A number of studies have found that lifting weights reduces the development of lymphedema.
It is also clear that air travel (whether long or short haul) does not increase the risk of lymphedema>
Sleeves are not indicated unless there is established lymphedema.
A Cochrane review found no increase in lymphedema associated with early shoulder-mobilization exercises (within 7 days of surgery), and in fact found that these were better than delayed exercises.
Weight loss, whether through reducing calories or fat intake, has been found to result in reduced lymphedema.
Studies have found that patients with a prior axillary dissection could undergo elective hand surgery (including carpal tunnel surgery) without an increase in lymphedema rates.
References:
Brown JC, Schmitz KH. Weight lifting and physical function among survivors of breast cancer: a post hoc analysis of a randomized controlled trial. J Clin Oncol. 2015;33:2184-2189.
Kilbreath SL, Ward LC, Lane K, et al. Effect of air travel on lymphedema risk in women with history of breast cancer. Breast Cancer Res Treat. 2010;120:649-654.
Stuiver MM, ten Tusscher MR, Agasi-Idenburg CS, Lucas C, Aaronson NK, Bossuyt PM. Conservative interventions for preventing clinically detectable upper limb lymphedema in patients who are at risk of developing lymphedema after breast cancer therapy. Cochrane Database Syst Rev. 2015;2:CD009765.
Background: Head and Neck Cancer is a major public health problem in India, majority of which are lifestyle related, male predominant requiring dedicated infrastructure and human resource. The 5-year survival is 59% for all stages combined and only 45% in patients with locally advanced inoperable head and neck cancer using current chemoradiation schedules. Chemotherapy agents administered in the induction or concurrent setting comprise of taxanes (Docetaxel, paclitaxel), platinum compounds (Cisplatin, carboplatin) and fluorouracil (TPF). For patients with advanced Head and neck squamous cell carcinoma (HNSCC), 3-weekly TPF regimen is the established standard induction chemotherapy (ICT) option based on overall survival benefit. However, TPF regimen is known to be associated with significant dose limiting toxicities which may impair tolerance and effectiveness of therapy. In this study we assessed the efficacy and toxicity of weekly vs. 3-weekly Docetaxel, Cisplatin, and Fluoro-uracil (TPF) induction chemotherapy in locally advanced Head and neck squamous cell carcinoma (LA-HNSCC).
Methods: This was an open labeled randomized two arm study with 41 patients in the 3-weekly TPF arm and 41 patients in the weekly arm. Patients were randomized using numbers from a randomization software, data recorded, and results were analyzed.
Results:The weekly group achieved far greater symptom relief than 3-weekly group (72 vs. 64%). The overall response rates were similar in both arms (ORR 75.6 and 73.1% in the weekly and 3-weekly groups, respectively). Renal toxicity was significantly lower in the weekly group as compared to 3 weekly arm post three cycles of chemotherapy (CrCl 91.49 ml/min vs. 76.67 ml/min, respectively). The weekly group had predominantly grade I and II neutropenia (19.5 and 17.1%, respectively) as compared to 3-weekly group where grade III and IV neutropenia (31 and 12%, respectively) was more prominent (p-0.003). Among non-hematological toxicities, mucositis, nausea/vomiting, and diarrhea in the weekly group were significantly lower when compared to 3-weekly group. Progression free survival was slightly higher in the weekly group (18 months) when compared to 3-weekly group (15 months) which was not statistically significant.
Conclusion: Weekly induction with TPF had lower toxicity and similar efficacy as compared to 3-weekly regimen in locally advanced HNSCC patients. Myelosuppression, which was the most serious and common complication of 3-weekly TPF regimens was notably low using the weekly regimen. Our results suggest that weekly TPF regimen may be a safer and effective alternative to 3-weekly TPF for treatment of LA-HNSCC. To our knowledge this is the first study reporting the efficacy of weekly TPF regimen in LA-HNSCC till date.
At a minimum follow-up of 2 years, the TAX 324 study showed a significant survival benefit of induction chemotherapy with docetaxel, cisplatin, and fluorouracil (TPF) versus cisplatin and fluorouracil (PF) in locally advanced head and neck cancer. We report the long-term results at 5 years’ minimum follow-up.
Methods
TAX 324 was a randomized, open-label phase 3 trial comparing three cycles of TPF induction chemotherapy (docetaxel 75 mg/m2, followed by intravenous cisplatin 100 mg/m2 and fluorouracil 1000 mg/m2 per day, administered as a continuous 24-h infusion for 4 days) with three cycles of PF (intravenous cisplatin 100 mg/m2, followed by fluorouracil 1000 mg/m2 per day as a continuous 24-hour infusion for 5 days) in patients with stage III or IV squamous-cell carcinoma of the head or neck. Both regimens were followed by seven weeks of chemoradiotherapy with concomitant weekly carboplatin. Randomization was done centrally with the use of a biased-coin minimization technique. At study entry, patients were stratified according to the site of the primary tumour, nodal status (N0 or N1 vs N2 or N3), and institution. For this long-term analysis, data as of Dec 1, 2008, were gathered retrospectively from patients’ medical records. Overall and progression-free survival were the primary endpoints. Tracheostomy and dependence on a gastric feeding tube were used as surrogate measures for treatment-related long-term toxicity. The intention-to-treat analysis included data from all 501 patients (255 TPF, 246 PF); data from the initial analysis in 2005 were used for 61 patients who were lost to follow-up. TAX 324 was registered at ClinicalTrials.gov, NCT00273546.
