- Epithelial-myoepithelial carcinoma (EMC):
- Is another typically indolent salivary gland tumor:
- That is characterized by a multi-nodular pattern and biphasic or bilayered arrangement of inner ductal cells and outer myoepithelial cells, with classically clear cytoplasm
- EMC:
- Is a rare tumor with low malignant potential:
- Accounting for less than 1 % of salivary neoplasms
- Peak incidence occurs in seventh decade:
- With a predilection for female
- As early as 1956, EMC was reported as:
- Adenomyoeipthelioma, clear cell adenoma, tubular solid adenoma and clear cell carcinoma:
- Due to its varied histopathologic appearance
- Adenomyoeipthelioma, clear cell adenoma, tubular solid adenoma and clear cell carcinoma:
- The term EMC was coined by Donath et al. in 1972:
- This discrete entity was subsequently incorporated in WHO classification of salivary gland tumors in 1991
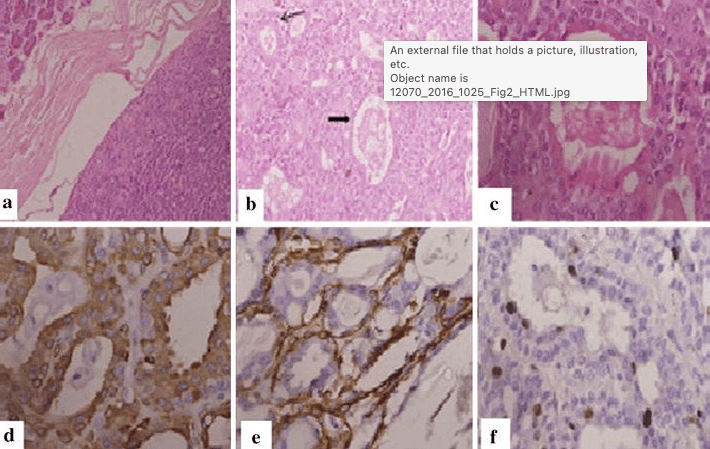
- On histopathologic examination:
- It shows dual cell population:
- Composed of luminal ductal epithelial cells (inner layer) surrounded by large polygonal clear myoepithelial cells (outer layer):
- Due to bidirectional differentiation of the stem cell
- Composed of luminal ductal epithelial cells (inner layer) surrounded by large polygonal clear myoepithelial cells (outer layer):
- It shows dual cell population:
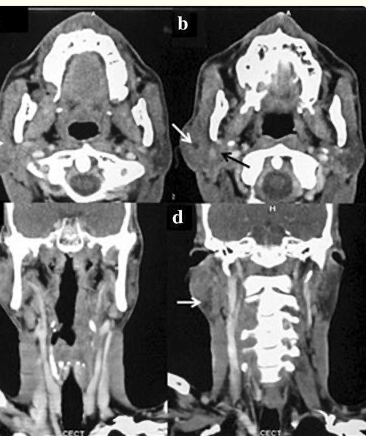
- The most common location is the parotid gland:
- Also the index case has parotid involvement:
- But it is also known to occur in submandibular gland and minor salivary glands of palate, base of tongue and rarely in breast, lung, kidney, uterus
- Also the index case has parotid involvement:
- Rarely, it may show high grade transformation of epithelial or myoepithelial component:
- Resulting in aggressive behavior
- Because of rarity of EMC a standard treatment guideline is not yet known:
- Surgical resection is the most widely used approach:
- Although, some of the reported cases have utilized post-operative radiotherapy (PORT) extrapolated from other salivary gland histologies
- Surgical resection is the most widely used approach:
- Although it is a low grade tumor:
- Local recurrence rates of 23% to 50 % have been reported:
- With 25 % chance of distant metastasis
- Local recurrence in as early as 6 months post operatively has been seen
- Local recurrence rates of 23% to 50 % have been reported:
- Histopathologic markers such as:
- Solid growth pattern, nuclear atypia, DNA aneuploidy, necrosis, positive surgical margins and high proliferative activity:
- Have been identified by some authors to be associated with more aggressive behavior and high frequency of local recurrences and metastases
- Solid growth pattern, nuclear atypia, DNA aneuploidy, necrosis, positive surgical margins and high proliferative activity:
- Surgery alone may not be sufficient in cases with histopathologic markers of aggressive behavior:
- These patients may be candidates for PORT
#Arrangoiz #CancerSurgeon #HeadandNeckSurgeon #SurgicalOncologist #SalivaryGlandTumors #EpithelialMyoepithelialCarcinoma #EMC #MSMC #MountSinaiMedicalCenter #Mexico #Miami
