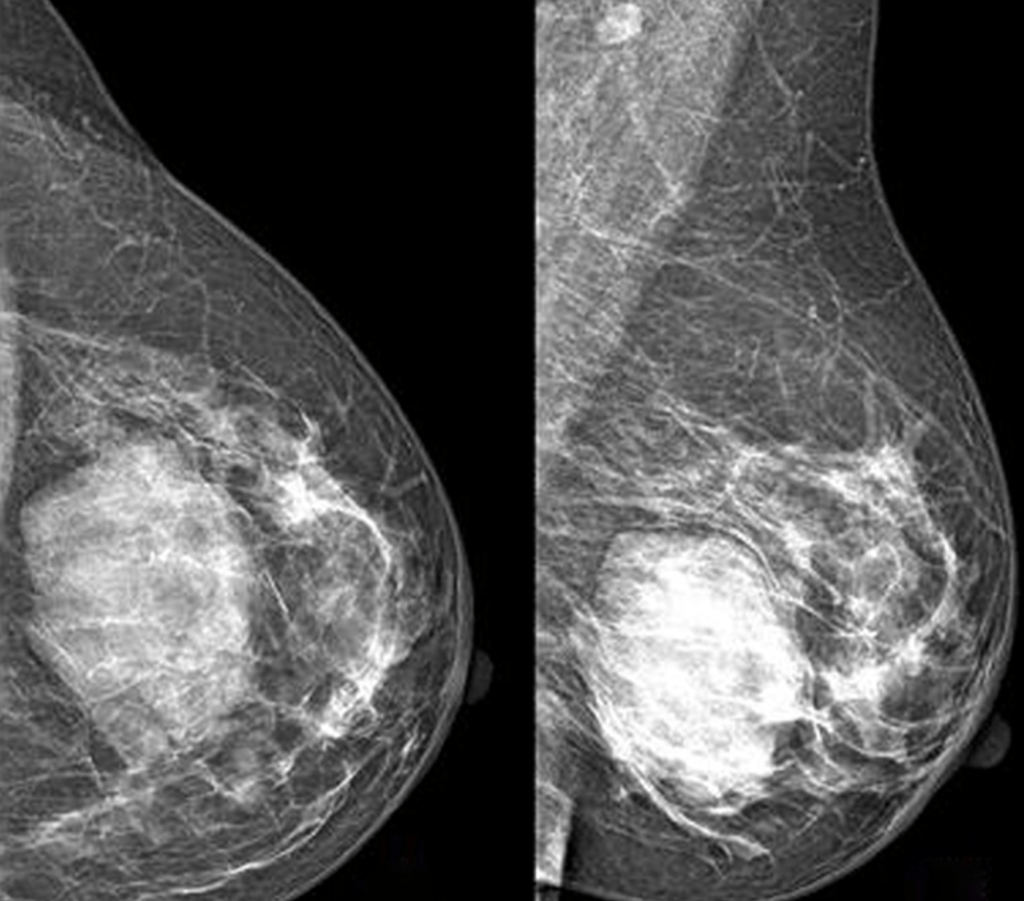
Image: Mammography performed with craniocaudal (A) and mediolateral oblique (B) incidences of the left breast shows a huge well-defined mass located between the inner and the outer inferior quadrants, with no suspicious features
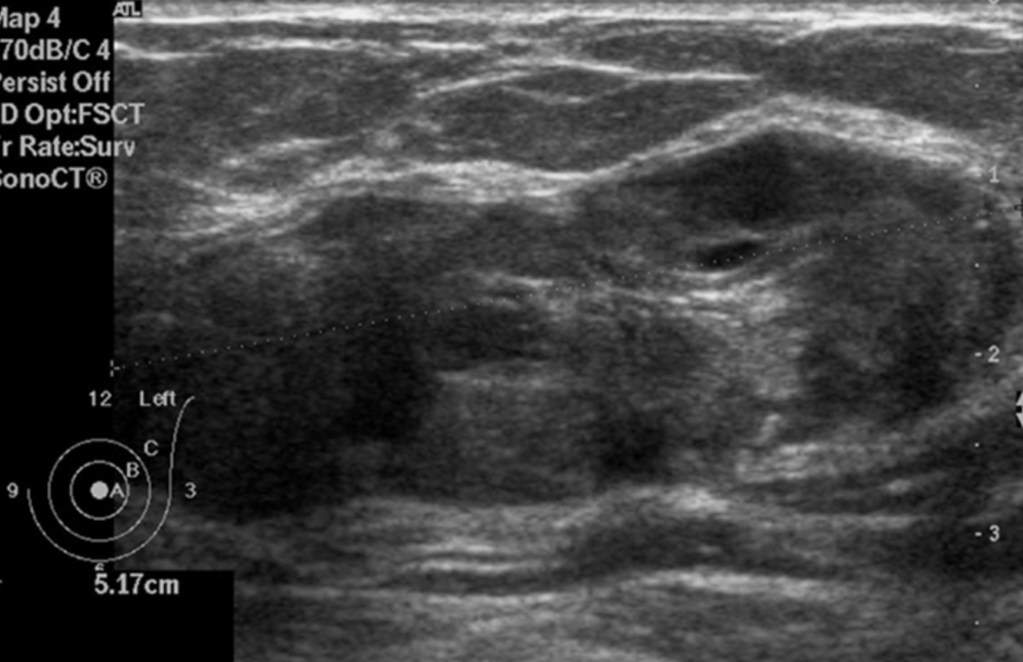
Image: Ultrasound of the left breast centered on the palpable lump showing an oval, heterogeneous lesions with smooth borders.
Mammography performed with craniocaudal (A) and mediolateral oblique (B) incidences of the left breast shows a huge well-defined mass located between the inner and the outer inferior quadrants, with no suspicious featuresUltrasound of the left breast centered on the palpable lump showing an oval, heterogeneous lesions with smooth borders.
References:
Celliers L, Wong DD, Bourke A. Pseudoangiomatous stromal hyperplasia: a study of the mammographic and sonographic features. Clin Radiol. 2010;65(2):145-149.
Guray M, Sahin AA. Benign breast diseases: classification, diagnosis, and management. Oncologist. 2006;11(5):435-439.
Hargaden GC, Yeh ED, Georgian-Smith D, Moore RH, Rafferty EA, et al. Analysis of the mammographic and sonographic features of pseudoangiomatous stromal hyperplasia. AJR Am J Roentgenol. 2008;191(2):359-363.
Salvador R, Lirola JL, Domínguez R, López M, Risueño N. Pseudo-angiomatous stromal hyperplasia presenting as a breast mass: imaging findings in three patients. Breast. 2004;13(5):431-435.