Findings
Median follow-up was 72·2 months (95% CI 68·8–75·5). Overall survival was significantly better after treatment with TPF versus PF (hazard ratio [HR] 0·74, 95% CI 0·58–0·94), with an estimated 5-year survival of 52% in patients treated with TPF and 42% in those receiving PF. Median survival was 70.6 months (95% CI 49·0–89·0) in the TPF group versus 34.8 months (22·6–48·0) in the PF group (p=0·014). Progression-free survival was also significantly better in patients treated with TPF (median 38.1 months, 95% CI 19·3–66·1, vs 13.2 months,10·6–20·7; HR 0·75, 95% CI 0·60–0·94). They detected no significant difference in dependence on gastric feeding tubes and tracheostomies between treatment groups. In the TPF group, three (3%) of 91 patients remained feeding-tube dependent, compared with eight (11%) of 71 patients in the PF group. Six (7%) of 92 patients had tracheostomies in the TPF group, versus eight (11%) of 71 in the PF group.
Interpretation
Induction chemotherapy with TPF provides long-term survival benefit compared with PF in locally advanced head and neck cancer. Patients who are candidates for induction chemotherapy should be treated with TPF.
The Head and Neck Cancer Group of the European Organization for Research and Treatment of Cancer (EORTC) conducted a phase 3 trial, called the EORTC 24971 / TAX 323 study
Background Phase 2 studies suggest that the standard regimen of cisplatin and fluorouracil (PF) plus docetaxel (TPF) improves outcomes in squamous-cell carcinoma of the head and neck. They compared TPF with PF as induction chemotherapy in patients with locoregionally advanced, unresectable disease.
Methods They randomly assigned eligible patients between the ages of 18 and 70 years who had stage III or stage IV disease and no distant metastases to receive either TPF (docetaxel and cisplatin, day 1; fluorouracil by continuous infusion, days 1 to 5) or PF every 3 weeks for four cycles. Patients without progression of disease received radiotherapy within 4 to 7 weeks after completing chemotherapy. The primary end point was progression-free survival.
The TPF regimen consisted of docetaxel at a dose of 75 mg per square meter, administered as a 1-hour infusion on day 1, fol- lowed by cisplatin at a dose of 75 mg per square meter, administered as a 1-hour infusion on day 1, and fluorouracil at a dose of 750 mg per square meter per day, administered by continuous infu- sion on days 1 to 5. The PF regimen consisted of cisplatin at a dose of 100 mg per square meter, administered as a 1-hour infusion on day 1, fol- lowed by fluorouracil at a dose of 1000 mg per square meter per day, administered by continu- ous infusion on days 1 to 5.
Results A total of 358 patients underwent randomization, with 177 assigned to the TPF group and 181 to the PF group. At a median follow-up of 32.5 months, the median pro- gression-free survival was 11.0 months in the TPF group and 8.2 months in the PF group (hazard ratio for disease progression or death in the TPF group, 0.72; P=0.007). Treatment with TPF resulted in a reduction in the risk of death of 27% (P=0.02), with a median overall survival of 18.8 months, as compared with 14.5 months in the PF group. There were more grade 3 or 4 events of leukopenia and neutropenia in the TPF group and more grade 3 or 4 events of thrombocytopenia, nausea, vomiting, stomatitis, and hearing loss in the PF group. The rates of death from toxic effects were 2.3% in the TPF group and 5.5% in the PF group.
Conclusions As compared with the standard regimen of cisplatin and fluorouracil, induction chemotherapy with the addition of docetaxel significantly improved progression- free and overall survival in patients with unresectable squamous-cell carcinoma of the head and neck. (ClinicalTrials.gov number, NCT00003888.)
Post-mastectomy radiation therapy (PMRT) is indicated for tumors greater than 5 cm with any number of involved axillary nodes, smaller cancers with four or more lymph nodes involved with metastases, and locally advanced breast cancer by the American Society of Clinical Oncology (ASCO) and American Society of Therapeutic Radiology and Oncology (ASTRO).
The 12th St. Gallen International Breast Cancer Conference also supported the recommendation for post-mastectomy radiation therapy for patients with four or more axillary lymph nodes involved with cancer metastases.
Locally-advanced breast cancer is defined as a tumor greater than 5 cm in size, tumor extending to chest wall, and tumor extending to skin in the form of nodules, ulcerations, or edema. These patient populations have a risk of local recurrence greater than 20%, which is greatly improved with post-mastectomy radiation therapy.
Some groups recommend post-mastectomy irradiation for patients with T1 or T2 tumors and any number of positive axillary lymph nodes.
A recent meta-analysis performed by the Early Breast Cancer Trialists Collaborative Group showed that adjuvant radiotherapy significantly reduced the risk of local recurrence (from 23% to 6%) for patients with node-positive disease who underwent mastectomy with axillary clearance, which in turn reduced the rates of breast cancer mortality and overall mortality.
The most recent National Comprehensive Cancer Network Guidelines also strongly recommend post-mastectomy radiation therapy to the chest wall and regional lymph node basins for patients with any nodal positivity. However, this recommendation has been controversial for patients with one to three positive nodes, as many more recent studies using modern systemic therapy have shown much lower locoregional failure rates (5% to 10% at 5 to 10 years, or lower).
Many authors suggest that looking at the total number of risk factors in an individual patient would be useful to determine if post-mastectomy radiation therapy may be beneficial clinically. In addition to tumor size and the degree of nodal involvement, such factors include young age (35 to 40 years or less), lymphovascular invasion, high tumor grade, close or positive surgical margins, hormone receptor status, lymph node ratio, and lack of receipt of systemic therapy. The survival benefit is not uniform across all risk groups. The data in the literature on these variables are conflicting, however, and there is no consensus on how to integrate these factors.
Risk for and response to radiotherapy for local regional chest-wall recurrence are increasingly being linked to biologic subtype. The finding of micrometastases in a sentinel node would prompt discussion with a radiation oncologist about the benefits of post-mastectomy radiation therapy, but currently there is no randomized or prospective evidence to support definitive use of this modality in this population.
