My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
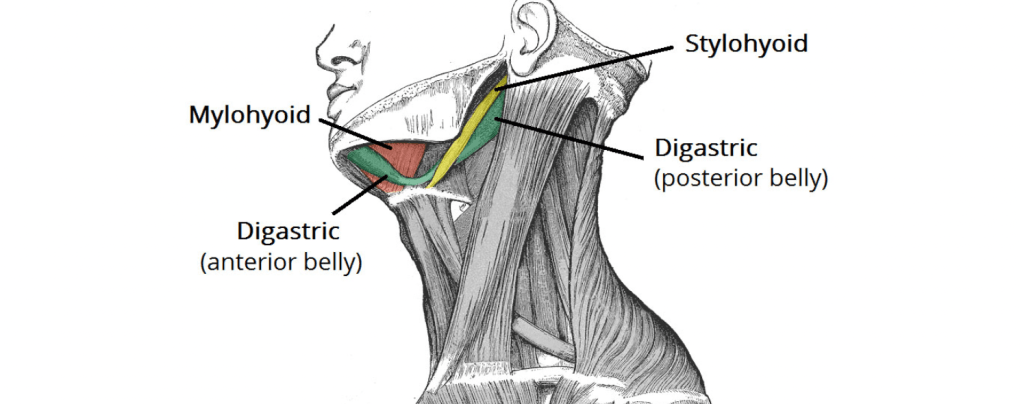
The posterior belly, longer than the anterior belly, arises from the mastoid notch which is on the inferior surface of the skull, medial to the mastoid process of the temporal bone. It lies posterior to the parotid gland and the facial nerve. The mastoid notch is a deep groove between the mastoid process and the styloid process. The mastoid notch is also referred to as the digastric groove or the digastric fossa.
The digastric muscle stretches between the mastoid process of the cranium to the mandible at the chin, and part-way between, it becomes a tendon which passes through a tendinous pulley attached to the hyoid bone. It originates from the second pharyngeal arch
“The resident’s friend”: Few qualms are as useful as the posterior belly of the digastric muscle.
It helps us to recognize…
