In 1984 Göran Åkerström, on the basis of 503 necropsies, analysed the location of the parathyroid glands:
Together with the work of Gilmour (n=478) and Wang (n=160), they form the foundations of our current knowledge on the subject
Dr. Juan M. Rangone modified the diagrams from Åkerström’s original publication to come up with the percentages of location of the “normodescended” parathyroid glands:
A. Percentages of the different locations of the superior parathyroid glands:
80% corresponds to the midglandular variant
12% to the cricopharyngeal variant
Usually located 1 cm higher than the crossing of the recurrent laryngeal nerve and the inferior thyroid artery
B. Percentages of the different locations of the inferior parathyroid glands:
Roughly 90% are located at the level, or no more than 1 cm below the inferior pole of the thyroid gland
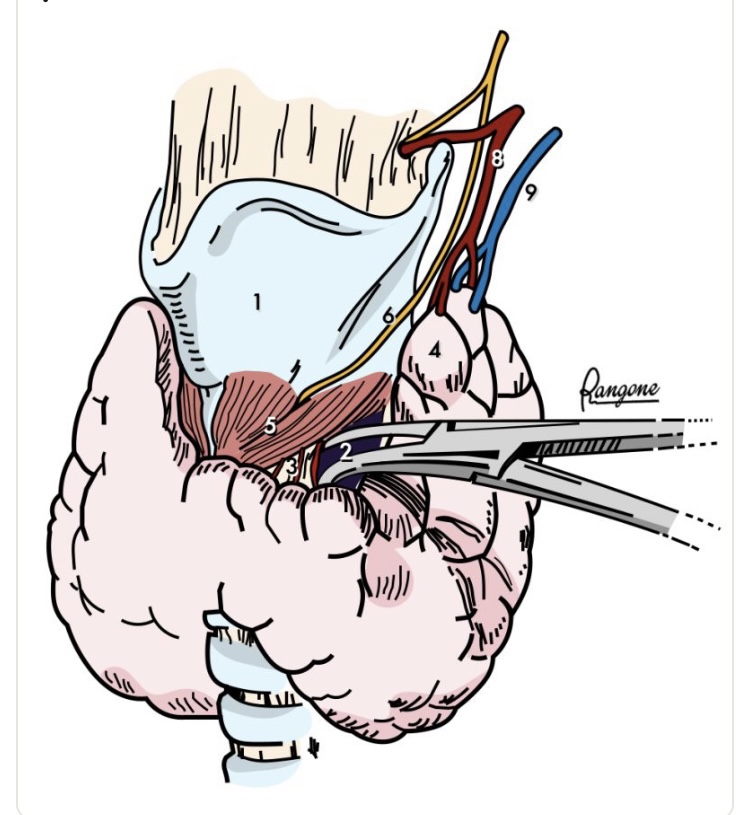
The lower and lateral retraction of the upper thyroid pole:
Reveals a diamond-shaped avascular space
The area is limited:
Medially:
By the lamina of the thyroid cartilage (superiorly) and cricoid cartilage (inferiorly):
Both covered by the cricothyroid muscle
Inferolaterally:
The space is circumscribed by the medial border of the upper thyroid pole and the upper border of the thyroid isthmus
The “roof” of the area:
Is covered by 2 or 3 “bridging” blood vessels that must be controlled to access the space
The “opening” of this virtual space:
Prior to the ligature of the upper thyroid pedicle:
Is a safety maneuver to protect the external branch of the superior laryngeal nerve
Landmarks:
Thyroid cartilage
Reeve cricothyroid space
Space with “bridging” blood vessels
Upper thyroid pole
Cricothyroid muscle
External branch of the superior larngeal nerve
Superior thyroid artery
Superior thyroid vein
Reference:
Abdullah H, Bliss R, Reeve T, Delbridge L (2000) Recognition of the avascular space medial to the upper pole of the thyroid and its surgical implications. Asian J. Surg. 23: 86–9.
