- The treatment options for DCIS are many including:
- Breast conserving surgery (BCS):
- With or with out radiation
- Unilateral mastectomy
- Bilateral mastectomy
- Endocrine therapy
- All have an excellent overall survival (OS)
- Breast conserving surgery (BCS):
- Treatment Options:
- Breast Conserving Surgery (BCS):
- Wide excision alone
- Wide excision with radiation (RT)
- Wide excision with endocrine therapy
- Wide excision with RT and endocrine therapy
- Unilateral mastectomy
- Bilateral mastectomy
- Breast Conserving Surgery (BCS):
- Mastectomy:
- Was considered to be the standard of care in the surgical management for all breast cancers, including:
- DCIS
- A meta-analysis of eight retrospective studies:
- Demonstrated an adjusted 10-year local recurrence rate of:
- 2.6% (95% confidence interval [CI] 0.8 to 4.5%) after mastectomy:
- Confirming the very low recurrence rate for DCIS treated with mastectomy
- 2.6% (95% confidence interval [CI] 0.8 to 4.5%) after mastectomy:
- Demonstrated an adjusted 10-year local recurrence rate of:
- Was considered to be the standard of care in the surgical management for all breast cancers, including:
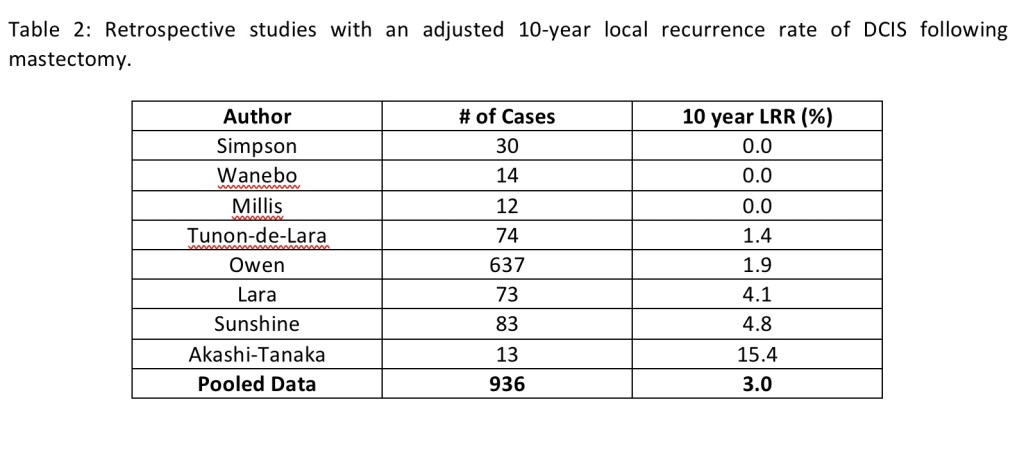
Table 3: Prospective randomized trials evaluating the role of adjuvant RT in women undergoing BCT for DCIS.