Gresik CM, Godellas C, Aranha GV, Rajan P, Shoup M. Pseudoangiomatous stromal hyperplasia of the breast: a contemporary approach to its clinical and radiologic features and ideal management. Surgery. 2010;148:752-757.
Virk RK, Khan A. Pseudoangiomatous stromal hyperplasia: an overview. Arch Pathol Lab Med. 2010;134:1070-1074.
Neal L, Sandhu NP, Hieken TJ, Glazebrook KN, Mac Bride MB, Dilaveri CA, et al. Diagnosis and management of benign, atypical, and indeterminate breast lesions detected on core needle biopsy. Mayo Clin Proc. 2014; 89:536-547.
Degnim AC , Frost MH, Radisky DC, Anderson SS, Vierkant RA, Boughey JC, et al. Pseudoangiomatous stromal hyperplasia and breast cancer risk. Ann Surg Oncol. 2010;17(12):3269-3277.
Is the standard of care for the majority of invasive breast cancers:
That are clinically node-negative regardless of patient age
Locally advanced cancers (T3-T4):
Are still considered contraindications to sentinel lymph node biopsy, thus inflammatory cancer (T4d):
Makes her only axillary staging option:
An axillary lymph node dissection
Sentinel node biopsy is prohibited by virtue of the inflammatorydiagnosis:
As the diagnosis suggests the dermal lymphatics are compromised with tumor
While some studies have shown a higher false negative rate in patients undergoing sentinel lymph node biopsy after neo-adjuvant chemotherapy:
This does not appear to affect axillary recurrence or survival:
Leading to current consensus guidelines that it is safe in this population
Several studies have shown that sentinel lymph node biopsy is safe in:
Multifocal and multicentric disease.