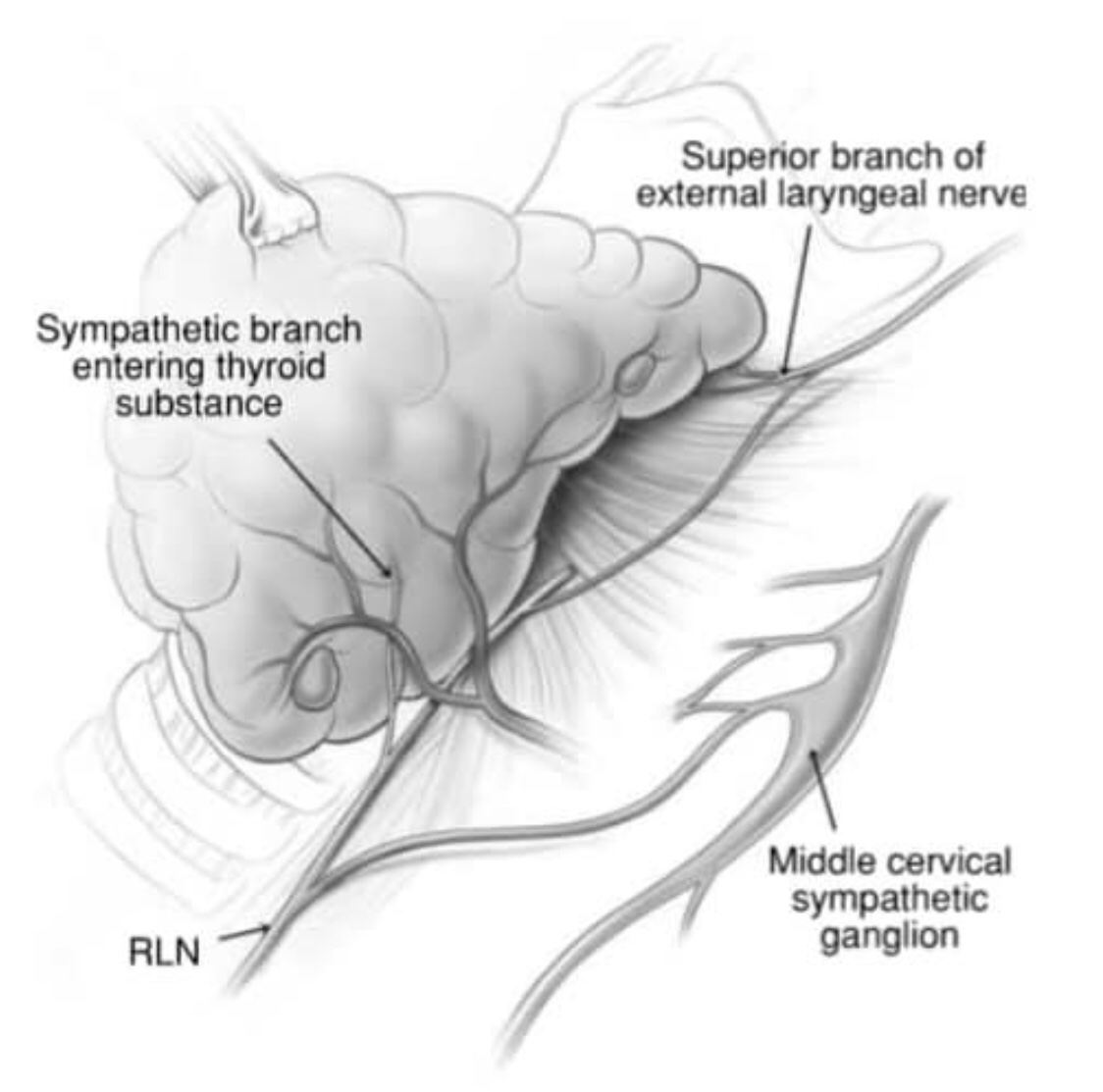
👉The external branch of the superior laryngeal nerve (EBSLN) has been labelled ‘the neglected nerve’ of thyroid surgery.
