







#Arrangoiz #ThyroidSurgeon #HeadandNeckSurgeon #CancerSurgeon #ThyroidCancer #ThyroidNodule #ThyroidMolecularAnalysis #Thyroseq #MSMC #MountSinaiMedicalCenter #Miami #Mexico
#Arrangoiz #ThyroidSurgeon #HeadandNeckSurgeon #CancerSurgeon #ThyroidCancer #ThyroidNodule #ThyroidMolecularAnalysis #Thyroseq #MSMC #MountSinaiMedicalCenter #Miami #Mexico
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncology #Surgeon #Teacher #BreastCancer #BreastExpert #MSMC #MountSinaiMedicalCenter #Miami #Mexico #SLNM #SLNB #SentinelLymphNodeBiopsy

#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #Surgeon #Teacher #BreastCancer #BreastDiseases #AxillaryDissection #BreastSurgery #MountSinaiMedicalCenter #MSMC #Miami #Mexico #SLNM #SLNB #SentinelLymphNodeBiopsy


#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #Surgeon #Teacher #BreastCancer #BreastDiseases #AxillaryDissection #BreastSurgery #MountSinaiMedicalCenter #MSMC #Miami #Mexico

#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #Surgeon #Teacher #BreastCancer #BreastDiseases #AxillaryDissection #BreastSurgery #MountSinaiMedicalCenter #MSMC #Miami #Mexico
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #Surgeon #Teacher #BreastCancer #BreastDiseases #AxillaryDissection #BreastSurgery #MountSinaiMedicalCenter #MSMC #Miami #Mexico
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #Surgeon #Teacher #BreastCancer #BreastDiseases #AxillaryDissection #BreastSurgery #MountSinaiMedicalCenter #MSMC #Miami #Mexico