For all patient groups, when the risk of local-regional recurrence is less than 20%, patients should be offered a balanced discussion with a radiation oncologist so they can best understand their risks for recurrence based on their specific tumor features.
Dominici LS, Mittendorf EA, Wang X, et al. Implications of constructed biologic subtype and its relationship to locoregional recurrence following mastectomy. Breast Cancer Res. 2012;14:R82.
Early Breast Cancer Trialists Collaborative Group. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomized trials. Lancet. 2014;383:2127-2135.
Khan A, Haffty BG. Postmastectomy radiation therapy. In Kuerer H, ed. Breast Surgical Oncology. New York, NY: McGraw-Hill; 2010:995-1008.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Breast Cancer. Available at http://www.nccn.org.
Sharma R, Bedrosian I, Lucci A, et al. Present-day locoregional control in patients with t1 or t2 breast cancer with 0 and 1 to 3 positive lymph nodes after mastectomy without radiotherapy. Ann Surg Oncol. 2010;17:2899-2908.
Patients with local–regionally advanced or metastatic thyroid carcinoma are a growing concern for head and neck surgeons, endocrinologists and medical oncologists. With the increasing incidence of thyroid carcinoma, now representing 5% of cancers diagnosed in women, this has resulted in over 650,000 patients living with a thyroid cancer diagnosis in the United States. Up to 30% of these patients will develop local regional recurrence and up to 15% will develop distant metastatic disease. Although surgery and radioactive iodine provide initial therapies for follicular derived carcinomas, tumors often become non-avid for radioactive iodine limiting this treatment modality. Despite the increasing number of patients with advanced thyroid carcinoma, there remains a limited set of drugs approved for advanced follicular derived thyroid carcinomas (sorafenib and lenvatinib). Ideally, molecular assessment of the tumor tissue will allow for directed therapy selection through the identification of altered biologic pathways. However, which testing methodology should be used in this patient population is debated based on time, cost, and information gained.
To better inform treatment decisions in advanced thyroid carcinoma patients, the landscape of mutational alterations particularly mutations associated with potential progression and metastasis is needed. Similarly, recognizing the distinct characteristics associated with oncogenes versus tumor suppressor genes in thyroid tumorigenesis and potential targetability is required.
BRAF V600E, a point mutation at codon 600 leading to a valine substitution to glutamic acid, represents the most common oncogene mutated in thyroid cancer occurring in 40% to 60% of papillary thyroid carcinomas,33% of poorly differentiated thyroid carcinomas, and 20% to 45% of anaplastic thyroid carcinoma.
Another oncogene, RAS, shows mutations in up to 30% of follicular carcinomas, 28% of poorly differentiated thyroid carcinoma, 24% of anaplastic thyroid carcinoma, and 10% to 20% of medullary thyroid carcinoma.
Mutations in RET proto-oncogene define hereditary medullary thyroid carcinoma and also occur in 40% to 50% of somatic cases.
Mutations in oncogenes often lead to currently “targetable therapies” either as specific gene inhibitors or often broader pathway inhibitors. Drugs targeting overactive pathways and oncogenes have expanded over the past decade. This includes a host of tyrosine kinase inhibitors and gene-specific inhibitors including BRAF V600E inhibitors, which has led to increased clinical trials in thyroid cancer.
These oncogenes are key drivers of the activated RAS–RAF–MEK–ERK signaling pathway, which contributes to thyroid carcinogenesis.
Concurrently, the recent development of a BRAF V600E specific antibody for immunohistochemical assessment has facilitated a more rapid and readily available technique for determining BRAF V600E status compared to molecular assays. This single gene testing approach fails to account for potentially altered secondary pathways, which may confer escape mechanisms. Moreover, about one third of papillary thyroid carcinomas will be BRAF V600E negative, thus limited testing leaves an unknown if other molecular alterations may exist or be of aid for therapeutic consideration (17).
Although oncogene alterations frequently occur at hotspots and are relatively easy to test, only with modern next-generation sequencing (NGS) can analysis be performed to gain insight into alterations within tumor suppressor genes. Dysregulation of TP53, a prototypic tumor suppressor gene, contributes to a vast array of tumors and is currently viewed as “nontargetable” based on current therapeutic considerations. TP53 gene mutations occur late in the progression of thyroid carcinoma with increasing incidence from papillary to poorly differentiated and finally anaplastic thyroid carcinomas. Although not currently targetable, knowledge of the presence of a TP53 mutation may be informative as a mechanism of resistance and possible biomarker portending a more aggressive clinical course.