👉Most surgeons have simply attempted to avoid this nerve on the assumption that so doing will prevent injury; however, it is now recognized that injury is relatively common and associated with the potential for significant impairment, espe- cially for those who use their voices professionally.
👉I was taught to always attempt to identify the nerve and recommend doing so.
👉Recently Aina and Hisham have shown that the nerve can be routinely identified in over 90% of cases, a level that sets a new benchmark for head and neck surgeons / endocrine surgeons.
👉The key to identifying the nerve is to develop the avascular plane between the cricothyroid muscle and the medial border of the upper pole of the thyroid lobe, a manoeuvre facilitated by lateral retraction of the lobe.
👉Awareness of the various positions of the EBSLN according to the Cernea classification is also essential if the nerve is to be both identified and preserved.
👉Type 1 EBSLN are located well clear of the thyroid, more than 1 cm above the upper pole of the lobe passing directly into the cricothyroid muscle.
👉Type 2a nerves pass in the vicinity of the superior thyroid vessels as they enter the gland substance.
👉Type 2b nerves cross over the anterior surface of the thyroid lobe.
👉Awareness of the anatomic variations, such as the nerve of Galen, a direct communication between the RLN and EBSLN, is important in avoiding injury to the nerve.
The true prevalence of iatrogenic injury to the EBSLN during thyroid surgery remains difficult to quantify, largely due to underdiagnosis and variability in clinical presentation.
– The pathophysiology and anatomical risk stratification of EBSLN injury were elegantly described by Cernea et al. in 1992 [1]. In this landmark study, the variant in which the nerve crosses the superior thyroid pedicle below the plane of the upper pole apex—classified as Cernea type 2B—was identified as carrying a high risk of injury.
– Although this configuration was initially reported in approximately 14% of cadaveric dissections by the University of São Paulo group [1], later clinical series by Gianlorenzo Dionigi et al. demonstrated that this “high-risk” anatomy may be present in up to 54% of patients with large or bulky goiters [2], significantly increasing surgical complexity.
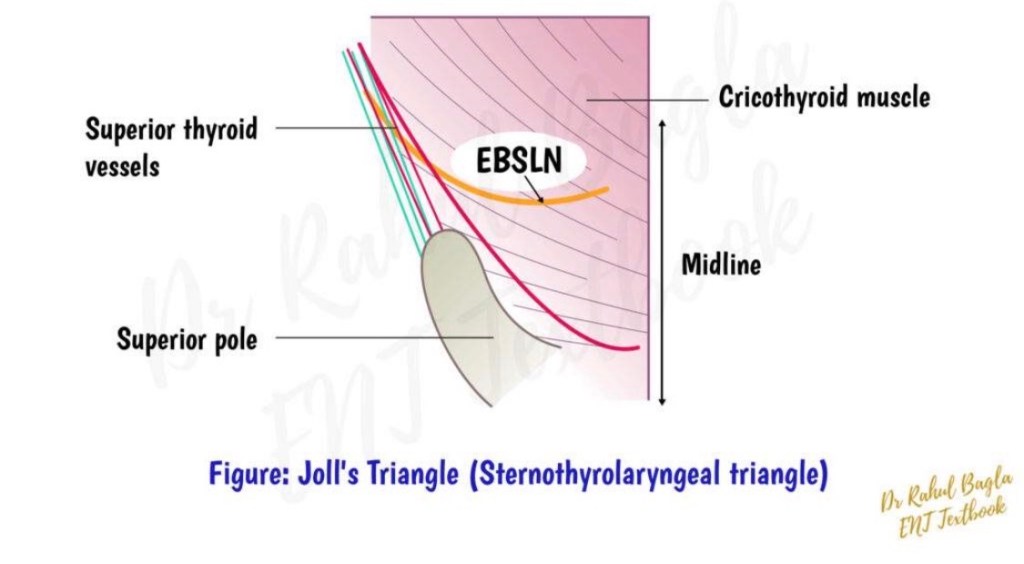
– First popularized by Mossman and DeWeese (1968), Joll’s sterno-thyro-laryngeal triangle remains a valuable anatomical landmark for identifying the EBSLN during superior pole dissection [3].