- In the last decade in the USA the use of contralateral prophylactic mastectomy (CPM) in women with unilateral breast cancer has substantially increased, specially in women with DCIS:
- The risk of developing a contralateral breast cancer in women with DCIS:
- Is approximately 0.8% per year
- In spite of the fact that the risk of contralateral breast cancer in DCIS is lower than the risk of ipsilateral recurrence:
- The cumulative risk of contralateral breast cancer may be clinically relevant:
- Because women with DCIS have very low risk of breast cancer mortality from their DCIS
- The cumulative risk of contralateral breast cancer may be clinically relevant:
- The risk of developing a contralateral breast cancer in women with DCIS:
- Randomized clinical trials:
- Proved that BCS was equivalent to mastectomy in women with invasive cancer:
- This conservative approach has been expanded to include DCIS
- There are no randomized prospective trials comparing recurrence rates or overall survival (OS):
- Between mastectomy and BCS for DCIS
- Proved that BCS was equivalent to mastectomy in women with invasive cancer:
- Silverstein et al, in a retrospective study, comparing 227 patients with DCIS treated with mastectomy or BCS (with or without RT):
- Showed that the 7-year disease-free survival (DFS):
- Was 98% for mastectomy and 84% for BCS:
- With no difference in OS
- Was 98% for mastectomy and 84% for BCS:
- Showed that the 7-year disease-free survival (DFS):
- The role of adjuvant RT in women undergoing BCS for DCIS have been studied in four prospective randomized trials:
- Only patients not taking tamoxifen and randomized to radiation or not are included in these four trials
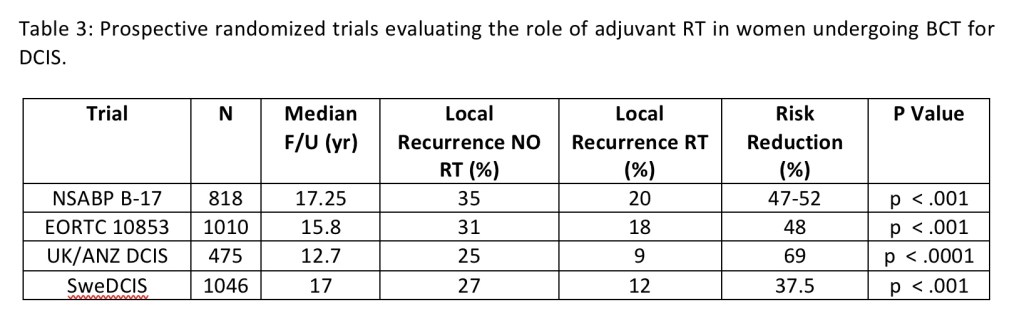
- The NSABP B-17 was the first phase III randomized study:
- That compared lumpectomy alone to lumpectomy plus breast radiation:
- In 818 patients with localized DCIS
- That compared lumpectomy alone to lumpectomy plus breast radiation:
- In the BCS only group (N=391):
- The event free survival was:
- 73.8%
- The event free survival was:
- In the BCS plus RT group (N=399):
- The event free survival:
- 84.4%
- The event free survival:
- In the BCS only group (N=391):
- The local recurrence rate was:
- 35%
- The local recurrence rate was:
- In the BCS plus RT group (N=399):
- Local recurrence rate was:
- 20%
- Local recurrence rate was:
- The trial concluded that:
- RT significantly decreases the rate of invasive cancer and DCIS in the ipsilateral breast:
- By approximately 50%
- RT significantly decreases the rate of invasive cancer and DCIS in the ipsilateral breast:
- In a recent update of the NSABP B-17 with 15 year follow-up:
- The invasive ipsilateral breast tumor recurrence (I-IBTR) for the BCS only group was:
- 19.4% compared to the BCS plus RT group of 8.9%
- They also found that there is an increase rate of breast cancer related mortality with I-IBTR but not with DCIS
- The invasive ipsilateral breast tumor recurrence (I-IBTR) for the BCS only group was:
- The Swedish breast cancer cooperative group (BCCG):
- Accrued 1046 patients between 1987 and 1999 with a mean follow-up of eight years
- Inclusion criteria included:
- A clinically negative axilla
- Localized DCIS to less than one quadrant of the breast
- In the BCS only group (N=520):
- The local recurrence rate was 27%
- In the BCS plus RT group (N=526):