There is no accurate axillary imaging that currently can replace sentinel lymph node biopsy in breast cancer
References
Lyman GH, Temin S, Edge SB, Newman LA, Turner RR, Weaver DL, et al. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2014;32(13):1365-1383.
Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, Costantino JP, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010;11(10):927-933.
Mamounas EP, Brown A, Anderson S, Smith R, Julian T, Miller B, Bear HD, et al. Sentinel node biopsy after neoadjuvant chemotherapy in breast cancer: results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol 2005;23(12):2694-2702.
Geng C, Chen X, Pan X, Li J. The feasibility and accuracy of sentinel lymph node biopsy in initially clinically node-negative breast cancer after neoadjuvant chemotherapy: a systematic review and meta-analysis. PLoS One. 2016;11(9):e0162605.
Knauer M, Konstantiniuk P, Haid A, Wenzl E, Riegler-Keil M, Pöstlberger S, et al. Multicentric breast cancer: a new indication for sentinel node biopsy–a multi-institutional validation study. J Clin Oncol.2006;24(21):3374-3380.
Can be a very useful tool in both the diagnosis and staging of breast cancer
Based on the Surveillance, Epidemiology, and End Results (SEER) Program database and Medicare data pre-operative breast MRI use:
Has increased from:
5.9% to 22.4% for ductal carcinoma in situ (DCIS)
7.0% to 24.3% for invasive cancer
In cases such as invasive lobular disease:
Pre-operative MRI has been shown to decrease the rate of re-excision:
However, data on the benefit of routine pre-operative breast MRI are mixed:
With some studies showing an increase in mastectomy rate:
While other studies have not shown an increase in mastectomy rate
Contralateral mastectomy has also been shown to be higher in those with pre-operative MRI
When all tumor types were considered:
There was consistently no difference in the rate of re-excision in those undergoing pre-operative MRI vs. no MRI
A recent meta-analysis showed that pre-operative MRI:
Was associated with increased odds of receiving ipsilateral mastectomy and contralateral prophylactic mastectomy with no difference in rates of re-excision, re-operation, or positive margins:
Therefore, use of MRI should be an individualized decision, and routine use in all patients is not appropriate
References
Henderson LM, Weiss J, Hubbard RA, O’Donoghue C, DeMartini WB, Buist DS, Kerlikowske K, Goodrich M, Virnig B, Tosteson AN, Lehman CD, Onega T. Factors Associated with Preoperative Magnetic Resonance Imaging Use among Medicare Beneficiaries with Nonmetastatic Breast Cancer. Breast J. 2016 Jan-Feb;22(1):24-34. doi: 10.1111/tbj.12522. Epub 2015 Oct 28.
Mann RM, Loo CE, Wobbes T, Bult P, Barentsz JO, Gilhuijs KG, Boetes C. The impact of preoperative breast MRI on the re-excision rate in invasive lobular carcinoma of the breast. Breast Cancer Res Treat. 2010 Jan;119(2):415-22. doi: 10.1007/s10549-009-0616-6.
Houssami N, Turner RM, Morrow M. Meta-analysis of pre-operative magnetic resonance imaging (MRI) and surgical treatment for breast cancer. Breast Cancer Res Treat. 2017;165(2):273-283.
Fancellu A, Soro D, Castiglia P, Marras V, Melis M, Cottu P, et al. Usefulness of magnetic resonance in patients with invasive cancer eligible for breast conservation: a comparative study. Clin Breast Cancer. 2014;14(2):114-121.
Fancellu A, Turner RM, Dixon JM, Pinna A, Cottu P, Houssami N. Meta-analysis of the effect of preoperative breast MRI on the surgical management of ductal carcinoma in situ. Br J Surg. 2015;102(8):883-893.
Parsyan A, Moldoveanu D, Balram B, Wong S, Zhang DD, Svadzian A, et al. Influence of preoperative magnetic resonance imaging on the surgical management of breast cancer patients. Am J Surg. 2016;211(6):1089-1094.