– In 1986, Michael Friedman provided a detailed description of the surgical approach to the upper thyroid pole that many of us continue to employ in complex cases, particularly when exposure of the EBSLN is critical [4].
– At the supero-external angle of the intermuscular pocket, created to identify the insertion of the sternothyroid muscle on the oblique line of the thyroid cartilage, surgeons frequently encounter a small arterial vessel. While its injury usually causes only minor (though often annoying) bleeding, it serves as an important anatomical landmark.
– These vessels supply the upper portion of the sternohyoid muscle, above the level of the cricoid cartilage.
– According to Wang et al. [5], in approximately 75% of cases, this vessel represents a terminal branch of a common trunk with the cricothyroid artery, originating from the superior thyroid artery. Before bifurcation, this trunk also gives rise to small nourishing branches to the thyrohyoid and omohyoid muscles.
– The so-called “sternohyoid nutrient vessel” is anatomically unique in 56% of cases [5]. After emerging superficially, it enters the (virtual) intermuscular space between the posterior surface of the sternohyoid and the anterior surface of the sternothyroid muscle, following one of two patterns:
✅ coursing along (“hugging”) the lateral border of the sternothyroid muscle, or ✅ directly piercing the most cranial fibers of the sternothyroid muscle.
– Awareness of this vascular anatomy can facilitate safe superior pole dissection, improve EBSLN identification, and ultimately reduce the risk of voice-related complications following thyroid surgery.
References
Cernea CR, et al. Identification of the external branch of the superior laryngeal nerve during thyroidectomy. Am J Surg. 1992. Dionigi G, et al. Surgical anatomy of the external branch of the superior laryngeal nerve. Gland Surg. Mossman HW, DeWeese MS. The surgical anatomy of the larynx. 1968. Friedman M. Surgical management of the superior thyroid pole. Otolaryngol Clin North Am. 1986. Wang C, et al. Vascular supply of the infrahyoid muscles and its surgical relevance. Surg Radiol Anat.
Sentinel Lymph Node Biopsy vs No Axillary Surgery in Patients With Small Breast Cancer and Negative Results on Ultrasonography of Axillary Lymph Nodes:
The SOUND Randomized Clinical Trial. Gentilini et al. JAMA Oncol. 2023 Sep 21:e233759. doi: 10.1001/jamaoncol.2023.3759
The SOUND trial that was published in JAMA Oncology concluded:
That patients with small breast cancer (less than 2 cm) and sonographically normal appearing lymph nodes:
Can be safely spared any axillary surgery:
Whenever the lack of pathological information does not affect the postoperative treatment plan
This study was designed to evaluate whether omission of sentinel lymph node (SLN) surgery in patients with negative axillary ultrasound:
Was noninferior to SLN surgery in terms of 5 year distant disease free survival
While this trial is unlikely to change practice immediately:
It is a thought provoking study that will likely generate multidisciplinary discussion
Phase III Randomized Controlled Trial:
Conducted at 18 European hospitals from 2012 to 2017:
Italy, Spain, Switzerland, and Chile:
Recruitment Feb 6, 2012 – Jun 30, 2017
Enrolled patients with invasive breast cancer up to 2 cm, cN0, planning for breast conserving surgery (BCT) and adjuvant radiation therapy (XRT) who had an axillary US showing no LN involvement on imaging:
If doubtful – FNA performed and had to be negative:
1406 negative AUS, 57 with negative FNA
Patients were randomized to SLN surgery vs no axillary surgery
Analysis cohort:
1405 women:
708 SLN
697 no axillary surgery
Median age 60
Tumor size 1.1 (IQR 0.8-1.5cm)
ER+ / Her2- disease in 87.8%
In the SLN group:
13.7% had positive nodes on SLN:
5.1% macrometases
8.6% micrometastases
2.0% had ≥ 2 positive SLNs, 0.6% had pN2 disease
Recommended adjuvant systemic therapy and radiotherapy were similar in the two groups:
20.1% of SLN group and 17.5% of no axillary surgery group received chemotherapy
98.0% of SLN group and 97.6% of no axillary surgery received radiation
