My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
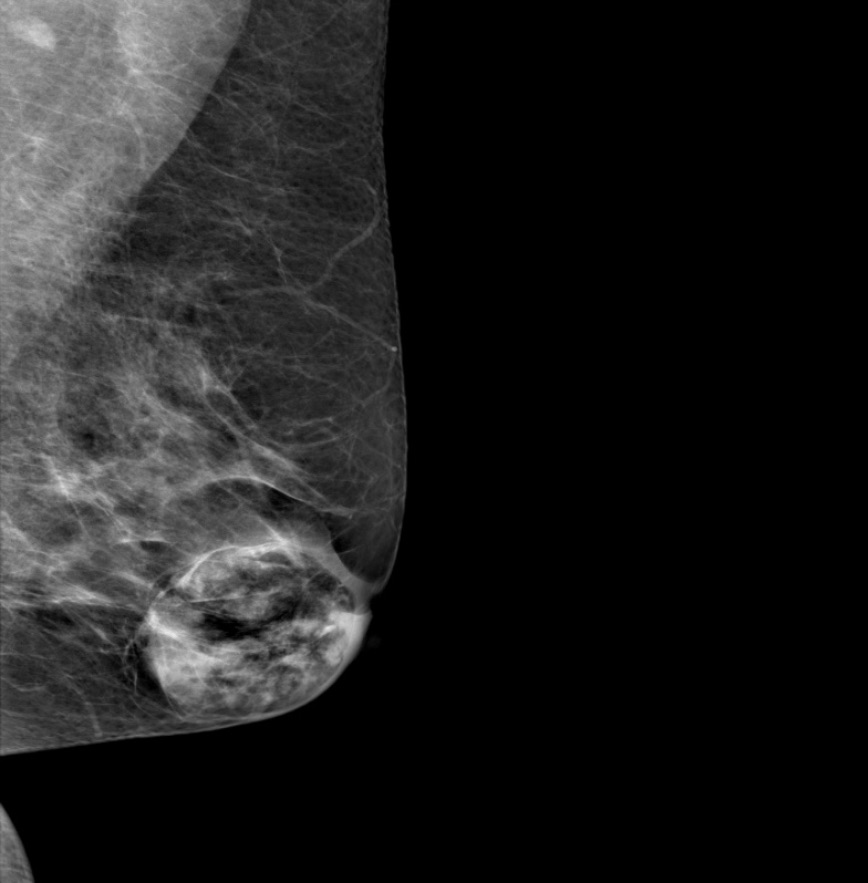
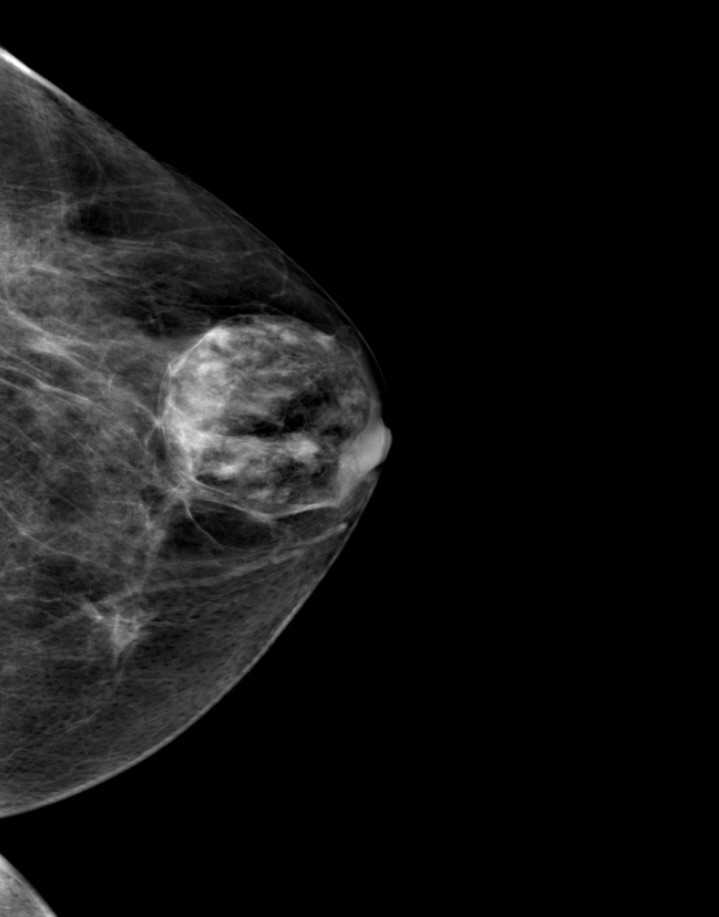
An overgrowth of a portion of normal breast tissue, or from fibrous and glandular elements becoming incorporated into a lipomatous growth:
Thus, they are sometimes called a “breast within a breast”
They are also variously called adenolipofibroma, lipofibroadenoma, adenolipofibroma, and fibroadenolipoma:
Because they contain fibrous, fatty, and epithelial tissues
They may present as palpable masses:
But are more commonly discovered on routine imaging
They are round, oval, or lobulated, and usually are well-circumscribed
They have a mixture of water density and fatty elements and frequently have either a capsule or the appearance of a capsule resulting from surrounding compressed breast tissue
A mammographically classic hamartoma does not require further imaging, short interval follow-up, or biopsy
The presence of a breast hamartoma:
Should prompt further questioning of the patient to be sure there is nothing to suggest she has multiple hamartoma syndrome (Cowden syndrome):
A rare disorder caused by a deleterious mutation:
In the phosphatase and tensin homolog (PTEN) gene
Patients with this disorder have an:
Increased head circumference
Multiple trichilemmoma skin lesions
Intestinal hamartomas
An increased risk of cancer of the:
Breast, thyroid, endometrium, and kidney
Genetic testing should be done if there is a personal or family history suggestive of the disorder
References
Crothers JG, Butler NF, Fortt RW, Gravelle IH. Fibroadenolipoma of the breast. Br J Radiol. 1985;58(687):191-202.
Daya D, Trus T, D’Souza TJ, Minuk T, Yemen B. Hamartoma of the breast, an underrecognized breast lesion. A clinicopathological and radiographic study of 25 cases. Am J Clin Pathol. 1995;103(6):685-689.
Murat, A, Ozdemir H, Yildirim H, Poyraz AK, Ozercan R. Hamartoma of the breast. Australas Radiol. 2007;51(Spec No.):B37-B39.