- Local recurrence rate was 12%
- The study identified that there was an increasing effect of RT with age:
- With patients under 50 years:
- Having a 6% absolute reduction of local recurrence with RT
- Patients older that 65 years:
- 18% absolute reduction of local recurrence with RT
- With patients under 50 years:
- The European Organization for Research and Treatment of Cancer (EORTC) 10853:
- Accrued 1010 patients between 1986 and 1996
- Inclusion criteria included:
- Patients younger that 70 years
- Completely excised DCIS measuring equal or less than 5 cm
- In the BCS only group (N=503):
- The local recurrence rate was 31%
- In the BCS plus RT group (N=507):
- Local recurrence rate was 18%
- The EORTC 10853 found similar findings to the NSABP B-17 study in that:
- I-IBTR was associated with a decrease in breast cancer specific survival (BCSS) but not with DCIS
- The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG):
- Carried out an individual patient-level meta-analysis of these four randomized controlled trials:
- Which included 3,729 women
- The use of RT after BCS:
- Decreased the risk of recurrence by approximately 50% (hazard ratio [HR] 0.49; 95% CI 0.41 to 0.58; p < .00001)
- Equivalent to an absolute 10-year reduction in the risk of any ipsilateral breast recurrence of 15.2%:
- 28.1% [no RT] versus 12.9% [RT]; p < .00001
- In the EBCTCG study:
- The number needed to treat with RT was nine women to prevent one ipsilateral breast recurrence
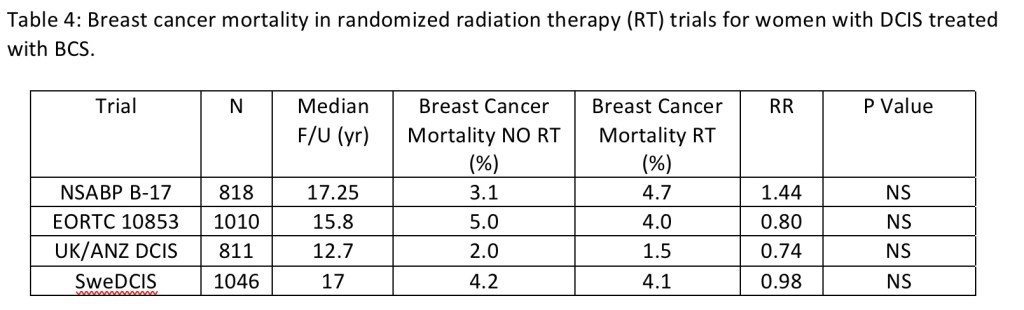
- After 10 years of follow-up, there was no notable effect on breast cancer mortality:
- Mortality from causes other than breast cancer, or all-cause mortality
- In all subgroup of patient, including those with small, low-grade tumors and negative margins:
- RT decreased the risk of an ipsilateral breast event by approximately 50%
- Hence, though RT clearly reduces local recurrence rates for women undergoing BCS for DCIS:
- It does not improve survival
- In view of the fact that breast RT has rare but potentially serious side effects (RT-induced malignancy and cardiovascular disease):
- Its risks should be weighed against the decrease in local recurrence when making treatment recommendations for patients with DCIS
- Carried out an individual patient-level meta-analysis of these four randomized controlled trials:
- Two randomized clinical trials have assessed the role of tamoxifen in preventing recurrence:
- The NSABP B-24:
- Was a double-blind prospective trial of adjuvant tamoxifen (20 mg/day) versus placebo for five-years:
- In 1,804 women undergoing BCS and adjuvant RT
- This studied accrued patients between 1991 and 1994
- Roughly 25% had positive or uncertain margins
- 80% had lesions measuring 1 cm or less
- The 15-year cumulative incidence of recurrence was reduced from:
- 18.3% to 16.0% with the addition of tamoxifen:
- With a reduction in invasive recurrence from 10% to 8.5%
- 18.3% to 16.0% with the addition of tamoxifen:
- The inclusion of tamoxifen also had a chemopreventive effect on the contralateral breast:
- With the 15-year cumulative incidence of all contralateral breast cancers (CBC):
- Reduced from 10.8% to 7.3%
- With the 15-year cumulative incidence of all contralateral breast cancers (CBC):
- The use of tamoxifen did not improve overall survival (OS)
- Was a double-blind prospective trial of adjuvant tamoxifen (20 mg/day) versus placebo for five-years:
- The NSABP B-24:
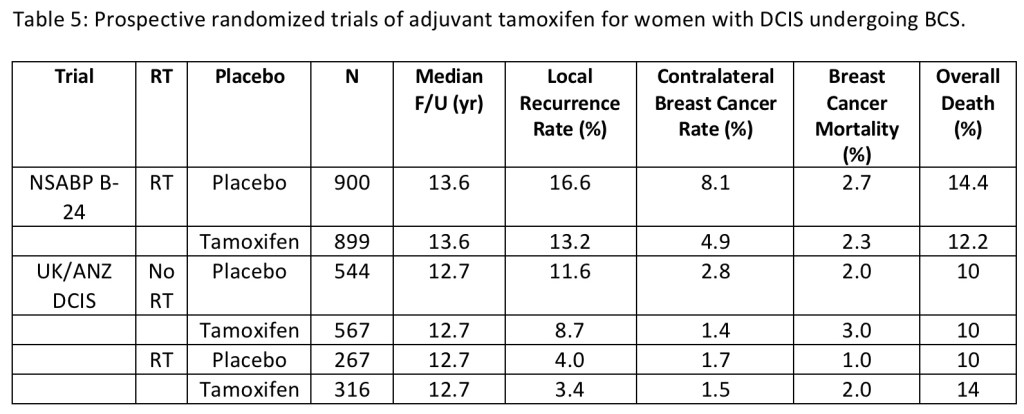
- A 2 × 2 factorial randomized trial of both RT and tamoxifen by the United Kingdom, Australia, and New Zealand (UK/ANZ) DCIS group accrued patients between 1990 to 1998
- The study allowed women to participate in either of the randomization arms
- A total of 1,576 women participated in the tamoxifen randomization:
- Of whom 1,053 did not receive RT and 523 did
- The use of tamoxifen decreased the incidence of ipsilateral DCIS recurrence (HR 0.70; 95% CI 0.51 to 0.86; p = .03):
- But had no effect on ipsilateral invasive disease (HR 0.95; 95% CI 0.66 to 1.38; p = .8)
- The ipsilateral benefit of tamoxifen was limited to those not receiving RT (HR for ipsilateral breast events 0.77; 95% CI 0.59 to 0.98; p = .04) and was not significant in those receiving RT
- The radiation analysis of the study is shown in table 6
- The chemopreventive effect of hormonal therapy was shown with a decrease in the incidence of any CBC events (HR 0.44; 95% CI 0.25 to 0.77; p = .005)
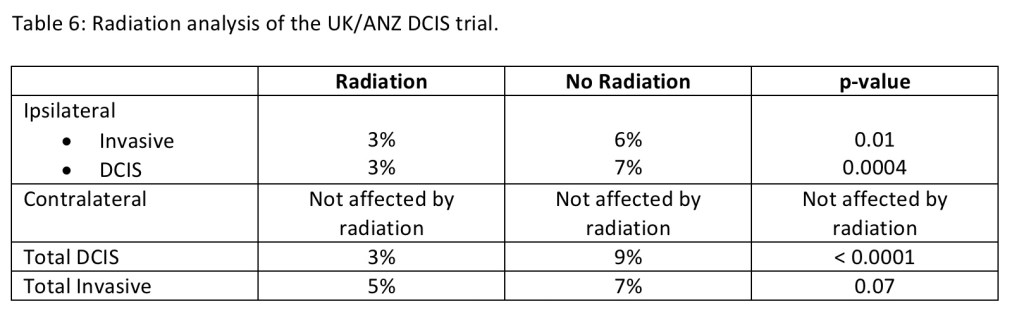
- As with the NSABP B-24, tamoxifen resulted in no survival advantage
- Patients were enrolled in the NSABP B-24 and UK/ANZ trials without knowledge of hormone receptor status
- Allred et el tested a subset of 732 cases (41%) from NSABP B-24 for estrogen receptors:
- They identified that the benefit of tamoxifen was limited to the ER-positive group
- In the non-randomized Eastern Oncology Cooperative Group and Cancer Therapy and the American College of Radiology Imaging Network (ECOG ACRIN) E5194 trial:
- Women with DCIS with low-risk clinical and pathologic characteristics were assigned to two cohorts between April 1997 and October 2002:
- Cohort one (n = 561) had low- (50%) or intermediate-grade (50%) DCIS and a tumor size ≤ 2.5 cm
- Cohort two (n = 104) had high-grade DCIS and a tumor size ≤ 1 cm
- Enrollment and cohort assignment were based on clinical and pathology assessment at treating institutions
- All patients underwent surgical excision (lumpectomy) of the primary DCIS tumor and received no radiation therapy
- Lumpectomy was to have a minimum negative margin width of ≥ 3 mm or no tumor on re-excision
- The primary endpoint of the study was the development of a ipsilateral breast event, defined as the first local recurrence of DCIS or invasive carcinoma in the treated breast
- Tamoxifen was not randomly assigned
- The median follow-up of the trial was 12.3 years
- A total of 99 ipsilateral breast events were observed (74 in cohort 1 and 25 in cohort 2), including 51 invasive ipsilateral breast events (52%; 39 in cohort 1 and 12 in cohort 2)
- Overall the IBTR rate:
- In the low to intermediate grade DCIS group was 14.4% compared to the high grade DCIS group which was 26.4% (p=0.003, HR 1.84)
- The I-IBTR rate:
- In the low to intermediate grade DCIS group was 7.5% compared to the high grade DCIS group which was 13.4% (p=0.08)
- The risks of developing an ipsilateral breast event and an invasive event increased over time through 12 years, with no plateau observed
- In group one, the rates of developing an ipsilateral breast event and an invasive ipsilateral breast event:
- Were approximately 1.2% and 0.6% per year through year the 12 years
- At 12 years, overall survival was 84.0% and 82.8% (p=0.96) and the incidence of contralateral breast cancer events was 6.7% and 12.0% (p=0.16)