83.3% (593 pts) vs 81.1% (565 pts) had whole breast radiation over 3 to 5 weeks
10.7% (76 pts) vs 10.8% (75 pts) had partial breast radiotherapy
3.4% (24 pts) vs 5.6% (39 pts) had intraoperative boost of ELIOT (12 Gy) followed by a hypofractionated course of whole-breast radiotherapy (37.05 Gy in 13 fractions)
The study authors concluded that patients with patients with small breast cancer with sonographically normal appearing lymph nodes:
Can be safely spared any axillary surgery:
Whenever the lack of pathological information does not affect the postoperative treatment plan
This study provides further data:
Supporting that axillary sentinel lymph node surgery does not provide therapeutic benefit
In the no axillary surgery group:
The cumulative incidence of lymph node recurrences in the axilla was very low:
0.4% at 5 years:
Despite a 13.7% rate of nodal involvement in the SLNB group
However, SLN surgery likely still has a role in certain patients for staging to guide adjuvant therapies:
In particular in young patients:
Where chemotherapy is associated with survival benefit for node positive disease (Rx-Ponder patient)
Furthermore, while adjuvant treatment recommendations in terms of rate of chemotherapy was similar between the two groups:
Identification of nodal positivity in ER+ breast cancer:
Also influences treatment options in terms of:
CDK4/6 inhibitor eligibility as well as consideration of extended endocrine therapy (to 10 years)
Many patients are interested in potential for omission of radiation therapy:
The trial required radiation, with 90% of patients having whole breast radiation and 10% partial breast radiation
Some of the patients in this trial with small breast cancers aged > 65 would be candidates for consideration of omission of radiation
This creates a dilemma regarding de-escalating axillary surgery leading to potential escalation of adjuvant radiation
It should be noted that tumor grade was not an inclusion / exclusion factor:
However, 18% had grade 3 disease
Patients with grade 3 disease have higher likelihood of nodal positivity:
Should omission of SLN surgery be limited to grade 1 and 2 disease at outset
Especially as grade 3 disease with 1 to 3 positive nodes:
Would make patients eligible for CDK4/6 inhibitor
Genomic scores were not included on this trial:
Most patients with ER+ / Her2- disease (with tumors > 1 cm in size) would be considered for genomic testing to guide systemic treatment recommendations
In summary:
Multidisciplinary discussion will be important before implementing any changes in practice as a result of the SOUND trial
I look forward to additional data from several other trials evaluating this question over the upcoming years:
Suggested that completion axillary dissection can be avoided in patients with:
cT1 to cT2, cN0 breast cancer with sentinel lymph node (SLN) metastasis:
Provided that systemic therapy and whole-breast irradiation (WBI):
Are incorporated into the treatment strategy for early-stage breast cancer following breast-conserving surgery (BCS)
This trial enrolled:
Clinically node-negative patients with:
Tumors less than 5 cm in size and with 1 to 2 positive SLNs by hematoxylin and eosin staining who were treated with BCS and planned WBI
Patients were randomized to:
SLN biopsy alone vs. axillary lymph node dissection (ALND)
The 10-year:
Overall survival was similar in the SLNB only group compared to the ALND group:
86.3% vs. 83.6%, p = 0.72
Disease-free survivalwas similar in the SLNB only group compared to the ALND group:
80.2% and 78.2%
In patients treated with ALND:
27% had additional non-SLN disease found at the time of ALND:
Suggesting that patients treated with SLNB alone would have a similar disease burden:
Yet, nodal recurrence rates were similar between the SLNB and ALND groups at 10 years:
1.5% vs. 0.5%, p = 0.13
Suggesting that systemic therapy and radiation therapy:
Provide adequate local control in patients with limited disease burden in the axilla
The AMAROS trial:
Is a phase III non-inferiority study:
Comparing ALND with axillary radiation therapy in patients with:
Clinical T1 / T2 N0 breast cancer with a positive sentinel node
