Pseudoangiomatous Stromal Hyperplasia (PASH)
- Introduction:
- Pseudoangiomatous stromal hyperplasia (PASH) of breast:
- Is a benign proliferative breast disease
- It was first described by Vuitch, Erlandson, and Rosen:
- In 1986
- This lesion is characterized by:
- A dense, collagenous proliferation of mammary stroma:
- Forming inter-anastomosing capillary-like spaces
- A dense, collagenous proliferation of mammary stroma:
- The age of presentation of PASH is usually:
- 12 to 70 years:
- With most cases appearing in women:
- In their late 30s to 40s
- With most cases appearing in women:
- 12 to 70 years:
- Both males and females are affected:
- In men, PASH may occur with gynecomastia
- It is seen in all racial and ethnic groups
- PASH is usually discovered incidentally:
- During screening mammography:
- It may resemble a fibroadenoma on imaging
- During screening mammography:
- It usually appears as:
- An oval, hypoechoic, or mixed echogenic mass without posterior shadowing
- Pseudoangiomatous stromal hyperplasia (PASH) of breast:
- PASH may also occur as a:
- Firm, painless, often rubbery and mobile mass in the breast:
- Small tumors may be asymptomatic
- Usually only one breast is affected:
- Though it may be bilateral
- May present as multifocal nodules in 60% of cases
- Firm, painless, often rubbery and mobile mass in the breast:
- When PASH occurs as a mass:
- It is usually a firm and painless mass
- It may occur occasionally in a pregnant woman:
- In which case it can enlarge rapidly
- Observation of asymptomatic PASH is appropriate:
- Excision is not required
- If PASH occurs as a mass and is symptomatic:
- A simple excision may be performed:
- However, not all PASH lesions need to be excised
- A simple excision may be performed:
- With an asymptomatic and incidentally identified lesion diagnosed pathologically as PASH:
- Routine follow-up is the appropriate treatment
- On gross examination:
- PASH is usually a well-circumscribed fibrous mass
- Cysts may occasionally be found within the lesion
- Microscopically:
- PASH consists of a network of slit-like spaces lined by myofibroblasts that resemble ectatic vessels, with intervening stromal collagen fibers
- The term “pseudoangiomatous” is used to describe this lesion:
- As it has been confused and occasionally misdiagnosed as low-grade angiosarcoma
- Though a new finding on mammogram or examination would be evaluated to rule out breast cancer:
- There is no increased risk of breast cancer associated with the diagnosis of PASH
- PASH may be mistaken for mammary angiosarcoma:
- But is not associated with an increased risk of developing:
- Angiosarcoma
- Invasive ductal carcinoma, or
- Other breast malignancies
- But is not associated with an increased risk of developing:
- There is no indication for genetic counseling or testing:
- Based on a diagnosis of PASH
- Excisional biopsy is not required:
- With concordant and benign findings on mammography and core biopsy
- It is thought that hormonal factors play an important role in PASH:
- According to Anderson et al:
- This lesion represents an important hyper-response to progesterone and estrogen
- According to Anderson et al:
- PASH is a common histological finding in breast biopsy specimens and can also be found in a normal breast that is in association with proliferative or non-proliferative fibrocystic changes:
- But it is rarely a symptomatic lesion
- PASH can be found in:
- Teenage girls as well as in postmenopausal women with or without hormonal therapy replacement
- It is important to recognize this entity because it can be easily confused with:
- Other benign tumors, such as:
- Fibroadenoma
- Phyllode tumor
- With malignant tumors, such as:
- Angiosarcoma
- Unfortunately, imaging features of PASH are non-specific:
- On mammography:
- The most common appearance described is:
- A well-defined, uncalcified mass, with regular borders
- Spiculated borders, suspicious borders, and architectural distortion can also be seen:
- But are uncommon
- The most common appearance described is:
- On ultrasound:
- PASH tends to be:
- An oval, round hypoechoic mass or
- Can presents as a heterogeneous mass with cystic areas
- PASH tends to be:
- According to Cohen et al:
- When a focal lesion with well-defined borders, containing no calcifications on mammography or a well-defined hypoechoic mass on ultrasound is seen:
- PASH can be considered and included in the differential diagnosis
- When a focal lesion with well-defined borders, containing no calcifications on mammography or a well-defined hypoechoic mass on ultrasound is seen:
- On mammography:
- Clinically and on imaging, the differential diagnosis include:
- Fibroadenoma:
- Especially in young patient
- Phyllode tumor:
- In older women
- Fibroadenoma:
- Histologically:
- PASH can be very similar to low-grade angiosarcoma
- Definitive diagnosis is based on histology:
- But unlike low-grade angiosarcoma:
- PASH lacks of invasive features and contains no necrosis, mitoses, and no destruction of mammary epithelial structures
- But unlike low-grade angiosarcoma:
- Management of PASH depends on presentation:
- When PASH is incidentally discovered or when it is asymptomatic:
- It can be followed up yearly by ultrasound or mammography for a period of 36 months
- Surgical procedures are indicated for:
- Symptomatic lesion with mechanical complaints, pain or apprehension for an alternative malignant lesion
- When PASH is incidentally discovered or when it is asymptomatic:
- Other benign tumors, such as:
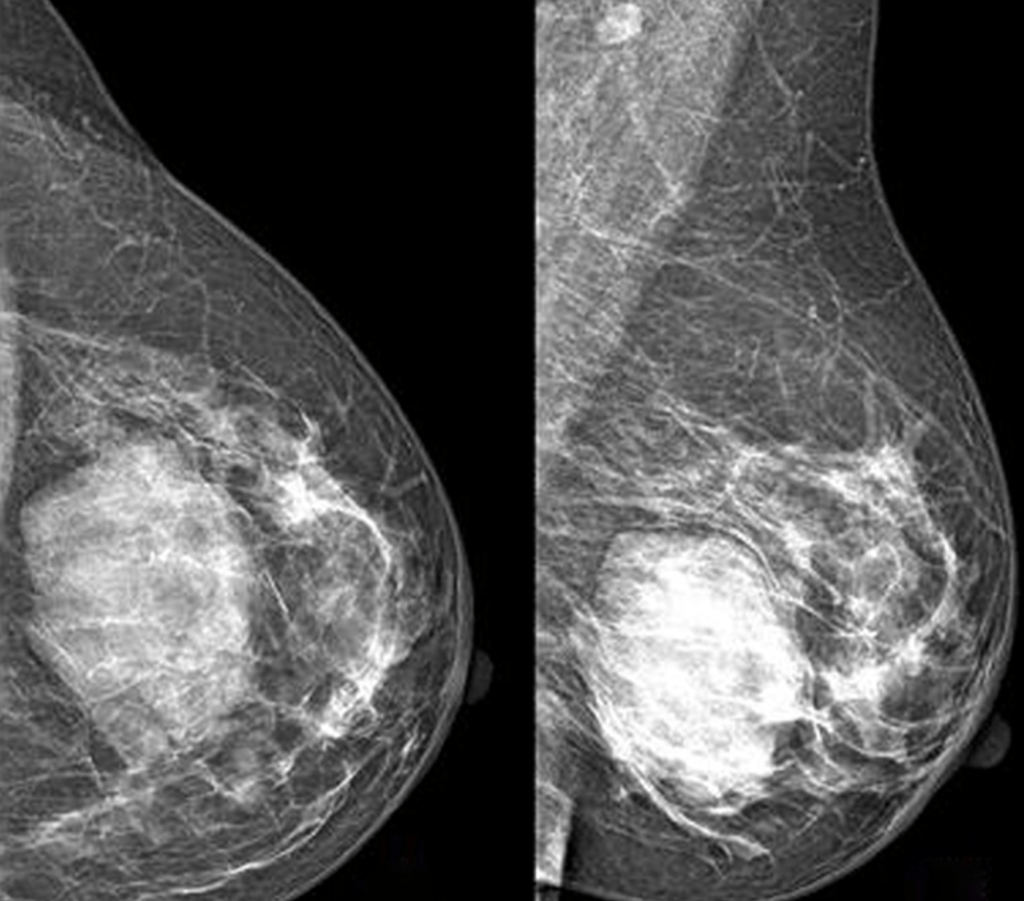
Image: Mammography performed with craniocaudal (A) and mediolateral oblique (B) incidences of the left breast shows a huge well-defined mass located between the inner and the outer inferior quadrants, with no suspicious features
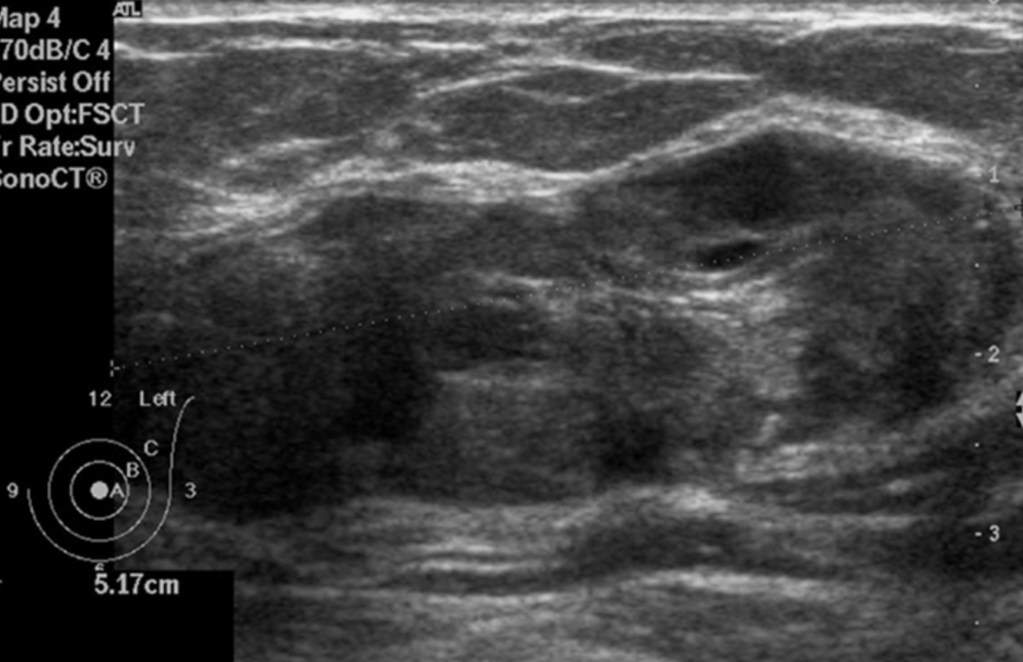
Image: Ultrasound of the left breast centered on the palpable lump showing an oval, heterogeneous lesions with smooth borders.
- References:
- Celliers L, Wong DD, Bourke A. Pseudoangiomatous stromal hyperplasia: a study of the mammographic and sonographic features. Clin Radiol. 2010;65(2):145-149.
- Guray M, Sahin AA. Benign breast diseases: classification, diagnosis, and management. Oncologist. 2006;11(5):435-439.
- Hargaden GC, Yeh ED, Georgian-Smith D, Moore RH, Rafferty EA, et al. Analysis of the mammographic and sonographic features of pseudoangiomatous stromal hyperplasia. AJR Am J Roentgenol. 2008;191(2):359-363.
- Salvador R, Lirola JL, Domínguez R, López M, Risueño N. Pseudo-angiomatous stromal hyperplasia presenting as a breast mass: imaging findings in three patients. Breast. 2004;13(5):431-435.
- Vuitch MF, Rosen PP, Erlandson RA. Pseudoangiomatous hyperplasia of mammary stroma. Hum Pathol. 1986;17(2):185-191.
- Gresik CM, Godellas C, Aranha GV, Rajan P, Shoup M. Pseudoangiomatous stromal hyperplasia of the breast: a contemporary approach to its clinical and radiologic features and ideal management. Surgery. 2010;148:752-757.
- Virk RK, Khan A. Pseudoangiomatous stromal hyperplasia: an overview. Arch Pathol Lab Med. 2010;134:1070-1074.
- Neal L, Sandhu NP, Hieken TJ, Glazebrook KN, Mac Bride MB, Dilaveri CA, et al. Diagnosis and management of benign, atypical, and indeterminate breast lesions detected on core needle biopsy. Mayo Clin Proc. 2014; 89:536-547.
- Degnim AC , Frost MH, Radisky DC, Anderson SS, Vierkant RA, Boughey JC, et al. Pseudoangiomatous stromal hyperplasia and breast cancer risk. Ann Surg Oncol. 2010;17(12):3269-3277.
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #PseudangiomatousStromalHyperplasia #PASH #Miami #Mexico #Surgeon #Teacher