- On multivariable analysis, study cohort (hazard ratio [HR] = 1.84, P = .009, for cohort 2 vs 1) and tumor size (HR = 2.11, P = .03, for > 10 mm vs ≤ 5 mm) were significantly associated with the development of an ipsilateral breast event
- On multivariable analysis for invasive ipsilateral breast event, cohort was of borderline significance (p=0.08)
- The conclusion of the E5194 trial was that for patients with DCIS of the breast who had favorable clinical and pathologic factors and were managed with surgical excision alone (without radiation):
- The study demonstrated that the risks of developing an ipsilateral breast event and an invasive ipsilateral breast event increased over time through 12 years of follow-up, without plateau
- Individual patients and their physicians will need to decide if these 12-year risks are acceptable, and to judge whether or not to add adjuvant treatment after surgical excision
- Women with DCIS with low-risk clinical and pathologic characteristics were assigned to two cohorts between April 1997 and October 2002:
- The Radiation Therapy and Oncology Group (RTOG) 9804 trial:
- Was a prospective randomized trial that accrued 636 patients from 1998 to 2006 with mammographically detected low-grade or intermediate-grade DCIS, measuring less than 2.5 cm with margins ≥ 3 mm:
- Compared RT (with or without tamoxifen) with observation (with or without tamoxifen) after surgery
- The trial was designed for 1,790 patients but was closed early because of lower than projected accrual
- Ipsilateral local failure (LF) was the primary end point
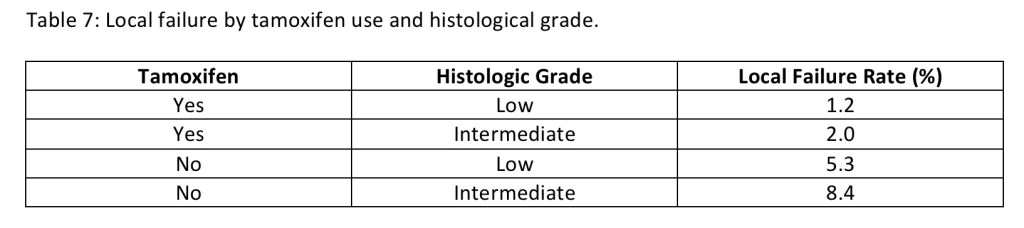
- Tamoxifen was optional if started within four weeks of DCIS diagnosis (62% of the patients did receive tamoxifen)
- Table 7 demonstrates the LF rate based on histologic grade and tamoxifen use
- With a median follow-up time was 7.17 years:
- Two LFs occurred in the RT arm (with or without tamoxifen), and 19 LFs occurred in the observation arm (with or without tamoxifen)
- At seven years, the LF rate was 0.9% (95% CI, 0.0% to 2.2%) in the RT arm (with or without tamoxifen) compared to 6.7% (95% CI, 3.2% to 9.6%) in the observation arm (with or without tamoxifen) (hazard ratio, 0.11; 95% CI, 0.03 to 0.47; P < .001)
- The conclusion of the trial:
- Said that the good-risk subset of patients with DCIS, the LF rate was low with observation but was decreased significantly with the addition of RT
- Was a prospective randomized trial that accrued 636 patients from 1998 to 2006 with mammographically detected low-grade or intermediate-grade DCIS, measuring less than 2.5 cm with margins ≥ 3 mm:
- The differences in the rates of local recurrence, in the patients who did not receive RT, between the NSABP B-24 (20.9%) and the RTOG 9804 (6.7%):
- Can be attributed to the fact that the B-24 trial did not separate patients in low-, intermediate-, or high-grade groups
- The differences in recurrence rate between the ECOG ACRIN E5194 (10.5%) and the RTOG 9804 (6.7%) trials in the low risk groups:
- May be secondary to the higher proportion of patients who took tamoxifen in the RTOG 9804 trial
- Two trials, the NSABP B-35 and International Breast Cancer Intervention Studies (IBIS)-II:
- Compared anastrozole (an aromatase inhibitor proven superior to tamoxifen for invasive cancer) with tamoxifen in hormone receptor–positive DCIS managed with local excision