The treatment options for DCIS are many including:
Breast conserving surgery (BCS):
With or with out radiation
Unilateral mastectomy
Bilateral mastectomy
Endocrine therapy
All have an excellent overall survival (OS)
Treatment Options:
Breast Conserving Surgery (BCS):
Wide excision alone
Wide excision with radiation (RT)
Wide excision with endocrine therapy
Wide excision with RT and endocrine therapy
Unilateral mastectomy
Bilateral mastectomy
Mastectomy:
Was considered to be the standard of care in the surgical management for all breast cancers, including:
DCIS
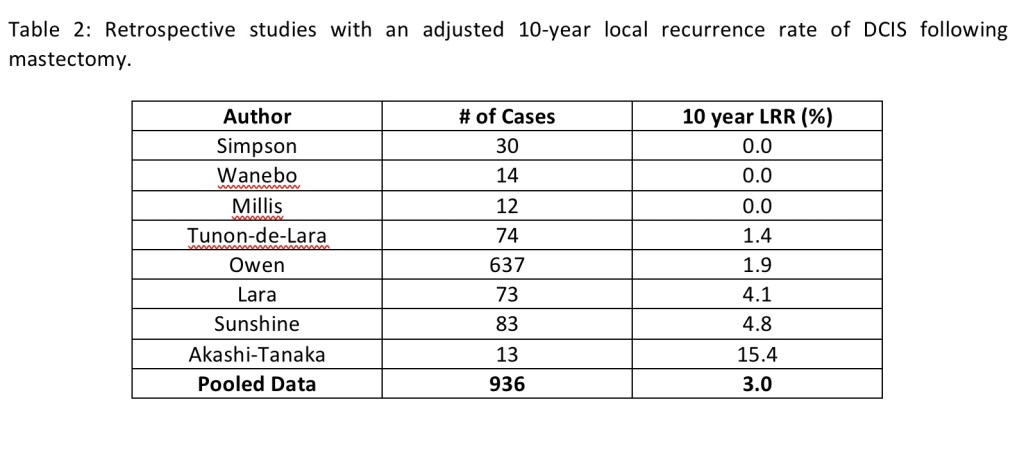
A meta-analysis of eight retrospective studies:
Demonstrated an adjusted 10-year local recurrence rate of:
2.6% (95% confidence interval [CI] 0.8 to 4.5%) after mastectomy:
Confirming the very low recurrence rate for DCIS treated with mastectomy
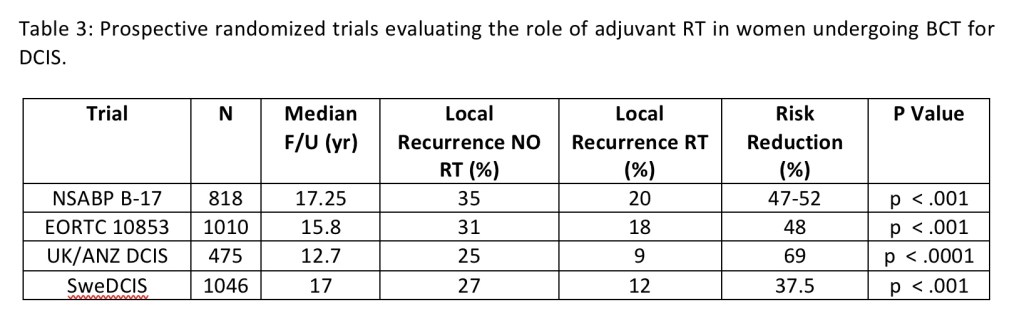
Table 3: Prospective randomized trials evaluating the role of adjuvant RT in women undergoing BCT for DCIS.
In the last decade in the USA the use of contralateral prophylactic mastectomy (CPM) in women with unilateral breast cancer has substantially increased, specially in women with DCIS:
The risk of developing a contralateral breast cancer in women with DCIS:
Is approximately 0.8% per year
In spite of the fact that the risk of contralateral breast cancer in DCIS is lower than the risk of ipsilateral recurrence:
The cumulative risk of contralateral breast cancer may be clinically relevant:
Because women with DCIS have very low risk of breast cancer mortality from their DCIS
Randomized clinical trials:
Proved that BCS was equivalent to mastectomy in women with invasive cancer:
This conservative approach has been expanded to include DCIS
There are no randomized prospective trials comparing recurrence rates or overall survival (OS):
Between mastectomy and BCS for DCIS
Silverstein et al, in a retrospective study, comparing 227 patients with DCIS treated with mastectomy or BCS (with or without RT):
Showed that the 7-year disease-free survival (DFS):
Was 98% for mastectomy and 84% for BCS:
With no difference in OS
The role of adjuvant RT in women undergoing BCS for DCIS have been studied in four prospective randomized trials:
Only patients not taking tamoxifen and randomized to radiation or not are included in these four trials
The NSABP B-17 was the first phase III randomized study:
That compared lumpectomy alone to lumpectomy plus breast radiation:
In 818 patients with localized DCIS
In the BCS only group (N=391):
The event free survival was:
73.8%
In the BCS plus RT group (N=399):
The event free survival:
84.4%
In the BCS only group (N=391):
The local recurrence rate was:
35%
In the BCS plus RT group (N=399):
Local recurrence rate was:
20%
The trial concluded that:
RT significantly decreases the rate of invasive cancer and DCIS in the ipsilateral breast:
By approximately 50%
In a recent update of the NSABP B-17 with 15 year follow-up:
The invasive ipsilateral breast tumor recurrence (I-IBTR) for the BCS only group was:
19.4% compared to the BCS plus RT group of 8.9%
They also found that there is an increase rate of breast cancer related mortality with I-IBTR but not with DCIS
The Swedish breast cancer cooperative group (BCCG):
Accrued 1046 patients between 1987 and 1999 with a mean follow-up of eight years
Inclusion criteria included:
A clinically negative axilla
Localized DCIS to less than one quadrant of the breast
In the BCS only group (N=520):
The local recurrence rate was 27%
In the BCS plus RT group (N=526):
Local recurrence rate was 12%
The study identified that there was an increasing effect of RT with age:
With patients under 50 years:
Having a 6% absolute reduction of local recurrence with RT
Patients older that 65 years:
18% absolute reduction of local recurrence with RT
The European Organization for Research and Treatment of Cancer (EORTC) 10853:
Accrued 1010 patients between 1986 and 1996
Inclusion criteria included:
Patients younger that 70 years
Completely excised DCIS measuring equal or less than 5 cm
In the BCS only group (N=503):
The local recurrence rate was 31%
In the BCS plus RT group (N=507):
Local recurrence rate was 18%
The EORTC 10853 found similar findings to the NSABP B-17 study in that:
I-IBTR was associated with a decrease in breast cancer specific survival (BCSS) but not with DCIS