Nerves: its cranial border is related to the facial nerve (VII PC), its caudal border to the spinal nerve or accessory (XI PC).
Vessels: on its ventral face rests the facial vein (posterior) or the retromandibular vein, on its dorsal face the facial artery.
They constitute, together with the omohyoid muscle (also morphologically digastric), the “protectors” of the internal jugular vein. Both muscles stand in the way of the surgeon’s scalpel to the junction of the vascular axis of the neck (the posterior belly does so at level IIa, the intermediate tendon of the omohyoid at the boundary between III-IV).
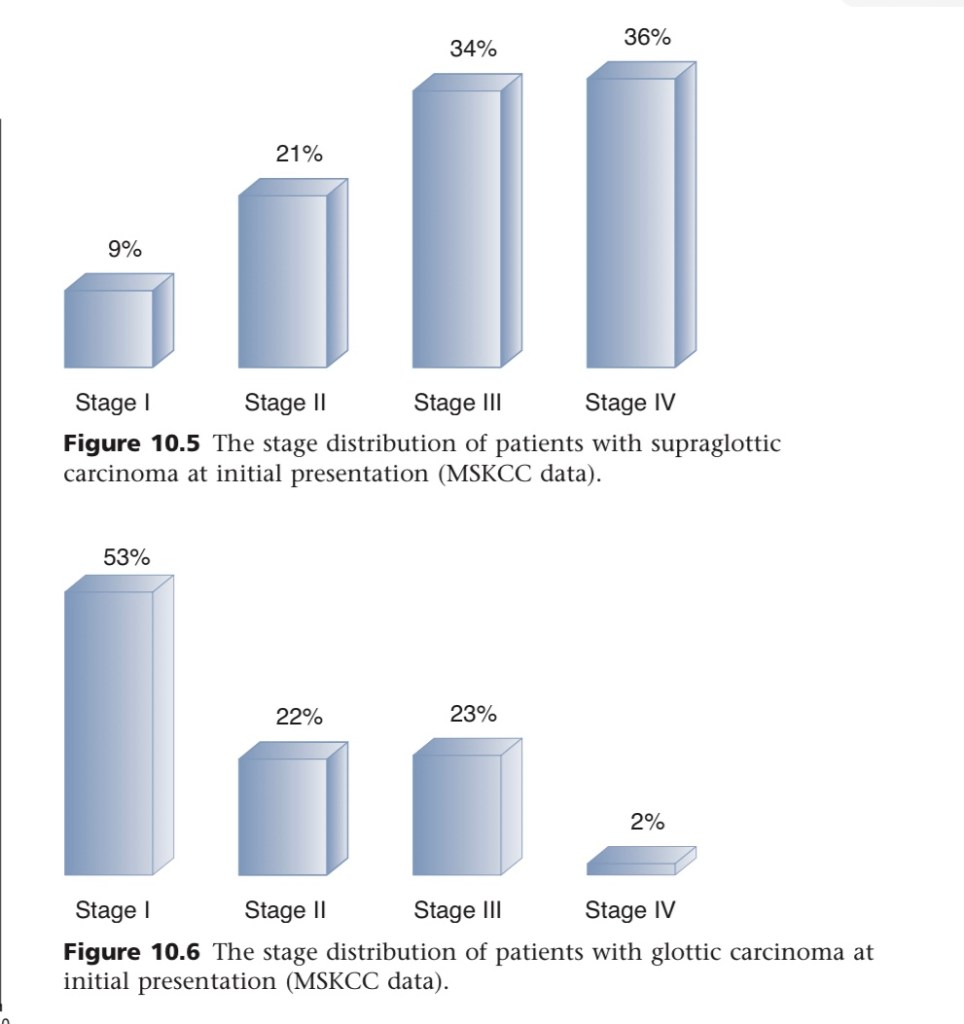
The glottic region is by far the most common site for primary malignant tumors in the larynx.
The stage distribution of patients with supraglottic carcinoma and glottic carcinoma at the time of presentation at Memorial Sloan Kettering Cancer Center is shown in the figures.