The trial showed low 5-year rates of regional recurrence:
In the ALND and axillary radiation therapy groups:
0.43% vs 1.19%, respectively
But the risk of patient perceived (subjective) or measured (objective) lymphedema:
Was twice as high in the ALND arm compared to the radiation arm:
Subjective
23% vs. 11% after 5 years of follow-up
Objective:
13% vs. 5% after 5 years of follow-up
The ACOSOG Z0010 trial:
Evaluates the incidence and impact of SLN and bone marrow micro-metastases on patients with early-stage breast cancer treated with BCS and radiation
It demonstrated that:
Identification of occult disease in the SNs with immunohistochemistry was not associated with survival
References:
Giuliano AE, McCall L, Beitsch P, Whitworth PW, Blumencranz P, Leitch AM, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 Randomized Trial. Ann Surg. 2010;252(3):426-432.Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347(16):1227-1232.Rutgers EJ, Donker M, Straver ME. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer patients: final analysis of the EORTC AMAROS trial (10981/22023). J Clin Oncol. 2013;31 (suppl; abstr LBA1001). Available at: http://meetinglibrary.asco.org/content/109779-132. Accessed November 7, 2013.Straver ME, Meijnen P, van Tienhoven G, et al. Sentinel node identification rate and nodal involvement in the EORTC 10981-22023 AMAROS trial. Ann Surg Oncol. 2010;17:1854-1861.
Hunt KK, Ballman KV, McCall LM, et al. Factors associated with local-regional recurrence after a negative sentinel node dissection: results of the ACOSOG Z0010 trial. Ann Surg. 2012;256:428-436.
General morbidity data and reviews echo this principle
Field/Dose (typical in AMAROS):
Axilla levels I to III ± SCV, ~ 50 Gy in conventional fractions; most modern clinics use tangents / high tangents plus nodal fields as indicated. (Protocol details in trial reports.)
Bottom line:
ART = ALND for control, with less arm morbidity:
So when axillary therapy is needed after a positive SLN:
In 38% (16 / 42) of clinically node-negative but pathologically node-positive axillae:
The sentinel node was the only involved node:
Limited disease that a blind sample / low-level dissection might have missed PubMed
Anatomic insight:
Among the last 54 mapped cases:
10 had level II-only metastases:
Underscoring why targeted mapping can outperform low-level sampling PubMed
Why it mattered?
Provided the first clinical proof-of-concept in breast cancer that a mapped SLN can accurately stage the axilla with far less surgery:
Laying the groundwork for later multicenter validation (Krag 1998) and definitive RCTs (NSABP B-32, ACOSOG Z0011) that enabled omission of routine ALND in properly selected patients PubMed
Practical pearls / caveats:
Learning curve is real:
Early experience showed lower identification and some false-negatives
Performance improved to perfect concordance in later cases
Training and standardized technique are crucial PubMed
Technique used here was blue dye alone (pre-radioisotope era):
Subsequent adoption of radiotracer (± dye) further raised identification and lowered FNR, but the 1994 study established the principle
Can a radioisotope-guided sentinel lymph node (SLN) biopsy accurately predict the status of the axilla in breast cancer across multiple surgeons and practice settings?
Methods:
Population and setting:
443 women with breast cancer:
Treated by 11 surgeons at varied centers
Everyone underwent complete axillary lymph node dissection (ALND) so SLNB performance could be verified
Technique:
Peritumoral / pericavity injection of:
4 mL technetium-99m sulfur colloid (≈1 mCi / 37 MBq):
Intraoperative hand-held gamma probe to find “hot spots,” then SLN excision followed by ALND
Key performance metrics:
Identification (“hot-spot”) rate:
93% (413 / 443)
Accuracy vs full axillary histology:
97% (392 / 405)
Sensitivity:
89% (101/114):
False-negative rate ≈ 11% among node-positive cases
Specificity / PPV:
100% (no false positives)
NPV:
96% (291/304)
Anatomic insight:
SLNs were outside the axilla in 8% and outside level I in 11%
3% of positive SLNs were in non-axillary locations
Why it mattered?