The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG):
Carried out an individual patient-level meta-analysis of these four randomized controlled trials:
Which included 3,729 women
The use of RT after BCS:
Decreased the risk of recurrence by approximately 50% (hazard ratio [HR] 0.49; 95% CI 0.41 to 0.58; p < .00001)
Equivalent to an absolute 10-year reduction in the risk of any ipsilateral breast recurrence of 15.2%:
28.1% [no RT] versus 12.9% [RT]; p < .00001
In the EBCTCG study:
The number needed to treat with RT was nine women to prevent one ipsilateral breast recurrence
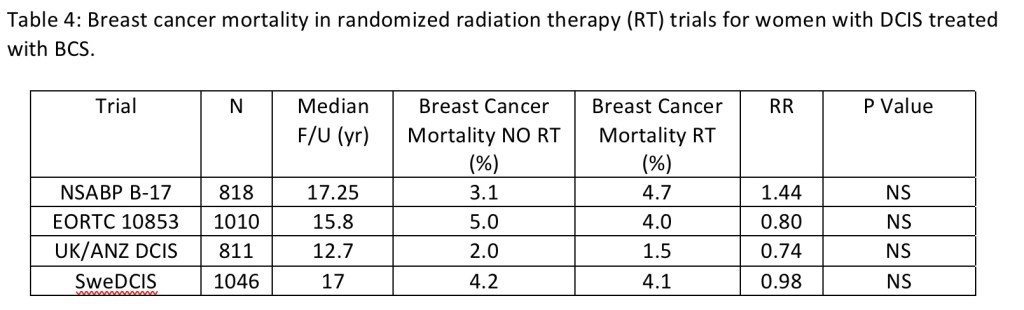
After 10 years of follow-up, there was no notable effect on breast cancer mortality:
Mortality from causes other than breast cancer, or all-cause mortality
In all subgroup of patient, including those with small, low-grade tumors and negative margins:
RT decreased the risk of an ipsilateral breast event by approximately 50%
Hence, though RT clearly reduces local recurrence rates for women undergoing BCS for DCIS:
It does not improve survival
In view of the fact that breast RT has rare but potentially serious side effects (RT-induced malignancy and cardiovascular disease):
Its risks should be weighed against the decrease in local recurrence when making treatment recommendations for patients with DCIS
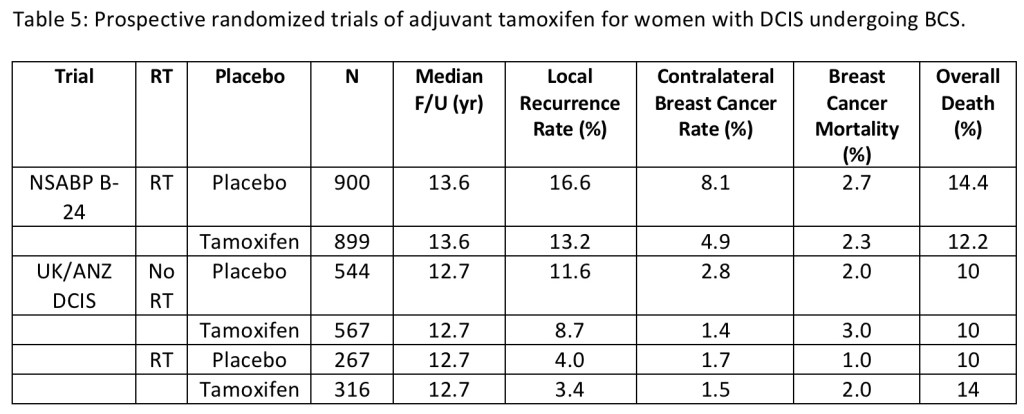
Two randomized clinical trials have assessed the role of tamoxifen in preventing recurrence:
The NSABP B-24:
Was a double-blind prospective trial of adjuvant tamoxifen (20 mg/day) versus placebo for five-years:
In 1,804 women undergoing BCS and adjuvant RT
This studied accrued patients between 1991 and 1994
Roughly 25% had positive or uncertain margins
80% had lesions measuring 1 cm or less
The 15-year cumulative incidence of recurrence was reduced from:
18.3% to 16.0% with the addition of tamoxifen:
With a reduction in invasive recurrence from 10% to 8.5%
The inclusion of tamoxifen also had a chemopreventive effect on the contralateral breast:
With the 15-year cumulative incidence of all contralateral breast cancers (CBC):
Reduced from 10.8% to 7.3%
The use of tamoxifen did not improve overall survival (OS)
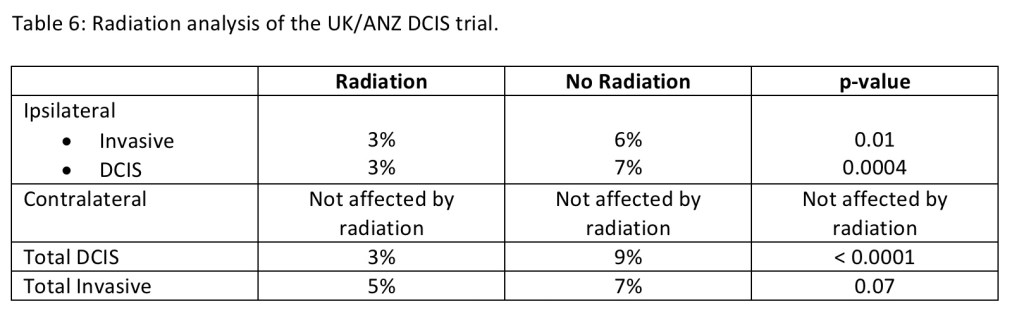
A 2 × 2 factorial randomized trial of both RT and tamoxifen by the United Kingdom, Australia, and New Zealand (UK/ANZ) DCIS group accrued patients between 1990 to 1998
The study allowed women to participate in either of the randomization arms
A total of 1,576 women participated in the tamoxifen randomization:
Of whom 1,053 did not receive RT and 523 did
The use of tamoxifen decreased the incidence of ipsilateral DCIS recurrence (HR 0.70; 95% CI 0.51 to 0.86; p = .03):
But had no effect on ipsilateral invasive disease (HR 0.95; 95% CI 0.66 to 1.38; p = .8)
The ipsilateral benefit of tamoxifen was limited to those not receiving RT (HR for ipsilateral breast events 0.77; 95% CI 0.59 to 0.98; p = .04) and was not significant in those receiving RT
The radiation analysis of the study is shown in table 6
The chemopreventive effect of hormonal therapy was shown with a decrease in the incidence of any CBC events (HR 0.44; 95% CI 0.25 to 0.77; p = .005)
As with the NSABP B-24, tamoxifen resulted in no survival advantage
Patients were enrolled in the NSABP B-24 and UK/ANZ trials without knowledge of hormone receptor status
Allred et el tested a subset of 732 cases (41%) from NSABP B-24 for estrogen receptors:
They identified that the benefit of tamoxifen was limited to the ER-positive group
In the non-randomized Eastern Oncology Cooperative Group and Cancer Therapy and the American College of Radiology Imaging Network (ECOG ACRIN) E5194 trial:
Women with DCIS with low-risk clinical and pathologic characteristics were assigned to two cohorts between April 1997 and October 2002:
Cohort one (n = 561) had low- (50%) or intermediate-grade (50%) DCIS and a tumor size ≤ 2.5 cm
Cohort two (n = 104) had high-grade DCIS and a tumor size ≤ 1 cm
Enrollment and cohort assignment were based on clinical and pathology assessment at treating institutions
All patients underwent surgical excision (lumpectomy) of the primary DCIS tumor and received no radiation therapy
Lumpectomy was to have a minimum negative margin width of ≥ 3 mm or no tumor on re-excision