Schrager CA, Schneider D, Gruener AC, Tsou HC, Peacocke M. Clinical and pathological features of breast disease in Cowden’s syndrome: an underrecognized syndrome with an increased risk of breast cancer. Hum Pathol. 1998;29(1):47-53.
Three of these are given off in the floor of the mouth:
These three branches form an extensive anastomotic network that ensures a rich blood supply to the muscles of the tongue and other structures in the floor of the oral cavity
The lingual artery:
Arises from the anterior surface of the external carotid artery in the neck
It emerges close to the tip of the greater horn / cornu of the hyoid bone:
Lies on the middle pharyngeal constrictor muscle
From its origin, the artery arches upwards and anteriorly:
Giving off its first branch:
The suprahyoid artery
The lingual artery then travels deep to the hyoglossus muscle:
Where it gives off the dorsal lingual arteries
The artery then continues into the floor of the mouth:
Passing lateral to the genioglossus muscle
At the anterior border of the hyoglossus muscle:
The lingual artery takes an upward turn and bifurcates into:
The deep lingual and sublingual arteries
Along its path:
The lingual artery is accompanied by the lingual veins and the glossopharyngeal nerve (cranial nerve IX)
The lingual artery has four branches;
The suprahyoid branch:
Travels along the superior border of the hyoid bone
It anastomoses with its counterpart on the contralateral side:
To supply the muscles attaching to the hyoid bone
The dorsal lingual branches:
Form anastomoses with their contralateral counterparts:
To supply the base of the tongue and its mucous membrane, as well as the palatoglossal arch, tonsil, soft palate and epiglottis
These branches are normally two to three small vessels that branch off the lingual artery medial to the hyoglossus muscle and pass into the posterior aspect of the tongue
The sublingual branch:
Supplies the sublingual gland, mylohyoid muscle and the buccal and gingival mucous membranes
It arises at the anterior border of the hyoglossus muscle and travels between the genioglossus and mylohyoid muscles to reach the sublingual glands
The deep lingual branch:
Forms the terminal portion of the lingual artery
It supplies the body of the tongue
The artery is located on the inferior aspect of the tongue close to the lingual frenulum
It passes between the genioglossus medially and the inferior longitudinal muscle laterally to reach the apex of the tongue
Breast pain (mastalgia) is common in women and occasionally occurs in men
Although it is usually mild and self-limited:
Approximately 15% of affected women require treatment
Evaluation of breast pain is important to determine whether the pain is due to:
Normal physiological changes related to hormonal fluctuation or to a pathologic process such as breast cancer
Breast pain:
Is a rare symptom of breast cancer
Women who present with breast pain but who have a normal exam and imaging studies:
Can be reasonably assured that their risk of breast cancer is:
Similar to that of a woman without breast pain
While cyclical breast pain has traditionally been attributed to fibrocystic changes, chronic cystic mastitis, and mammary dysplasia:
Breast pain and nodularity are so common that the term fibrocystic “disease”:
Has become obsolete:
It should no longer be used
Epidemiology:
Breast pain is common:
Up to 70% of women in Western societies:
Will experience it sometime during their lives
One study of almost 1700 women (mean age 34 years) surveyed by online questionnaire:
Found that over one-half (51.5%) had experienced breast pain
Pain was more commonly reported among:
Older women
Those with larger breast sizes
Those less fit and / or physically active
Among women who reported symptoms:
41% and 35% reported negative impacts from breast pain on their sexual health and sleep, respectively
10% of those symptomatic had reported breast pain as an issue for over half of their lives
The prevalence of breast pain appears to depend on the population studied:
Breast pain is less common in Asian cultures:
Affecting as few as 5% of women
Classification and etiology:
Breast pain can be classified into three categories:
Cyclical
Noncyclical
Extramammary
Clinically it is more important to differentiate between extra mammary and true breast pain than between cyclical and noncyclical pain:
This is because management of cyclical and noncyclical breast pain is similar:
While extramammary pain may require a different treatment
Cyclical breast pain:
Affects two-thirds of patients with true mastalgia
Cyclical pain is associated with hormonal fluctuations of the menstrual cycle:
Usually presenting in the week prior to onset of menses
It is frequently bilateral and most severe in the upper outer quadrant of the breasts
Minor cyclical breast discomfort is normal:
It begins during the late luteal phase and dissipates with the onset of menses
This is usually bilateral and diffuse pain
Cyclical breast discomfort is caused by normal hormonal changes associated with ovulation:
That stimulate the proliferation of normal glandular breast tissue and result in pain
The stimulation of ductal elements by estrogen, stimulation of the stroma by progesterone, and / or stimulation of ductal secretion by prolactin:
All contribute to cyclical pain during the menstrual cycle
Cyclical breast pain can also be associated with pharmacologic hormonal agents:
Postmenopausal hormone therapy
Oral contraceptive pills
Noncyclical breast pain:
Affects one-third of women with true mastalgia
The pain does not follow the usual menstrual pattern:
May be constant or intermittent
More likely to be unilateral and variable in its location in the breast
Noncyclical breast pain is more likely to be related to:
A breast or chest wall lesion
Possible etiologies include:
Large pendulous breasts:
May cause pain due to stretching of Cooper’s ligaments
Neck, back, shoulder pain and headache may be present, as well as a rash under the pendulous breast in the inframammary fold
Diet, lifestyle:
A high-fat diet, smoking, and caffeine intake have been associated with breast pain:
It is difficult to conduct randomized trials with appropriate blinding that will negate the placebo effect
Hence, there is currently no high-quality evidence to suggest that a low-fat diet, smoking cessation, or caffeine avoidance reduces breast pain
Hormone replacement therapy :
Up to one-third of menopausal women receiving postmenopausal hormone therapy experience some degree of noncyclical breast pain:
Which may spontaneously resolve over time
Breast cysts:
Solitary cysts:
Particularly when the presentation is abrupt, are frequently painful
Ductal ectasia:
Is characterized by distention of subareolar ducts:
Due to inflammation unrelated to infection
Ductal ectasia may be associated with fever and acute local pain and tenderness:
Caused by penetration of the duct wall by lipid material:
Which may resolve to leave a subareolar nodule
In one study, the site and degree of duct dilatation correlated with the intensity of noncyclical breast pain
Mastitis:
Mastitis or breast abscess typically presents as a painful, swollen, and red breast in a febrile woman
Mastitis is more prevalent during lactation but can also occur in nonlactating women:
Idiopathic granulomatous mastitis [IGM] or smokers
Inflammatory breast cancer:
Women with de novo inflammatory breast cancer (primary disease) may present with:
Pain and a rapidly progressing tender, firm, enlarged breast
The skin over the breast is warm and thickened, with a “peau d’orange” (orange skin) appearance, but there is often no fever or leukocytosis
Hidradenitis suppurativa:
Although primarily confined to the axilla:
Can involve the breast and present as breast nodules and pain
Other etiologies of breast pain include:
Pregnancy
Thrombophlebitis (Mondor’s disease)
Trauma
Macrocysts
Prior breast surgery
A variety of medications:
Hormones as well as some antidepressants, cardiovascular agents, and antibiotics
Extramammary pain:
Some women who present with breast pain actually have referred pain from sources other than the breasts
The breast is innervated by:
The anterolateral and anteromedial branches of the intercostal nerves (T3 to T5):
Irritation of these nerves anywhere along their course can lead to pain that is felt in the breast or nipple
In some studies done in primary care and certain breast clinic settings, it has been found that women presenting with breast pain:
More often have extramammary pain rather than true mastalgia
Extramammary pain may be from:
Musculoskeletal sources such as the chest wall, spinal or paraspinal disorders, trauma, or scarring from prior biopsy
It may also be related to medical problems such as biliary, pulmonary, esophageal, or cardiac disease
Chest wall pain:
Is frequently due to pectoralis major muscle injury, related to repetitive activities such as water skiing, raking, rowing, or shoveling
Chest wall pain that presents as bilateral parasternal discomfort can also arise from:
Costochondritis:
Typically the second through fifth costochondral junctions
Tietze syndrome:
Typically the second and third costochondral junctions
Other etiologies of chest wall pain include:
Slipping and clicking ribs and arthritis
Spinal and paraspinal disorders:
Radicular chest wall pain may be due to:
Cervical arthritis:
This pain typically occurs in older women in whom vertebral, spinal, and paraspinal problems in the neck and upper thorax accumulate with age
Paraspinal muscle spasm and other impingements on the free course of the sensory nerves from the neck and upper thorax:
Can cause a radiculopathy leading to pain or hyperesthesia
Burning pain, which is typical of nerve root pressure, is a common feature
Imaging studies of the neck may reveal the etiology of the pain
Trauma:
Breast pain can be caused by local trauma, such as seat belt injury, child or pet kicking, or intimate partner violence, to the breasts or anterior chest wall
Pain can also be caused by intercostal neuralgia due to a respiratory infection or underlying pleuritic lesions
Additionally, gallbladder disease or ischemic heart disease may present as intermittent chest pain attributed to the breast
Postthoracotomy syndrome:
Is an unusual disorder in which a healing chest wound simulates the effect of a suckling infant
It can be associated with:
An elevated prolactin concentration
Breast pain
Milk production
A similar effect can be seen with other forms of chest wall irritation, including burns and chafing from clothing overlying the nipple
History:
It may be helpful to ask women with cyclical pain to record the occurrence and severity of breast pain in a diary and note potential aggravating and ameliorating factors
Questions the patient should be asked about her pain include:
Where in the breast or axilla does the pain occur?
Is the pain bilateral?
What does the pain feel like?
How severe is the pain?
If premenopausal:
Is it phasic, with peaks at midcycle and premenstrually?
Is it associated with use of oral contraceptive pills or hormone replacement therapy?
Did it begin after a recent birth or pregnancy loss or termination?
Is it related to vigorous or repetitive use of the pectoral muscle group?
Is there a concurrent neck, back, or shoulder problem?
Are there systemic or other local symptoms, such as fever or erythema?
Is there a history of recent trauma to the chest?
Does the pain affect her ability to perform daily activities?
In addition, a complete medical and surgical history and systematic review of systems should be obtained. Breast cancer risk should be assessed
Chest wall pain is often lateral and may be burning or knifelike, and localized or diffuse
Physical examination:
Breast:
The breast should be examined for signs of inflammation or infection, which would suggest an etiology of mastitis.
Mastitis typically presents as a painful, swollen, and red breast in a febrile woman.
Mastitis is more prevalent during lactation but can also occur in nonlactating women
The key point in examining a woman with breast pain is to look for signs suggestive of breast malignancy:
Such as a mass, skin changes, or bloody nipple discharge
The four breast quadrants, subareolar areas, axillae, and supraclavicular and infraclavicular areas should be systematically examined with the woman both lying and sitting with her hands on her hips and then above her head
The specific goals of the examination are to:
Check for skin changes, noting the symmetry and contour of the breasts, position of the nipples; scars; skin retraction; dimpling; edema or erythema; ulceration or crusting of the nipple; and changes in skin color
Check for enlarged or tender axillary, supraclavicular, or infraclavicular lymph nodes
Delineate and document breast masses
Check for nipple discharge
Identify localized areas of tenderness and relate them to areas of pain noted by the woman and to other physical findings
Women found to have a palpable breast mass, skin changes, or bloody nipple discharge should be referred to a breast specialist for further evaluation and imaging to treat or exclude breast cancer
Chest wall:
Physical exam should also aim at differentiating true breast pain from extramammary pain
Features of breast pain that suggest an extramammary origin include:
Unilateral, and brought on by activity
Located very lateral or medial in the breast
Reproducible by pressure on a specific area of the chest wall
To specifically look for chest wall pain, women may be asked to lie on each side:
These positions enable the breast to fall away from the chest wall, which permits palpation of the underlying chest wall muscles and ribs
Women with pain in the lower aspect of their breast should have the breast elevated with one hand and the underlying chest wall palpated with the other
Chest wall pain due to pectoralis major muscle injury can be reproduced by asking the patient to place her hand flat on the iliac wing and push inward
Women found to have chest wall pain can be reassured that there is no serious underlying cause for the pain, and they can be treated according to the symptoms
Imaging:
For most women who present with breast pain, a thorough history and physical examination must be performed, and clinical judgment must be used in deciding upon any diagnostic imaging studies
Suspicious physical findings present:
Women of any age who have suspicious physical findings such as a mass, skin changes, or bloody nipple discharge should undergo:
Mammography with or without ultrasound
Suspicious physical findings absent:
Assuming they are up to date with breast cancer screening, women who have breast pain but no other suspicious findings on physical exam:
May undergo breast imaging selectively based on their presentation and age
Breast imaging, even with a negative result, has been credited with alleviating patient anxiety
Seeking reassurance is often cited as the main reason for imaging in patients with breast pain
Many women do not seek further medical attention after assurance that their pain is not due to breast cancer
The imaging modalities most commonly used in these clinical scenarios are breast ultrasound and mammography
There are no data to suggest the use of breast magnetic resonance imaging (MRI) for this patient population
In a case-control study, there was no difference in breast cancer incidence in women undergoing mammography for a painful breast (0.5%) compared with the contralateral nonpainful breast (0.5%) and compared with women without breast pain (0.7%)
Three studies of ultrasound for focal breast pain without a palpable mass detected cancer in 0%, 1.2%, and 4.6% of patients
The American College of Radiology Appropriateness Criteria guidelines recommend the following approach to selecting an imaging modality:
Women with cyclical or bilateral nonfocal breast pain:
Usually do not require imaging:
The yield of finding a specific cause with imaging is low
Women with noncyclical, unilateral, or focal breast pain that is not extramammary (eg, chest wall pain), as determined by physical exam:
Should undergo breast imaging to elucidate the underlying etiology and exclude breast cancer
The choice of imaging modality is based on age:
Women under 30 years of age:
Should undergo ultrasound because it is more accurate than mammography for that age group
Mammography is added if abnormality is found on the ultrasound and/or if a patient’s history or risk status justifies the radiation exposure
Women between 30 and 39 years of age:
Should also undergo ultrasound
Unilateral or bilateral mammography should also be performed because in this age group some small cancers are found on mammography but not ultrasound
Women age 40 and older:
Should undergo both mammography and ultrasound
For women who have breast pain but no abnormality on physical examination or imaging studies:
The risk for breast cancer is low at approximately 0.5%
Treatment:
After obtaining normal findings on clinical and imaging studies, reassurance is often all that is required:
A simple assurance that the patient does not have breast cancer provides adequate relief for 78% to 85% of women
Such patients would also benefit from a follow-up visit in two to three months to exclude or treat recurrent/persistent pain
For some women, however, breast pain can cause problems with their activities of daily living:
As an example, in a study of 1171 healthy premenopausal women:
11% reported moderate-to-severe pain that interfered with sexual activity (48%), physical activity (37%), social activity (12%), and school activity (8%):
Consequently, these women required treatment for their breast pain
Approximately 15% of women seen in the breast clinic for breast pain:
Require treatment beyond simple reassurance
Breast pain is treated:
Medically
Breast surgery is not indicated to treat pain:
In the absence of any breast pathology
First-line therapy:
First-line therapy for breast pain is conservative and typically includes:
Reassurance that this is not a malignancy
Physical support
Over-the-counter analgesics
Manipulation of hormone-based medications for those who take them
I prefer to treat with first-line therapy for six months before moving onto one of the second-line therapies:
Which may be more effective but also have more side effects
Some practitioners also endorse therapies such as caffeine abstinence or evening primrose oil (EPO):
Although such therapies have not been proven effective by vigorous placebo controlled trials:
They are generally harmless and may provide relief for some patients
Physical support:
Support garments:
A well-fitting brassiere to better support the breast is widely advocate
The use of a support bra with steel underwire tends to reduce mastalgia in women with pendulous breasts
In addition, use of a “sports bra” during exercise has been shown to reduce pain related to breast movement
Wearing a soft, supportive bra at night stops the breast pulling down on the chest wall, supports tender breast tissues, and helps many women sleep
Women with asymmetric breasts may benefit from specialized fitting to place extra padding on one side, which permits appropriate support of that side without overcompressing the contralateral side
Compresses:
Some women obtain relief from application of warm compresses or ice packs or gentle massage
For those who breast feed:
Ice packs are recommended during the obstructive (prebacterial) phase of puerperal mastitis:
To decrease milk production regionally and thereby relieve ductal intraluminal pressure and subsequent pain
Acetaminophen or NSAID:
Can be used to relieve breast pain
Topical NSAIDs may also be useful:
While the weaker types of topical NSAID (eg, ibuprofen gel) may not be effective in relieving breast pain
Data from randomized trials demonstrated significant improvement in those treated with diclofenac gel with minimal side effects
In the United States (US), two types of topical NSAIDs are available:
Salicylate, the active ingredient in aspirin, is found in Aspercreme and Nuprin
Diclofenac, which has the same active ingredient as the oral NSAID, is available as a patch, gel, or topical solution
Second-line therapy:
Treatment with one of the second-line therapies may be required in patients who still have debilitating breast pain despite first-line therapy for six months
Some physicians prefer to use tamoxifen first because it has fewer side effect than danazol
Treatment with tamoxifen or danazol for one to three months, until either pain subsides or side effects increase
Tamoxifen:
For patients with more severe mastalgia refractory to other treatments, tamoxifen can provide breast pain relief
A meta-analysis of three randomized trials found tamoxifen to be more effective in relieving breast pain than placebo (relative risk 1.92, 95% CI 1.42-2.58)
Tamoxifen is effective at both doses of 20 mg daily and 10 mg daily:
The side effects are significantly reduced at the lower dose
Thus, when used off-label to treat severe mastalgia, tamoxifen is usually given at 10 mg once daily for three months
However, tamoxifen is associated with menopause-like symptoms such as:
Hot flashes:
Vaginal dryness
Joint pain
Leg cramps
It can also increase the risk of:
Blood clots
Strokes
Uterine cancer
Cataracts
Thus, tamoxifen is infrequently used to treat mastalgia
Restricting tamoxifen to the luteal phase of the menstrual cycle has also been suggested to reduce side effects
Danazol:
Is an androgen, and for severe mastalgia, it is usually given at 200 mg once daily
It should be noted that since 2018, the US Food and Drug Administration (FDA) no longer approves the use of danazol for the indication of fibrocystic breast disease
Danazol is effective in relieving breast pain and tenderness:
According to a meta-analysis of four randomized trials against placebo, it resulted in a 20 point mean reduction in pain score on a visual analogue scale (VAS) of 0 to 100
However, the use of danazol is limited by its androgenic effects
At the recommended dose of 200 mg daily, significant proportions of patients reported side effects such as:
Weight gain (30%)
Menstrual irregularity (50%)
Deepening of the voice (10%)
Hot flashes (10%)
Restricting the use of danazol to the luteal phase of the menstrual cycle reduces the side effects without compromising its effectiveness
Women on hormone-based medications:
Postmenopausal hormone therapy that causes breast pain should be decreased or discontinued if at all possible:
This should only be done if breast pain is intolerable and after discussing with the patient the risks and benefits or curtailing hormone replacement therapy
It is not clear whether oral contraceptives cause or relieve cyclical mastalgia:
Decreasing the dose of estrogen in an oral contraceptive regimen can be effective in controlling breast pain
In other studies, oral contraceptives can reduce breast pain severity and duration in some women with cyclical symptoms:
The impact of oral contraceptive pills on breast pain may largely depend on their compositions; alternatively, they may have different effects on different women
Progestogens also improve breast pain symptoms in some women:
While oral and topical (applied to the breast) progesterone did not show benefit in randomized trials:
A vaginal cream of micronized progesterone (4 g of vaginal cream containing 2.5% natural progesterone used from the 19th to the 25th day of the cycle for six cycles) reduced breast pain in 65% of women compared with 22% of controls in a trial
Therapies not proven by randomized trial data:
The role of diet and lifestyle in relieving cyclical breast pain is unclear, with a strong likelihood of a placebo response for many interventions
However, some practitioners feel that some of these treatments (eg, caffeine abstinence and evening primrose oil [EPO]) are worth trying because they are generally harmless and may offer some women pain relief
A low-fat (15% of calories), high complex carbohydrate diet has been effective in some observational studies and small randomized trials:
However, the trials could not be blinded, which may invite a placebo effect
Additionally, such low-fat diets are difficult to maintain beyond a few weeks
Elimination of caffeine has not been effective in controlled trials, although it seems to be helpful in some women
EPO or its active ingredient gamma linoleic acid (GLA) has been studied in multiple randomized trials of breast pain:
Despite early enthusiasm, neither has been shown to be effective beyond the placebo effect
Vitamin E has been shown in multiple randomized trials to be no better than placebo in the treatment of benign breast disease:
Thus, vitamin E should not be prescribed to treat mastalgia
Bromocriptine is a dopamine agonist that inhibits prolactin release:
Although bromocriptine is effective in relieving pain compared with placebo, it is less effective than danazol, and up to 80% of women develop side effects such as headaches and dizziness
Therefore, it is no longer used to treat breast pain
Several other drugs that affect estrogen or prolactin secretion (including bromocriptine and other gonadotropin-releasing hormone [GnRH] agonists) have been studied but are not advocated for use in patients with severe mastalgia, because of unfavorable side effect profiles
Investigational therapies:
Because of the unfavorable side effect profiles of the medications currently used to treat mastalgia (eg, danazol, tamoxifen), there is great interest in developing natural (herbal) products that could relieve breast pain:
However, the benefits of most of these products remain unproven due to a lack of vigorous testing in randomized trials
Phytoestrogens, such as genistein, isoflavones, and soy milk, have been investigated as treatments for breast pain:
Soy milk has been tested against cow milk in a controlled trial, and although an improvement of symptoms was noted in 56% of test subjects versus 10% of controls, the trial was criticized for noncompliance due to the unpalatable taste of the soy milk
Agnus castus, a fruit extract, has significantly lowered visual analogue pain scores against placebo in controlled trials and is well tolerated
Matricaria chamomilla (chamomile) extract has also improved cyclical breast pain on a visual analogue scale compared with placebo in a controlled trial
Chest wall pain:
For women diagnosed with chest wall pain, local heat and analgesics such as acetaminophen or NSAIDs may relieve pain, but most women do not require therapy beyond reassurance that the source of pain is muscle strain or articular
Patients should reduce or cease activities that brought on or aggravated their pain until the pain improves
In severe cases in which the pain is localized but not relieved by over-the-counter pain medications, a trigger point injection with a mixture of a local anesthetic and corticosteroid may bring relief for the patient and can be repeated as necessary
Prognosis:
In general, mastalgia has a natural history of remission and relapse, evidenced by the fact that improvement is seen in as many as 40% of women receiving placebo in randomized trials
The prognosis of women who have breast pain is variable and influenced by the age of onset of pain and whether pain is cyclical or noncyclical:
In one series, cyclical breast pain spontaneously resolved within three months of onset in 20% to 30% of women, but transient relapses were common
In another series, noncyclical breast pain spontaneously resolved in 50% of patients
Relief may be spontaneous or related to a hormonally mediated event:
Such as pregnancy or menopause
Associated conditions:
Breast pain is usually a symptom, not a diagnosis
Although most women who have breast pain will not have any associated conditions, some will, in which case their pain should be treated as a component of the associated condition
Premenstrual syndrome:
Is characterized by the presence of both physical and behavioral (including affective) symptoms that occur repetitively in the second half of the menstrual cycle and interfere with some aspects of the woman’s life
Breast tenderness is one of the common symptoms of PMS
A meta-analysis of 10 randomized trials of selective serotonin reuptake inhibitors (SSRIs) used in women with premenstrual symptoms showed SSRIs to be more effective than placebo at relieving breast pain
Thus, women who have breast pain or tenderness as a component of PMS may benefit from SSRIs
Breast cancer:
The presence of a breast cancer in a patient who presents with only pain is extremely low, ranging from 0.5% to 33.%
Breast pain may occur at the time of presentation of a breast cancer, although the pain is typically associated with adjacent benign, cystic breast tissue rather than the cancer
One caveat in retrospective studies is that recall of breast pain might be increased after the diagnosis of breast cancer
In addition, pain may also occur following the imaging and core biopsy of the cancer rather than being associated with the cancer itself.