75% of patients with glottic carcinoma have localized disease at the time of diagnosis, in contrast to nearly 70% of patients with supraglottic carcinoma who have advanced disease at presentation.
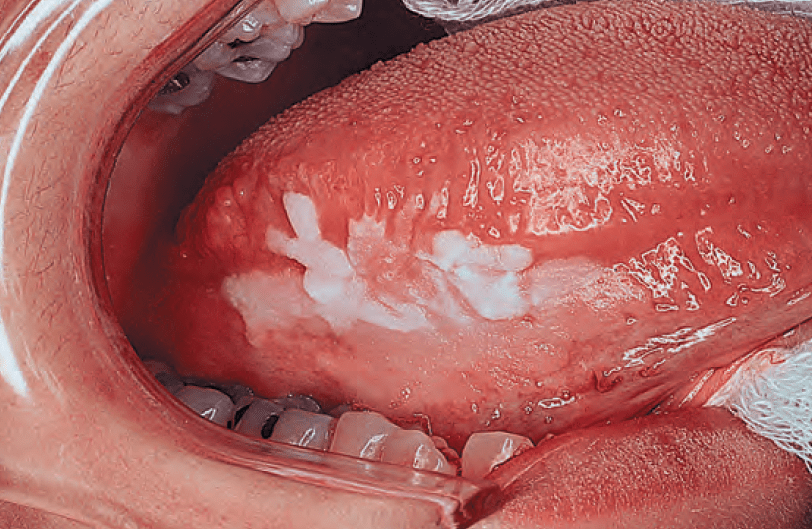
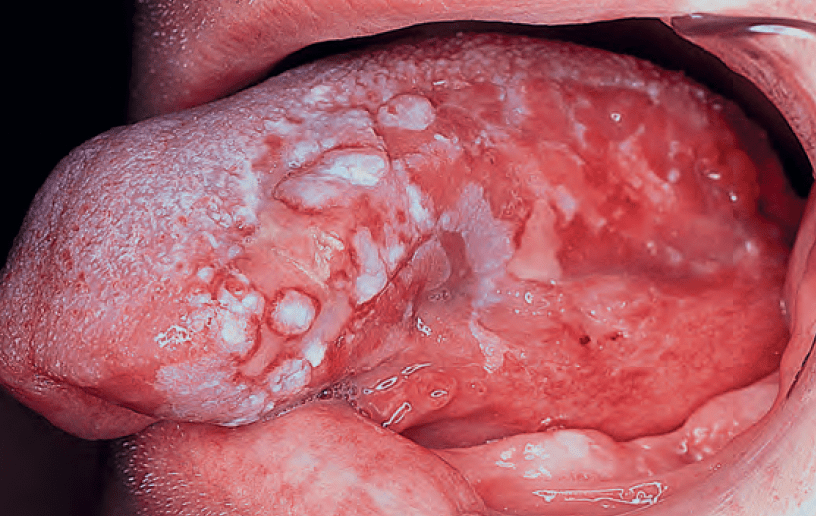
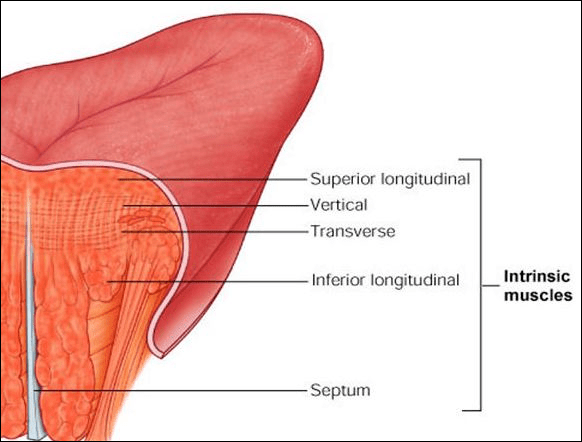
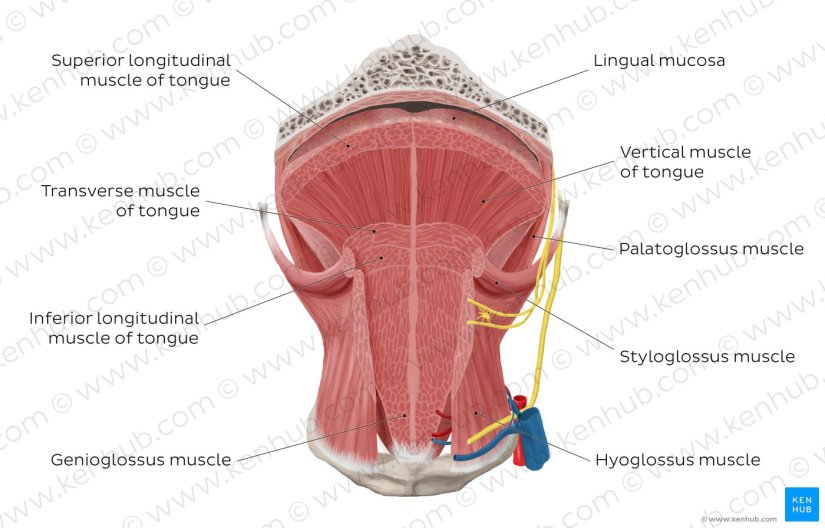
The intrinsic muscles (bilateral superior and inferior longitudinal, transverse, and vertical muscles) interdigitate and have no tissue spaces, which allows invasive cancers to spread easily.
On the other hand, infiltration of the extrinsic muscles of the tongue (genioglossus, hyoglossus, styloglossus, and palatoglossus) is a feature of locally advanced cancer.
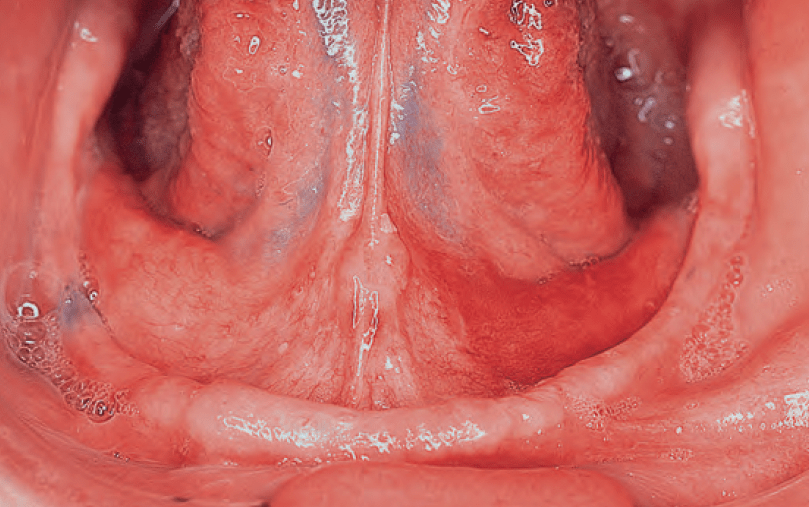
The arterial supply to the tongue and floor of the mouth is from the:.