The primary endpoint of the study was the development of a ipsilateral breast event, defined as the first local recurrence of DCIS or invasive carcinoma in the treated breast
Tamoxifen was not randomly assigned
The median follow-up of the trial was 12.3 years
A total of 99 ipsilateral breast events were observed (74 in cohort 1 and 25 in cohort 2), including 51 invasive ipsilateral breast events (52%; 39 in cohort 1 and 12 in cohort 2)
Overall the IBTR rate:
In the low to intermediate grade DCIS group was 14.4% compared to the high grade DCIS group which was 26.4% (p=0.003, HR 1.84)
The I-IBTR rate:
In the low to intermediate grade DCIS group was 7.5% compared to the high grade DCIS group which was 13.4% (p=0.08)
The risks of developing an ipsilateral breast event and an invasive event increased over time through 12 years, with no plateau observed
In group one, the rates of developing an ipsilateral breast event and an invasive ipsilateral breast event:
Were approximately 1.2% and 0.6% per year through year the 12 years
At 12 years, overall survival was 84.0% and 82.8% (p=0.96) and the incidence of contralateral breast cancer events was 6.7% and 12.0% (p=0.16)
On multivariable analysis, study cohort (hazard ratio [HR] = 1.84, P = .009, for cohort 2 vs 1) and tumor size (HR = 2.11, P = .03, for > 10 mm vs ≤ 5 mm) were significantly associated with the development of an ipsilateral breast event
On multivariable analysis for invasive ipsilateral breast event, cohort was of borderline significance (p=0.08)
The conclusion of the E5194 trial was that for patients with DCIS of the breast who had favorable clinical and pathologic factors and were managed with surgical excision alone (without radiation):
The study demonstrated that the risks of developing an ipsilateral breast event and an invasive ipsilateral breast event increased over time through 12 years of follow-up, without plateau
Individual patients and their physicians will need to decide if these 12-year risks are acceptable, and to judge whether or not to add adjuvant treatment after surgical excision
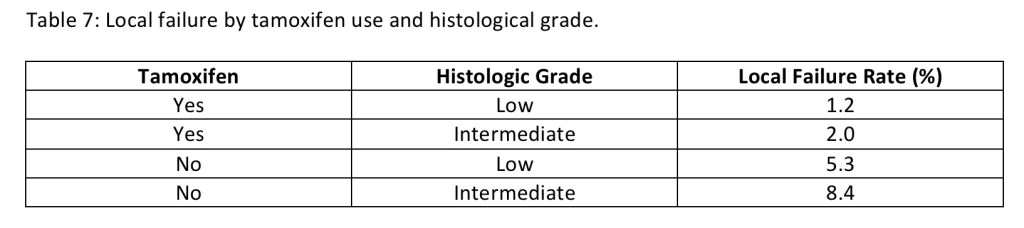
The Radiation Therapy and Oncology Group (RTOG) 9804 trial:
Was a prospective randomized trial that accrued 636 patients from 1998 to 2006 with mammographically detected low-grade or intermediate-grade DCIS, measuring less than 2.5 cmwith margins ≥ 3 mm:
Compared RT (with or without tamoxifen) with observation (with or without tamoxifen) after surgery
The trial was designed for 1,790 patients but was closed early because of lower than projected accrual
Ipsilateral local failure (LF) was the primary end point
Tamoxifen was optional if started within four weeks of DCIS diagnosis (62% of the patients did receive tamoxifen)
Table 7 demonstrates the LF rate based on histologic grade and tamoxifen use
With a median follow-up time was 7.17 years:
Two LFs occurred in the RT arm (with or without tamoxifen), and 19 LFs occurred in the observation arm (with or without tamoxifen)
At seven years, the LF rate was 0.9% (95% CI, 0.0% to 2.2%) in the RT arm (with or without tamoxifen) compared to 6.7% (95% CI, 3.2% to 9.6%) in the observation arm (with or without tamoxifen) (hazard ratio, 0.11; 95% CI, 0.03 to 0.47; P < .001)
The conclusion of the trial:
Said that the good-risk subset of patients with DCIS, the LF rate was low with observation but was decreased significantly with the addition of RT
The differences in the rates of local recurrence, in the patients who did not receive RT, between the NSABP B-24 (20.9%) and the RTOG 9804 (6.7%):
Can be attributed to the fact that the B-24 trial did not separate patients in low-, intermediate-, or high-grade groups
The differences in recurrence rate between the ECOG ACRIN E5194 (10.5%) and the RTOG 9804 (6.7%) trials in the low risk groups:
May be secondary to the higher proportion of patients who took tamoxifen in the RTOG 9804 trial
Two trials, the NSABP B-35 and International Breast Cancer Intervention Studies (IBIS)-II:
Compared anastrozole (an aromatase inhibitor proven superior to tamoxifen for invasive cancer) with tamoxifen in hormone receptor–positive DCIS managed with local excision
Both studies were randomized and double-blinded
The NSABP B-35:
Was a phase III clinical trial that randomized postmenopausal women with ER-positive DCIS to five years of anastrozole or tamoxifen following BCS and whole breast RT