Prior breast surgery:
Pain that develops after breast surgery is of a different etiology and treated differently from de novo breast pain
It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
The head and neck surgeon’s work area:
Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:
This is the neurosurgeon field
Among the diagnostic procedures performed by the head and neck surgeon, are the following:
Nasopharyngolaryngoscopy:
Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions
The surgeries most commonly performed by the head and neck surgeon are:
Total or near total thyroidectomies
Hemithryoidectomies (lobectomies)
Comprehensive neck dissections
Selective neck dissections
Maxillectomies:
Total maxillectomy
Subtotal maxillectomy
Infrastructure maxillectomy
Suprastructure maxillectomy
Medial maxillectomy
Mandibulectomy:
Segmental
Marginal
Tracheostomy
Salivary gland surgeries:
Parotid gland operations:
Limited superficial parotidectomy with identification and preservation of the facial nerve
Superficial parotidectomy with identification and preservation of the facial nerve
Near total parotidectomy with identification and preservation of the facial nerve
Total parotidectomy
Submandibular gland resection
Sublingual gland resection
Resection of tumors of the oral cavity:
Glossectomy
Resection of the floor of the mouth tumors
Resection of tumors of the pharynx
Resection of tumors of the larynx
Split-thickness skin grafts
Full-thickness skin grafts
Sentinel lymph node mapping and sentinel lymph node biopsy
Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
The training of the head and neck surgeon includes mastering the following subjects:
Surgical Anatomy
History and Basic Principles of Head and Neck Surgery
Epidemiology, Etiology, and Pathology of Head and Neck Diseases
Diagnostic Radiology of the Head and Neck Region
Tumors of the Scalp, Skin and Melanoma
Eyelids and Orbit
Nasal Cavity and Paranasal Sinuses
Skull Base and Temporal Bone
Lips and Oral Cavity
Pharynx and Esophagus
Larynx and Trachea
Cervical Lymph Nodes
Thyroid and Parathyroid Glands
Salivary Glands
Neurogenic Tumors and Paragangliomas
Soft Tissue Tumors
Bone Tumors and Odontogenic Lesions
Reconstructive Surgery
Oncologic Dentistry and Maxillofacial Prosthetics
Principles of Radiation Oncology
Principles of Chemotherapy
Molecular Oncology, Genomics and Immunology
Nutrition
Biostatistic
My name is Rodrigo Arrangoiz I am a board-certified surgical oncologist who sub-specializes in breast cancer and head and neck cancer. I earned his medical degree at the Anahuac University Medical School in Mexico City, Mexico and graduated Suma Cum Laude. I completed his internship and residency in general surgery at Michigan State University, where he was named chief resident during his fifth year of residency. I also completed a complex surgical oncology, head and neck fellowship at the Fox Chase Cancer Center in Philadelphia and at the same time he undertook a master’s in science (Clinical Research for Health Care Professionals) at Drexel University in Philadelphia. I participated in a two-year global online fellowship in head and neck surgery and oncology through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center.
I have participated in multiple courses and academic congresses as a lecturer and guest professor and has also participated in several publications on topics related to his specialty that include oral cavity cancer, hyperparathyroidism, thyroid cancer, breast cancer, endocrine tumors, squamous cell carcinoma of the head and neck, and more. I am board certified by the American Board of Surgery, the Mexican Board of General Surgery and the Mexican Board of Oncology.
I am a member of various medical associations such as the American College of Surgeons, American Thyroid Association, American Head and Neck Society, American Medical Association, American Society of Clinical Oncology, Association of Academic Surgeons, Society of Surgical Oncology, among others.
In a postmenopausal woman who is not taking hormone therapy:
The new development of a cyst would be uncommon
Diagnostic ultrasound images of nodular density
The lesion contains diffuse internal echoes:
So it is sonographically compatible with a complicated cyst
Low-grade carcinomas, especially ER+ tumors:
Grow slowly enough that one would not expect a mammogram 2 years earlier in such a patient to be completely normal
In addition, a low-grade carcinoma grows slowly enough to allow desmoplasia to occur:
Creating spicules
Low-grade carcinomas are less cellular than high-grade tumors, and have more collagen and less water:
These factors contribute to posterior shadowing:
Especially in lesions 1.5 cm or larger
A high-grade carcinoma:
Grows so rapidly that desmoplasia does not have time to develop
They are more cellular, evoke an inflammatory rather than fibroelastotic response, have more water content, and frequently have cystic or hemorrhagic necrosis:
All of these factors contribute to posterior enhancement rather than shadowing
Triple-negative breast cancer:
Can frequently be confused with a benign lesion on both mammogram and ultrasound due to its unique biological characteristics
Being a highly metabolically active cancer:
Its shape is usually round, oval and/ or lobulated, not spiculated like lower grade breast malignancies, and it often lacks an echogenic rim
As in other high-grade cancers, posterior acoustical enhancement rather than shadowing is seen
Astute sonographers will be able to demonstrate its low elasticity using specialized features on their ultrasound machine or by increasing transducer probe pressure
References
Dogan BE, Tumbull LW. Imaging of triple-negative breast cancer. Ann Oncol. 2012;23(Suppl 6):vi23-vi29
Kojima Y, Tsunoda H. Mammography and ultrasound features of triple-negative breast cancer. Breast Cancer. 2011;18(3):146-151.
Stavros AT. Ultrasound of solid breast nodules: distinguishing benign for malignant. In: Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004:445-527.
Wojcinski S, Soliman AA, Schmidt J, Makowski L, Degenhardt F, Hillemanns P. Sonographic features of triple-negative and non-triple-negative breast cancer. J Ultrasound Med. 2012;31(10):1531-1541.
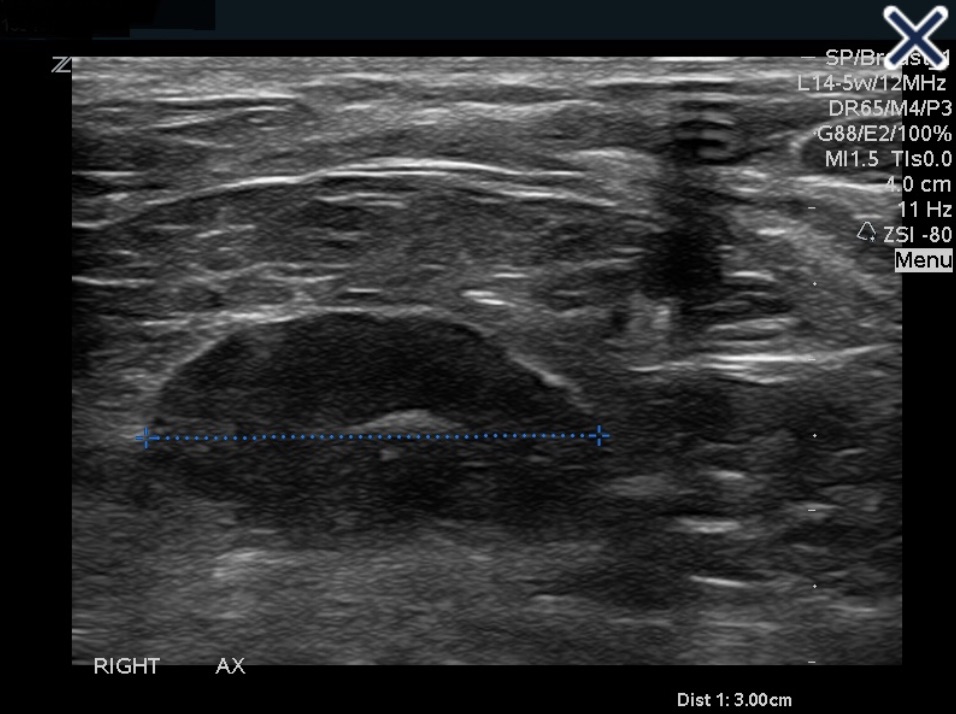
Is elliptical in shape (or bean shaped), and has a narrow, symmetrical, hypoechoic cortex surrounding an isoechoic to hyperechoic fatty hilum (mediastinum)
The cortex of a normal node is composed largely of lymphatic tissue and fluid-filled cortical sinuses:
Thus the hypoechoic echogenicity
The hilum contains alternating medullary cords and sinusoids that have innumerable acoustic interfaces:
Thus the higher degree of echogenicity
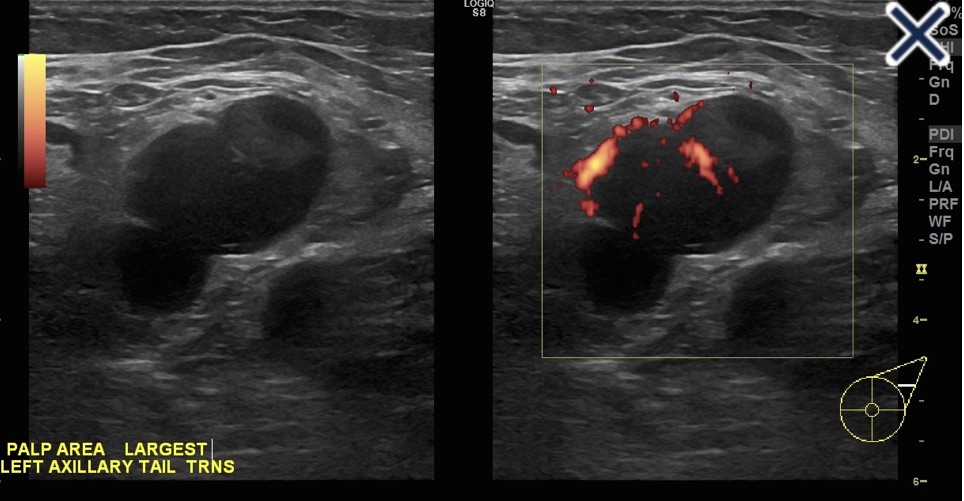
Metastatic Axillary Lymph Node. Another presentation of a metastatic node is an asymmetric cortex where the tumor can be seen invading the hilum with convex indentations that look like “rat bites”Lymph node completely replaced with metastatic carcinoma obliterating the fatty hilum. Doppler shows more than a single blood vessel supplying the node.
When a lymph node is completely replaced with metastatic cancer:
It will be rounded, hypoechoic, and the hilum will be completely obliterated (Image)
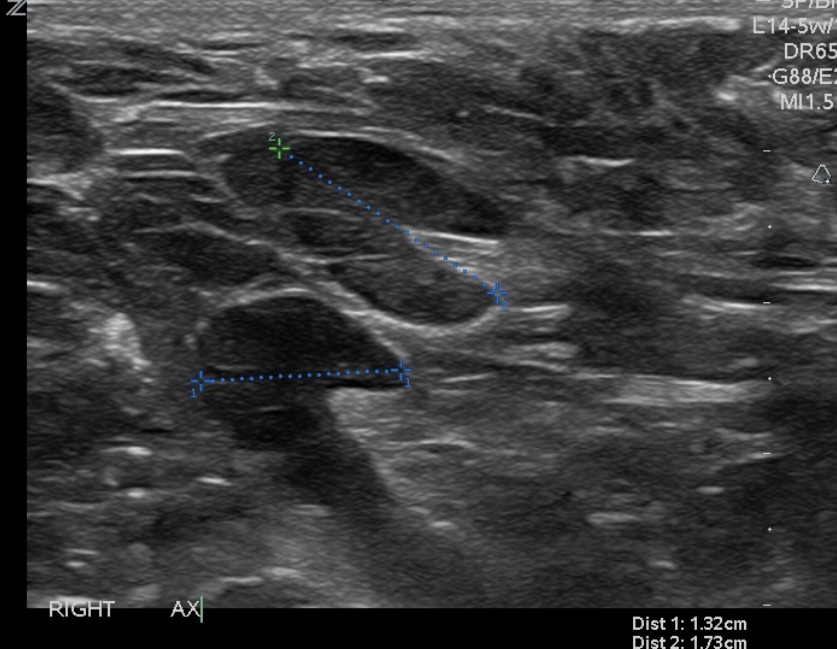
Before the node reaches the stage of complete replacement:
It can have an asymmetric, thickened cortex, with an eccentric hilum (Image)
Another presentation of a metastatic node:
Is an asymmetric cortex where the tumor can be seen invading the hilum with convex indentations that look like “rat bites” (First Image)
A metastatic node can also have severe compression of a central hilum resulting in a slit-like central hyperechoic band (Image)
Severe compression of the hilum by metastatic carcinoma resulting in a “slit-like” central hilumLymph nodes with eccentric hila and asymmetric, thickened cortices.
Reactive nodes can be difficult to distinguish from metastatic nodes (Image)
Reactive node.
In general, benign causes of nodal enlargement:
Tend to thicken the cortex diffusely
In addition, it is not uncommon to have a metastatic node adjacent to a normal node:
But all nodes in a region tend to be reactive when the cause is benign
Finally, a reactive node has blood supply on Doppler examination through a single hilum, whereas metastatic nodes tend to have multiple transcapsular vessels
References
Rahbar H, Partridge SC, Javid SH, Lehman CD. Imaging axillary lymph nodes in patients with newly diagnosed breast cancer. Curr Probl Diagn Radiol. 2012;41(5):149-158.
Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004.