#Arrangoiz #CancerSurgeon #HeadandNeckSurgeon #SurgicalOncologist #MASC #MammaryAnalogSecretoryCarcinoma #SalivaryGlandTumors #MSMC #MountSinaiMedicaCenter #Mexico #Miami
#Arrangoiz #CancerSurgeon #HeadandNeckSurgeon #SurgicalOncologist #SalivaryGlandTumors #EpithelialMyoepithelialCarcinoma #EMC #MSMC #MountSinaiMedicalCenter #Mexico #Miami
• Acinic cell carcinomas (AcCC):
• Is the second most common malignant tumor:
• Involving the parotid gland
• They represent 15% of malignant parotid gland neoplasms
• AcCC accounts for approximately:
• 5% to 17% of all salivary gland tumors:
• 10% to 17% of all malignant salivary gland tumors
• The parotid gland is composed almost exclusively of serous type acini:
• And it is the most common site of AcCC:
• 80% to 90% of cases
• Other reported sites are:
• The palate (up to 15%)
• Submandibular gland (4%)
• Sublingual gland (1%)
• AcCC occurs most often in the fifth decade of life:
• Women are affected more often than in men (ratio 3:2)
• It is generally a low-grade carcinoma:
• With indolent behavior
• Recurrences are usually delayed:
• Sometimes after decades:
• In a series reported by Ellis et al:
• 12% of tumors recurred and 8% metastasized (bone, lung, and brain)
• The regional lymph nodes:
• Were the most common site of metastases:
• Spafford et al:
• Reported cervical lymphadenopathy to be present in 10% to 15% of cases of AcCC
• Spiro et al:
• In a series of 67 cases with AcCC treated before 1968, identified five cases (7.5%) with cervical metastases at the time of initial treatment
• It is interesting that this tumor is the most common bilateral malignant salivary gland neoplasm:
• Although its bilateral presentation is not nearly as common as the bilateral presentations of benign tumors:
• Warthin’s tumor and pleomorphic adenoma
• AcCC:
• Are typically encased in a fibrous capsule:
• Grossly resembling round circumscribed nodules with a tan surface
• The cut surface is solid but may show cystic degeneration and hemorrhage
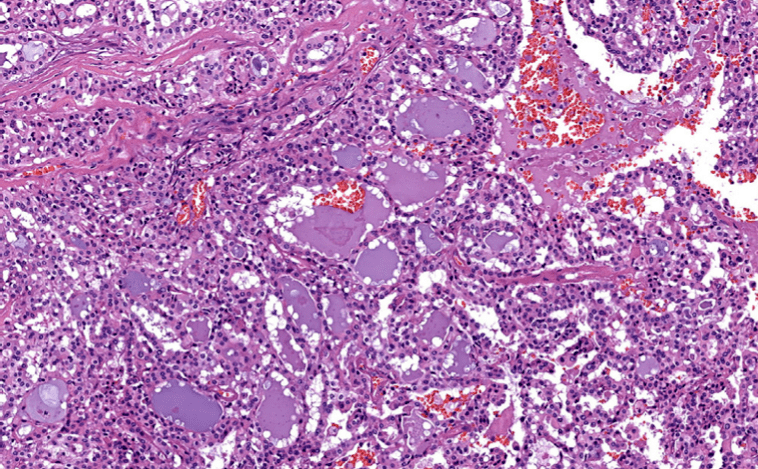
• Histologically, there are five cell types:
• Serous acinar cells:
• Explaining the predilection for the parotid gland
• Cells with clear cytoplasm
• Intercalated ductal cell
• Nonspecific glandular cell
• Vacuolated cell
• The microscopic recognition of AcCC also requires a strong appreciation for its varied growth patterns:
• There are four histologic growth patterns:
• Solid
• Microcystic
• Papillary
• Follicular
• Caution must be taken not to misread the:
• Solid pattern as normal parotid parenchyma
• The papillary-cystic pattern as cystic mucoepidermoid carcinoma
• The follicular pattern as metastatic thyroid carcinoma
• Serous acinar differentiation:
• Is developed most fully in the acinic cell:
• These cells have dark round nuclei and granular purplish cytoplasm
• The diagnosis of AcCC may be difficult to establish:
• Especially when some other cell type dominates the histopathology picture
• Some examples of this are the predominance of clear cells might cause confusion with:
• Mucoepidermoid carcinoma, clear cell adenocarcinoma, and metastatic renal cell carcinoma:
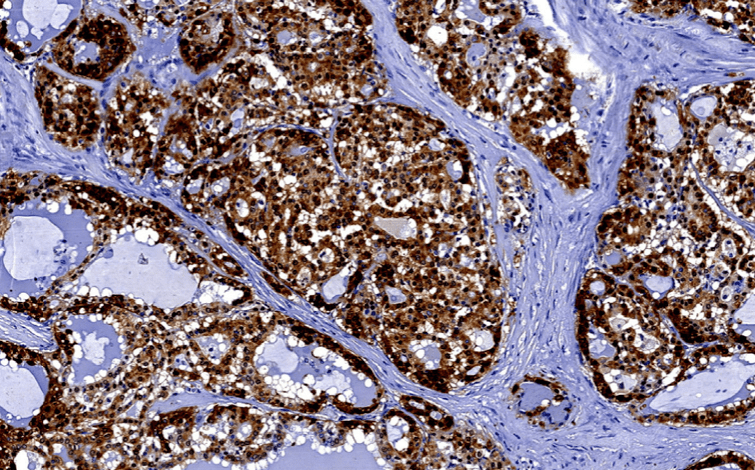
• In these circumstances, the diagnostic acinic cells can be identified using a periodic acid-Schiff (PAS) reagent:
• Their cytoplasmic secretory granules are PAS positive and diastase resistant
• Overall survival has been crudely estimated to be about 84%:
• Survival at 5 years has been reported between 76% to 90%, but fell to 56% at 20 years:
• Emphasizing the need for long- term follow-up