The trial sought to determine how effective anastrozole is compared to tamoxifen in preventing a breast cancer recurrences, as well as the quality of life of patients taking anastrozole
It accrued 3104 women between 2003 to 2006 with nine years of follow up
The inclusion criteria included postmenopausal women with estrogen and progesterone receptor (ER / PR) positive DCIS and / or LCIS, that were excised with negative margins
Investigators found significantly fewer breast cancer events in the anastrozole group (n = 90) compared to the tamoxifen group (n = 122) (HR, 0.73; confidence interval, 0.56–0.96, P=0.0234)
The estimated 10-year breast-cancer-free interval rates were:
93.5% for the anastrozole group compared to 89.2% for the tamoxifen group:
This recorded difference in breast cancer-free interval:
Was attributable almost entirely to younger postmenopausal women less than 60 years of age
Interestingly the difference between treatments did not become apparent until after five years of follow-up:
Likely due to the low number of events in both group
There was no difference in OS between the two treatment groups
The IBIS-II:
Accrued 2980 women between 2003 to 2013 from 238 centers in 17 countries with a follow-up of seven years
The study randomized postmenopausal women with ER positive DCIS (micro-invasion was permitted), negative surgical margins, and adjuvant RT according to local practices (70% of patients received RT) to lumpectomy plus anastrazole to lumpectomy plus tamoxifen
The incidence of any breast cancer event was low in both groups (5%):
Anastrozole was non-inferior to tamoxifen
DCIS is a non-invasive entity:
Lymph node involvement is not expected to occur
If a patient presents with DCIS in the breast but is found to have malignant cells in the lymph nodes preoperatively:
The patient has, by definition, invasive breast cancer and not DCIS
In situations where patients have large tumors (greater than 4 cm) or extensive micro-calcifications:
A focus of invasion can be missed because of limited pathologic sampling:
There is roughly a 20% to 30% rate of associated invasive disease:
Reported on final pathology in patients who were diagnosed with DCIS on stereotactic biopsy
This patients, as well as those with high-grade or palpable disease:
Are at higher risk for lymph node involvement and may also warrant sentinel lymph node (SLN) mapping:
Particularly if they are undergoing mastectomy or if BCS is to be followed by oncoplastic surgery
The risk of not identifying metastatic disease in the lymph nodes must be weighed against the risk of lymphedema associated with SLN dissection in each patient
Cox et al, in 1998:
Reported a positive SLN biopsy rate of 6% in patients with DCIS when a combination of hematoxylin–eosin staining and immunohistochemistry was utilized
Another study by Klauber-DeMore et al. (2000):
Identified a positive SLN biopsy rate of 12% in patients with DCIS considered to be at high risk for invasion and among 10% of patients who had DCIS with micro-invasion
Invasive carcinoma is identified when DCIS is diagnosed by core needle biopsy of a tumor mass:
In 25% of the cases compared to 13% of the cases when the biopsy is performed for micro-calcifications
The incidence of identifying a positive SLN:
Is more frequent in large areas of DCIS:
Odds ratio of 1.14 per 1 cm increase in size
When comedo necrosis is present:
Up to 40% of the cases
When the DCIS is high nuclear grade:
23% vs 7% low-intermediate grade
When estrogen receptors (ER) / progesterone receptors (PR) are negative:
33% vs 11% for ER / PR positive disease
A study from the MD Anderson Cancer Center (MDACC), (Francis et al. (2015)):
Investigated the incidence of positive lymph nodes and the clinical significance of these findings in 1,234 patients with an initial diagnosis of DCIS planned for SLN dissection:
The positive SLN biopsy rate was 10.7% (positive SLNs in 132 patients):
The results included isolated tumor cells in 66 (5.4%) patients, micro-metastases in 36 (2.9%) and macro-metastases in 30 (2.4%)
There was upstaging in the primary tumor in 26.5% of the cases (327 patients) to micro-invasion or invasive cancer
Factors predictive of a positive SLN were:
Diagnosis by excisional biopsy
Papillary histology
DCIS greater than 2 cm
More than three interventions prior to SLN dissection (needle biopsy, excisional biopsy, etc.)