Dorsal lingual, sublingual, and deep lingual branches of the lingual artery.
The venous drainage of the tongue is into the lingual veins:
Which drain into the facial and retromandibular veins:
Which join to form the common facial vein.
Vasculature Tongue:
Similar to most of the head and neck region, the tongue derives its arterial blood supply from the external carotid artery.
The lingual arterybranches off the external carotid artery deep to the stylohyoid muscle:
At first, it travels superomedially; after a short distance, it changes direction and moves anteroinferiorly.
The hypoglossal nerve (cranial nerve XII) crosses over it laterally before it enters the tongue deep in the hyoglossus muscle.
Within the tongue, the lingual artery gives rise to its three main branches:
The dorsal lingual artery:
The dorsal lingual artery supplies the base of the tongue
The deep lingual artery:
The deep lingual artery travels on the lower surface of the tongue to the tip.
The sublingual artery:
A branch to the sublingual gland and the floor of the mouth is known as the sublingual artery.
The veins of the tongue parallel the lingual artery branches:
The deep lingual vein begins at the tip of the tongue and travels posteriorly to join the sublingual vein:
This veins drains into the dorsal lingual vein, which accompanies the lingual artery.
The dorsal lingual vein drains into the lingual veins:
Which drain into the facial and retromandibular veins, which join to form the common facial vein:
Directly or indirectly, this vein empties into the internal jugular vein.
The hypoglossal nerve provides motor innervations to all muscles of the tongue except the palatoglossus:
Which is supplied by the pharyngeal plexus.
The lingual nerve is the sensory nerve to the anterior two thirds of the tongue, the floor of the mouth, and the lower gum, while taste sensation is carried along the chorda tympani branch of the facial nerve.
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon and is a member of Mount Sinai Medical Center.
He is first author on some publications on oral cavity cancer:
Oral Tongue Cancer: Literature Review and Current Management
Knowledge of anatomy allows us to infer probable complications of parotidectomies.
Facial nerve motor weakness is a complication inherent to the extent of the operation, the extent of the tumor and technique used (less common in extracapsular dissections and partial parotidectomies, more common in superficial, deep-lobe or total parotidectomies).
The rates of transient injury in the literature are highly variable and there are large biases.
The lack of sensation or pre auricular and auricular paraesthesia will depend on the preservation of the posterior branch of the greater auricular nerve (at 24 months: 31% vs. 71%, with and without preservation respectively).
Frey’s syndrome (also called “gustatory sweating” syndrome) and First Bite Syndrome are more common in parotidectomies that include the deep lobe of the gland.
Frey’s has been linked to disruption of the secretagogue [parasympathetic] innervation of the gland (mediated through the auriculotemporal nerve).
The First Bite Syndrome occurs more frequently after surgeries for tumors located in the retromandibular prolongation of the gland, or in the pre-styloid space (parapharyngeal), which sometimes force to ligate the external carotid artery causing disruption of the sympathetic innervation.
Played a critical role in the establishment of breast conserving surgery (BCT):
As a preferred mode of treatment for women with small breast cancers (≤ 2 cm)
For this study, 701 women with tumors ≤ 2 cm and clinically negative axillary examinations:
Were enrolled and randomized to radical mastectomy (n = 349) versus BCT (quadrantectomy and axillary node dissection) followed by radiotherapy (n = 352)
Results from Milan I:
Were concurrent with those from NSABP B-06 trial:
Showing no appreciable differences in long-term survival between the groups:
Despite a higher cumulative incidence of recurrence at 20 years in patients treated with BCT
Ipsilateral breast tumor recurrence rates after 20 years follow-up were:
8.8% for the BCT group compared to a 2.3% rate of local recurrence for the radical mastectomy group (P<0.001)
Additionally, there were no significant differences between the two groups in the rates of contralateral breast cancer, distant metastases, or secondary primary cancers.
Overall, Milan I concluded that:
Long-term survival was the same for women who underwent radical mastectomy as those who received BCT:
Thus providing more evidence to support breast-conserving surgery as treatment for women with small cancers
References
Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347(16):1227-1232.
Julian TB, Venditti CA, Duggal S. Landmark clinical trials influencing surgical management of non-invasive and invasive breast cancer. Breast J. 2015:21(1);60-66.