- Both studies were randomized and double-blinded
- The NSABP B-35:
- Was a phase III clinical trial that randomized postmenopausal women with ER-positive DCIS to five years of anastrozole or tamoxifen following BCS and whole breast RT
- The trial sought to determine how effective anastrozole is compared to tamoxifen in preventing a breast cancer recurrences, as well as the quality of life of patients taking anastrozole
- It accrued 3104 women between 2003 to 2006 with nine years of follow up
- The inclusion criteria included postmenopausal women with estrogen and progesterone receptor (ER / PR) positive DCIS and / or LCIS, that were excised with negative margins
- Investigators found significantly fewer breast cancer events in the anastrozole group (n = 90) compared to the tamoxifen group (n = 122) (HR, 0.73; confidence interval, 0.56–0.96, P=0.0234)
- The estimated 10-year breast-cancer-free interval rates were:
- 93.5% for the anastrozole group compared to 89.2% for the tamoxifen group:
- This recorded difference in breast cancer-free interval:
- Was attributable almost entirely to younger postmenopausal women less than 60 years of age
- This recorded difference in breast cancer-free interval:
- 93.5% for the anastrozole group compared to 89.2% for the tamoxifen group:
- Interestingly the difference between treatments did not become apparent until after five years of follow-up:
- Likely due to the low number of events in both group
- There was no difference in OS between the two treatment groups
- The IBIS-II:
- Accrued 2980 women between 2003 to 2013 from 238 centers in 17 countries with a follow-up of seven years
- The study randomized postmenopausal women with ER positive DCIS (micro-invasion was permitted), negative surgical margins, and adjuvant RT according to local practices (70% of patients received RT) to lumpectomy plus anastrazole to lumpectomy plus tamoxifen
- The incidence of any breast cancer event was low in both groups (5%):
- Anastrozole was non-inferior to tamoxifen
- DCIS is a non-invasive entity:
- Lymph node involvement is not expected to occur
- If a patient presents with DCIS in the breast but is found to have malignant cells in the lymph nodes preoperatively:
- The patient has, by definition, invasive breast cancer and not DCIS
- In situations where patients have large tumors (greater than 4 cm) or extensive micro-calcifications:
- A focus of invasion can be missed because of limited pathologic sampling:
- There is roughly a 20% to 30% rate of associated invasive disease:
- Reported on final pathology in patients who were diagnosed with DCIS on stereotactic biopsy
- There is roughly a 20% to 30% rate of associated invasive disease:
- This patients, as well as those with high-grade or palpable disease:
- Are at higher risk for lymph node involvement and may also warrant sentinel lymph node (SLN) mapping:
- Particularly if they are undergoing mastectomy or if BCS is to be followed by oncoplastic surgery
- Are at higher risk for lymph node involvement and may also warrant sentinel lymph node (SLN) mapping:
- The risk of not identifying metastatic disease in the lymph nodes must be weighed against the risk of lymphedema associated with SLN dissection in each patient
- A focus of invasion can be missed because of limited pathologic sampling:
- Cox et al, in 1998:
- Reported a positive SLN biopsy rate of 6% in patients with DCIS when a combination of hematoxylin–eosin staining and immunohistochemistry was utilized
- Another study by Klauber-DeMore et al. (2000):
- Identified a positive SLN biopsy rate of 12% in patients with DCIS considered to be at high risk for invasion and among 10% of patients who had DCIS with micro-invasion
- Invasive carcinoma is identified when DCIS is diagnosed by core needle biopsy of a tumor mass:
- In 25% of the cases compared to 13% of the cases when the biopsy is performed for micro-calcifications
- The incidence of identifying a positive SLN:
- Is more frequent in large areas of DCIS:
- Odds ratio of 1.14 per 1 cm increase in size
- When comedo necrosis is present:
- Up to 40% of the cases
- When the DCIS is high nuclear grade:
- 23% vs 7% low-intermediate grade
- When estrogen receptors (ER) / progesterone receptors (PR) are negative:
- 33% vs 11% for ER / PR positive disease
- Is more frequent in large areas of DCIS:
- A study from the MD Anderson Cancer Center (MDACC), (Francis et al. (2015)):
- Investigated the incidence of positive lymph nodes and the clinical significance of these findings in 1,234 patients with an initial diagnosis of DCIS planned for SLN dissection:
- The positive SLN biopsy rate was 10.7% (positive SLNs in 132 patients):
- The results included isolated tumor cells in 66 (5.4%) patients, micro-metastases in 36 (2.9%) and macro-metastases in 30 (2.4%)
- The positive SLN biopsy rate was 10.7% (positive SLNs in 132 patients):
- There was upstaging in the primary tumor in 26.5% of the cases (327 patients) to micro-invasion or invasive cancer
- Factors predictive of a positive SLN were:
- Diagnosis by excisional biopsy
- Papillary histology
- DCIS greater than 2 cm
- More than three interventions prior to SLN dissection (needle biopsy, excisional biopsy, etc.)
- Micro-invasion or invasive cancer
- It was noted that with increasing numbers of preoperative interventions (biopsy, needle localization, etc.):
- There was a higher likelihood of positive SLN findings:
- With the majority being isolated tumor cells (44/907, 4.2%) or micro-metastases (12/907, 1.3%)
- There was a higher likelihood of positive SLN findings:
- There were no macro-metastases identified in the SLNs of patients with pure DCIS
- The high incidence of isolated tumor cells in the SLNs with increasing preoperative interventions supports the concept of benign mechanical transport of epithelial cells during manipulation of the primary tumor
- At a median follow-up of 61.7 months:
- There was no difference in disease-free survival (DFS) outcomes in the patients with pure DCIS with or without positive SLN findings
- Investigated the incidence of positive lymph nodes and the clinical significance of these findings in 1,234 patients with an initial diagnosis of DCIS planned for SLN dissection:
- In general terms, SLN dissection should be limited to patients who undergo mastectomy for:
- Large, high-grade DCIS because it is difficult to perform lymphatic mapping after a mastectomy if invasive cancer is found in the mastectomy specimen
- The 2017 ASCO guidelines do not recommend SLN biopsy for BCS for DCIS:
- But for large, high-grade DCIS with necrosis one can discuss with the patient the option of performing the SLN biopsy during BCS
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #Surgeon #Teacher #Miami #Mexico #MountSinaiMedicalCenter