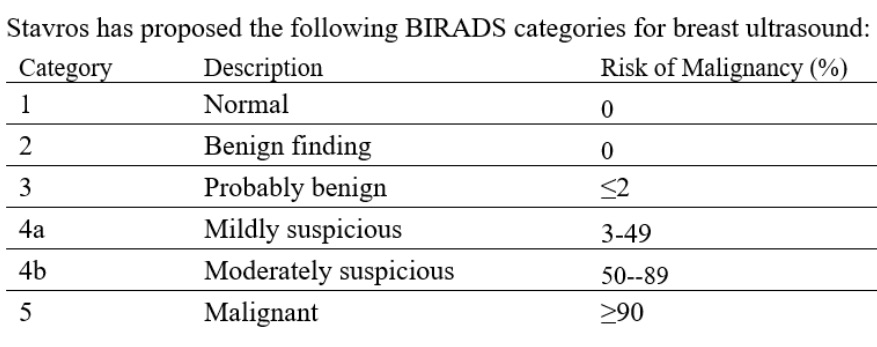
Stavros has proposed the following BIRADS categories for breast ultrasound (see Table 1)
Proposed BIRADS categories for breast ultrasound
The American College of Radiology classification subdivides category 4 into:
BIRADS 4a:
Which has a 2% to 10 % risk of malignancy
BIRADS 4b:
Which has a 10% to 50 % risk
BIRADS 4c:
Which has a 50% to 95% risk
BIRADS 5 has 95% or greater chance of malignancy
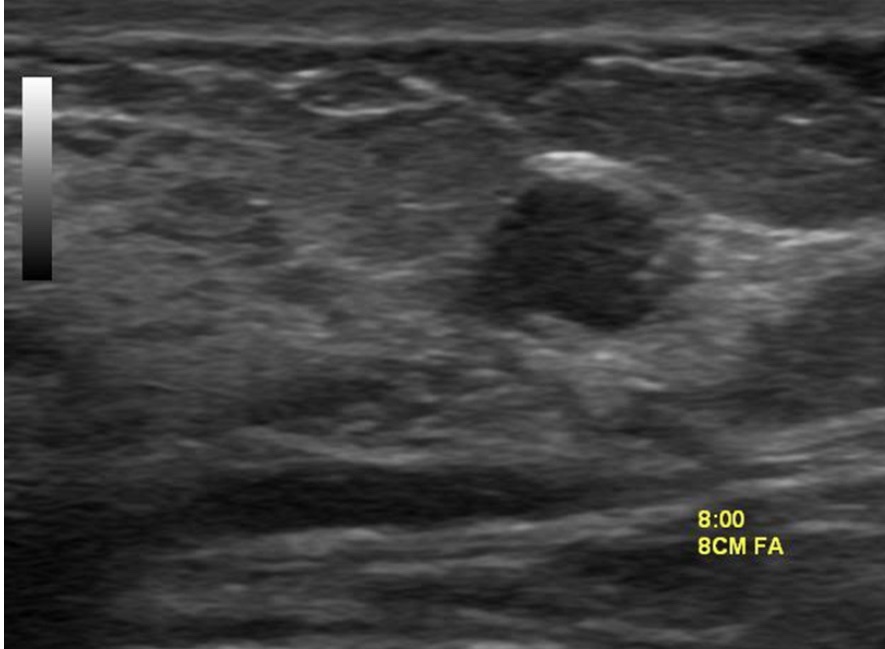
In evaluating a solid sonographic nodule:
One should first look for any of the 10 signs of malignancy:
If even one of them is present:
The lesion cannot be considered BIRADS 3
The 10 signs of malignancy include:
Shadowing
Hypoechoic echotexture
Spiculation
Angular margins
Thick echogenic halo
Microlobulation
Taller than wide
Duct extension
Branching pattern
Calcifications
Note that Stavros compares the echogenicity of lesions to that of breast fat, not breast parenchyma:
Therefore, a lesion with hypoechoic echotexture would be very hypoechoic if breast parenchyma is used as the reference
The hypoechoic lesion in the image does not have smooth margins but appears microlobulated
Regardless of whether the classification of Stavros or the American College of Radiology is used:
The risk of the lesion in this patient is not low enough to be considered BIRADS 3 nor high enough risk to warrant BIRADS 5:
Thus, it falls somewhere in the BIRADS 4 range:
Biopsy is required
References
D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. 5th ed. Reston, VA: American College of Radiology; 2013
Jales RM, Sarian LO, Torresan R, Marussi EF, Alvares BR, Derchain S. Simple rules for ultrasonographic subcategorization of BI-RADS®-US 4 breast masses. Eur J Radiol. 2013;82(8):1231-1235.
Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004.
Women over age 40 with heterogeneously dense breasts or extremely dense breasts:
At average risk for developing breast cancer:
12% to 13% lifetime risk:
Require only annual mammography
The decision to pursue additional imaging in patients with elevated risk should supplement but never entirely replace mammography
Use of screening ultrasound or MRI of the breast are appropriate for women at increased risk:
But the benefit remains to be determined in women of average risk for breast cancer
Breast fibroglandular composition:
Is defined by one of the following four descriptions:
Almost entirely fatty
Scattered areas of fibroglandular density
Heterogeneously dense
Extremely dense
The U.S. population distribution of breast density is as follows:
10% almost entirely fatty
40% scattered areas of fibroglandular density
40% heterogeneously dense
10% extremely dense
Women with heterogeneously dense or extremely dense breasts:
Are considered to have dense breasts:
Sensitivity of mammography decreases as breast density increases
Increased breast density not only has a masking effect, which may obscure masses:
But also serves as an independent risk factor for breast cancer
It has been reported that the increased risk:
May be as much as 4 to 6-fold
Estimates this high are obtained when comparing women with dense breasts to those with fatty replaced breasts
Since only 10% of women have fatty replaced breasts:
It makes more sense to make the comparison with women of average breast density
The relative risk for cancer in women with heterogeneously dense breasts compared with the average woman is approximately 1.2, and the relative risk for cancer in women with extremely dense breasts compared with the average woman is approximately 2.1
In general, breast density decreases with increasing age and increasing body mass index:
So it is not the absolute density that is a risk factor:
But the difference in the observed and expected density
Several states have passed legislation requiring women with dense breasts to be specifically informed of their breast density:
Such women are informed of the limitations of mammography in dense breasts and are instructed to discuss further management with their physicians
An informed decision regarding potential use of supplemental screening options, in addition to mammography, should be discussed, factoring in elements such as overall breast cancer risk as well as the positives and negatives of additional screening, including likelihood of additional benign biopsies
Guidelines for enhanced screening have been developed using lifetime risk calculations as calculated by models stressing family history, such as the Tyrer Cuzick Model, and not purely using breast density
References
1. D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA. ACR BI-RADS® Atlas: Breast Imaging Reporting and Data System, 5th ed. Reston, VA: American College of Radiology; 2013. 2. 3. Freer PE. Mammographic breast density: impact on breast cancer risk and implications for screening. Radiographics. 2015;35(2):302-315.
Brentnall AR, Harkness EF, Astley SM, Donnelly LS, Stavrinos P, Sampson S, et al. Mammographic density adds accuracy to both the Tyrer-Cuzick and Gail breast cancer risk models in a prospective UK screening cohort. Breast Cancer Res. 2015;17(1):147.