Provided the first large, multicenter, surgeon-diverse validation:
Showing SLN biopsy is a highly accurate predictor of axillary status:
Establishing the foundation for replacing routine ALND in cN0 patients and enabling the de-escalation pathway:
Later confirmed by trials like NSABP B-32 and Z0011
Nuances and caveats the paper raised:
Learning curve / variability:
Success varied by surgeon and patient factors, underscoring the need for technique standardization and training
Technique scope:
Study used radioisotope only (no blue dye in the protocol):
Which many centers later combined with blue dye to further enhance identification and lower FNR:
Background reviews consistently show higher detection and lower FNR with combined mapping
Design/Pop: Phase III, HR+/HER2– stage II–III EBC; broadened risk (included select stage IIA N0 with high genomic/grade risk). Randomized to ribociclib 400 mg (3 weeks on/1 off) for 3 years + NSAI vs NSAI alone; ET planned ≥5 years. Primary endpoint: iDFS. Primary readout: With ~33 mo median follow-up, iDFS HR ~0.75 (0.749; 95% CI 0.628–0.892; P=0.0012). Absolute benefit over time: Exploratory 4-year update shows absolute iDFS improvement grew from ~2.7% at 3 yrs to ~4.9% at 4 yrs; distant relapse-free survival favored ribociclib. Subgroups: Benefit consistent across stage II and III and other pre-specified groups (methodology commentary). Safety/Tolerability: Lower starting dose (400 mg) chosen for adjuvant tolerability; class-expected AEs (neutropenia, LFT elevations, QTc monitoring needed). (Trial design/safety overviews).
Regulatory & guidelines
US FDA (Sept 17, 2024): Ribociclib + an aromatase inhibitor approved for adjuvant treatment of HR+/HER2– stage II–III EBC at high risk of recurrence (also a ribociclib/letrozole co-pack). Guideline movement: Professional guidance in 2024–2025 reflects inclusion of adjuvant CDK4/6 inhibition (abemaciclib in monarchE-eligible; ribociclib after approval per NATALEE risk criteria). Check current NCCN/ASCO updates locally. UK/NICE (Apr 2025): Ribociclib endorsed for early HR+/HER2– disease (node-positive high-risk), with access caveats for node-negative high-risk.
How NATALEE compares to monarchE (abemaciclib)
monarchE (2 years abemaciclib continuous + ET; high-risk node-positive only) has durable iDFS/DRFS gains and now a statistically significant OS benefit (HR ~0.84; 7-yr OS 86.8% vs 85.0%). NATALEE uses intermittent ribociclib for 3 years and broader eligibility (including some node-negative). It delivers robust iDFS benefit with growing absolute separation on longer follow-up; OS not yet mature.
Practical takeaways for clinic
Who fits NATALEE-style ribociclib? HR+/HER2– stage II–III at high risk (e.g., node-positive; select node-negative with high genomic/grade risk). Confirm payer/regulator language in your region. Duration & dosing: Ribociclib 400 mg, 3 weeks on/1 off for 36 months + AI; plan ET for ≥5 years. Monitor ANC, LFTs, and QTc. Choosing the CDK4/6 agent: Abemaciclib remains a strong default in classic monarchE-eligible high-risk node-positive patients—now with OS data. Ribociclib extends adjuvant CDK4/6 benefit to broader early-stage risk per NATALEE and is FDA-approved for stage II–III high-risk. Consider patient comorbidities (QTc, liver), logistics of a 3-year course, and shared decision-making.
Key sources to cite in slides
Hortobagyi GN et al. Ann Oncol 2025; NATALEE primary publication (iDFS HR 0.749). ESMO Oncology News 2025; 4-year NATALEE exploratory analysis (absolute iDFS gain ~4.9% at 4 yrs). FDA label/news for adjuvant ribociclib (Sept 2024). monarchE OS update 2025. ASCO/NCCN updated guidance on adjuvant CDK4/6 use.