Micro-invasion or invasive cancer
It was noted that with increasing numbers of preoperative interventions (biopsy, needle localization, etc.):
There was a higher likelihood of positive SLN findings:
With the majority being isolated tumor cells (44/907, 4.2%) or micro-metastases (12/907, 1.3%)
There were no macro-metastases identified in the SLNs of patients with pure DCIS
The high incidence of isolated tumor cells in the SLNs with increasing preoperative interventions supports the concept of benign mechanical transport of epithelial cells during manipulation of the primary tumor
At a median follow-up of 61.7 months:
There was no difference in disease-free survival (DFS) outcomes in the patients with pure DCIS with or without positive SLN findings
In general terms, SLN dissection should be limited to patients who undergo mastectomy for:
Large, high-grade DCIS because it is difficult to perform lymphatic mapping after a mastectomy if invasive cancer is found in the mastectomy specimen
The 2017 ASCO guidelines do not recommend SLN biopsy for BCS for DCIS:
But for large, high-grade DCIS with necrosis one can discuss with the patient the option of performing the SLN biopsy during BCS
Though recognized as a distinct entity for many years:
This common histologic subtype did not garner widespread acceptance into the cytopathologic nomenclature:
Until it was described in a case series by Chem and Rosai in 1977
Characterized by its follicular architectural pattern:
The nuclear changes are variably present throughout the tumor
Follicular variant papillary thyroid cancer demonstrates a follicular growth pattern:
But cytologically the tumors display the typical features of common-type papillary thyroid cancers, including:
Large, overlapping nuclei with hypodense chromatin
Nuclear pseudoinclusions, and nuclear grooves
Most also contain psammoma bodies
Fine-needle aspirate of a papillary thyroid carcinoma of the thyroid showing a psammoma body. The concentric, laminations can best be appreciated under the microscope by moving the depth of focus.
Of the several histologic subtypes of papillary thyroid carcinoma:
The follicular variants are probably the most common
The incidence of follicular variant papillary cancer has been increasing:
While that of the classical form has been decreasing
In a single-center study:
Nearly 40% of the papillary thyroid cancers were follicular variants
In a multicenter study:
23% of papillary thyroid cancers were:
The noninvasive, well-circumscribed subtype:
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features, NIFTP
According to the 2017 World Health Organization classification of endocrine tumors:
Follicular variants of papillary thyroid cancer are subtyped as being either infiltrative or encapsulated with invasion:
Infiltrative:
The infiltrative subtype demonstrates invasive tongues of tumor infiltrating into non-neoplastic thyroid parenchyma and lacks a well-defined tumor capsule
The infiltrative subtype has a biological behavior and molecular profile that is more similar to classic papillary thyroid cancer than follicular cancers
The infiltrative subtype is more likely to have lymph node metastases and BRAF V600E mutations
While being less likely than follicular thyroid cancers to have distant metastases or RAS mutations
Encapsulated with invasion:
The encapsulated with invasion subtype demonstrates both a well-defined tumor capsule and either invasion of the tumor capsule or invasion into vesselswithin or beyond the tumor capsule
The encapsulated variants, particularly those with vascular invasion, have a tumor biology (often RAS mutation) and biological behavior (more likely to have distant metastases, less likely to have lymph node metastases) that is more similar to follicular thyroid cancer than to classical papillary thyroid cancer
It is the presence of either vascular or tumor capsular invasion that differentiates an encapsulated follicular variant of papillary thyroid cancer (capsular and/or vascular invasion present) from noninvasive encapsulated follicular variant of papillary thyroid cancer (NIFTP; no capsular or vascular invasion present)
In the past, encapsulated follicular variant of papillary thyroid cancer without evidence for either vascular or tumor capsule invasion were considered noninvasive variants of papillary thyroid cancer
However, noninvasive encapsulated follicular variants of papillary thyroid cancer have a very low malignant potential and are uniformly cured with lobectomy
Because of the very low malignant potential, this type was renamed noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), emphasizing that this tumor can be managed as a neoplasm rather than a malignancy
Both the American Thyroid Association and the World Health Organization have endorsed this change in nomenclature
While thyroid surgery is required to distinguish NIFTP from the encapsulated with invasive subtype, therapy beyond thyroid lobectomy is usually not required (ie, thyroid-stimulating hormone [TSH] suppression and radioactive iodine ablation is not required)
Proper use of the NIFTP nomenclature requires adherence to strict histopathological criteria, which means that tumors previously classified as noninvasive encapsulated follicular variant of papillary thyroid cancer cannot be assumed to be NIFTP tumors
Because the entire tumor capsule may not have been sampled or preserved at the time of initial diagnosis, it is often not possible to determine if an archived tumor sample meets all the diagnostic criteria to be reclassified as an NIFTP tumor
The diagnosis of classic PTC requires nuclear features including:
Intranuclear inclusions and nuclear grooves
The nuclei are larger than usual and often overlap:
Some may appear empty and are often called “Orphan Annie eyes“
The nuclear features of PTC distinguish it from other tumors:
Enabling it to be diagnosed on fine-needle aspiration
In addition, the tumor architecture is characterized by:
Branching papillae with a central fibrovascular stalk
Psammoma bodies, or “ghosts” of infarcted papillae:
Are virtually pathognomonic of PTC:
These concentric, lamellated, calcified spheres may be seen in approximately 50% of cases
Classical PTC is typically unencapsulated with invasive and ill-defined margins:
Nevertheless, this common histologic type is generally associated with an excellent prognosis
Surgical specimen showing the classic histologic appearance of papillary thyroid cancer with papillary structure (branching papillae) and no follicles or colloid. Follicular development can be seen in some of these carcinomas (follicular variant of papillary thyroid cancer); in them, the diagnosis is made from the cytologic features of the cells.FNA of a thyroid nodule showing papillary thyroid cancer. The cells and nuclei are large, and their cytoplasm has a “ground glass” appearance. Nucleoli are prominent, and the nuclei have clefts, grooves, and “holes” due to intranuclear cytoplasmic inclusions (“Orphan Annie eyes”).