My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Current management strategies for primary breast lymphoma:
Are largely based on results published in small, single-institution series
Historically, primary breast lymphoma was treated with:
Modified radical mastectomy with or without adjuvant chemotherapy or radiotherapy
Treatment strategies had focused on:
Anthracycline-based chemotherapy with or without consolidative radiotherapy
Current treatment guidelines dictate that surgery should be reserved for obtaining adequate tissue for diagnosis, if needed, and should not be regarded as a therapeutic modality in the treatment of this disease:
In several series, surgery has been associated with worse outcomes
Some histologies may be amenable to localized surgery so understanding the disease pathology is important in decision making
While axillary nodal status is an important prognosticator:
There are no definitive guidelines regarding how to stage the axilla:
In addition to CT scan, axillary ultrasound with percutaneous biopsy is frequently used
Sentinel lymph node biopsy has not been studied in this malignancy and currently has no role in its workup
References:
Aviles A, Delgado S, Nambo MJ, Neri N, Murillo E, Cleto S. Primary breast lymphoma: results of a controlled clinical trial. Oncology. 2005;69(3):256-260.
Aviv A, Tadmor T, Polliack A. Primary diffuse large B-cell lymphoma of the breast: looking at pathogenesis, clinical issues and therapeutic options. Ann Oncol. 2013;24(9):2236-2244.
el-Ghazawy IM, Singletary SE. Surgical management of primary lymphoma of the breast. Ann Surg. 1991;214(6):724-726.
Jennings WC, Baker RS, Murray SS, et al. Primary breast lymphoma: the role of mastectomy and the importance of lymph node status. Ann Surg. 2007;245(5):784-789.
That represents an aggregation of coherent material
A breast mass:
May be benign or malignant:
A benign mass:
May be solid or cystic
A malignant mass:
Is typically solid
A cystic mass with solid components (complex cyst):
Can also be malignant
Evaluation of a palpable breast mass:
Requires a systematic approach to the history, physical examination, and radiographic imaging studies to ensure a correct diagnosis:
A missed diagnosis of breast cancer is one of the most frequent causes of malpractice claims in the United States
A breast mass:
Can be discovered by the patient incidentally or on routine examination by a patient or clinician:
It is often discovered after a breast examination prompted by other symptoms (eg, pain, nipple discharge) or trauma
On the physical examination:
The palpable breast mass can be obvious or subtle
The density can be soft, firm, or hard
It can be mobile or fixed to the chest wall or skin
It can be tender or nontender
The mass may have well-defined or nondiscrete margins
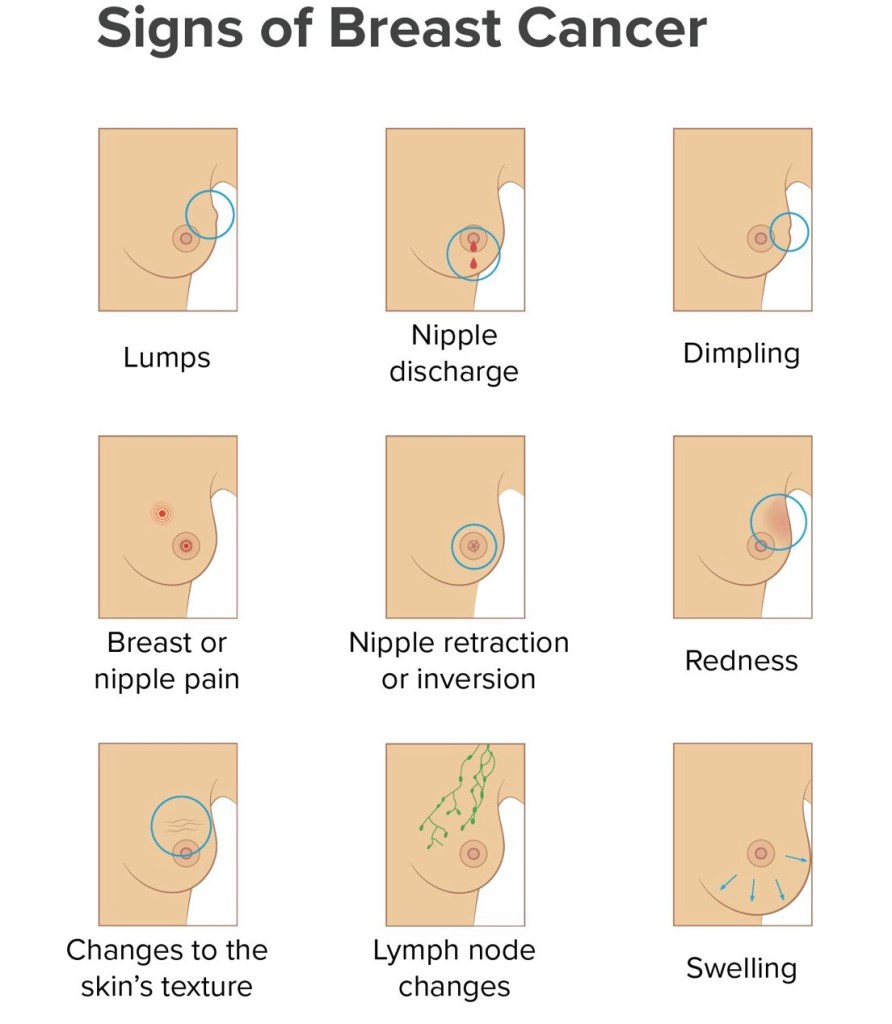
The mass can be associated with clinical findings including:
Ecchymosis
Erythema
Peau d’orange
Skin dimpling
Nipple discharge
Nipple retraction
Often the mass has no associated clinical findings
Multiple epidemiologic studies around the world have reported that:
Breast cancer occurs more frequently in the upper outer quadrant than any other part of the breast:
In a National Cancer Database (NCDB) study of over 2 million women diagnosed with breast cancer between 2004 and 2015:
39.5% had cancer in the upper outer quadrant
Smaller studies reported breast cancer in the upper outer quadrant in 36% to 62% of patients
Although this is most likely secondary to:
The upper outer quadrant having more breast tissue:
There may be differences in genomic instability in this area
The differential diagnosis of a palpable breast mass includes:
Benign and malignant etiologies
Palpable breast masses:
Are very common in women
Most palpable masses are benign:
Approximately 90% or more of palpable breast masses in women in their 20s to early 50s are benign:
However, excluding breast cancer is a crucial step in the assessment of a breast mass in a woman of any age
The following types of masses are among the most common benign breast masses palpated:
Fibroadenoma:
A simple fibroadenoma is a benign solid mass
It typically is identified in young women but can also be identified as a calcified mass in older women
The mass is firm and often mobile
A fibroadenoma may be:
Solitary
Multiple
Bilateral
Cyst:
A simple cyst is a benign, fluid-filled mass:
That can be palpated as a component of fibrocystic changes of the breast or as a discrete, compressible, or ballotable solitary mass
Breast cysts are commonly found in premenopausal, perimenopausal, and occasionally postmenopausal women
Fibrocystic changes:
Fibrocystic changes in the breast are common:
Particularly in premenopausal women
May be prominent and organized:
However, the breast tissue tends to be more diffuse and tender and generally does not form a discrete or well-defined mass
Most patients present with breast pain:
That may be cyclical or constant
May be bilateral, unilateral, or focal
The breast tissue, particularly in the upper outer quadrant:
May increase in size prior to the onset of menses, then return to baseline after the onset of the menstrual flow
On clinical examination:
The breast tissue frequently is nodular
Galactocele:
A galactocele is a milk retention cyst common in women who are breastfeeding
Fat necrosis:
Fat necrosis is a benign breast mass that can develop after:
Blunt trauma to the breast
Injection of native or foreign substances such as:
Fat, paraffin, or silicone
An operative procedure such as breast reductive surgery or autologous breast reconstruction
Radiation therapy to the breast
Fat necrosis from trauma:
Is generally associated with skin ecchymosis
Fat necrosis can often be clinically and even radiographically difficult to distinguish from a malignant mass
Breast abscess:
A breast abscess is a localized collection of inflammatory exudate (ie, pus) in the breast tissue
Primary breast abscesses:
Develop when mastitis or cellulitis is left untreated or does not respond to antibiotic treatment
Patients with primary breast abscess present with:
Localized, painful inflammation of the breast associated with fever and malaise, along with a fluctuant, tender, palpable mass
The diagnosis is established via ultrasonography demonstrating a fluid collection
Malignant:
The differential diagnosis of a malignant breast mass includes:
Multiple invasive and noninvasive cancers
The following types of masses are among the most common malignant breast masses palpated:
The most common breast cancer is an infiltrating ductal breast carcinoma:
This invasive histology accounts for approximately 70% to 80% of invasive breast cancers
Other invasive breast cancers include infiltrating lobular carcinoma and mixed ductal / lobular carcinoma:
Infiltrating lobular carcinoma often presents as a prominent diffuse thickening of the breast rather than as a discrete mass
There are also variants of the invasive ductal carcinomas that can be detected as a palpable mass
Rarely, noninvasive cancers (ductal carcinoma in situ [DCIS]) with or without microinvasion can develop into a palpable breast mass
The clinical evaluation of a palpable breast mass begins with a complete history and physical examination:
Although some radiographically identified masses may not be palpable, the same clinical evaluation also applies
History:
The history should include a:
Full review of medical and surgical illnesses, medications, and allergies and an assessment of risk factors for breast cancer, such as a detailed family history
In addition, for masses identified by the patient, subjective information about how and when the mass was first noted, if it is painful, and how it has changed over time should be recorded
The history of presenting symptoms includes:
Any change in the general appearance of the breast, such as an increase or decrease in size or a change in symmetry
New or persistent skin changes
New nipple inversion
If nipple discharge is present, whether it is bilateral, unilateral, or from one specific duct
Other important information includes the timing, color, frequency, and spontaneity of the discharge
The characteristics of any breast pain, the relationship of symptoms to menstrual cycles (cyclic or noncyclic), the location within the breast (or both breasts), the duration, and whether it is aggravated or alleviated by any activities or medications
The presence of a breast mass and its evolution, including how it was first noted (accidentally, by breast self-examination, clinical breast examination, or mammogram), how long it has been present, and whether it has changed in size
The precise location of any breast mass
Whether a mass waxes and wanes during the menstrual cycle:
Benign cysts may be more prominent premenstrually and regress in size during the follicular phase
Trauma to the breast (eg, car accident with seat belt, direct injury from a hard object) may result in a breast mass due to the development of fat necrosis or a hematoma
In addition, trauma may be the precipitating event to detection of an existing benign or malignant mass:
Any mass after a trauma that fails to resolve will require a complete evaluation
Risk factors for breast cancer:
A thorough risk assessment is part of the evaluation of women with breast complaints, and significant negative as well as positive findings should be documented in the medical record
Physical examination:
The breast examination includes both breasts and the nodal basins of the neck, chest wall, and both axillae and is part of a complete physical examination:
Inspection – The patient should be examined in both the upright and supine positions. The patient must be disrobed from the waist up, allowing the examiner to visualize and inspect the breasts
The breast examination is started with the patient in a seated position with her arms relaxed
The patient is then asked to raise her arms over her head so the lower part of the breasts can be inspected
Finally, the patient should put her hands on her hips and press in to contract the pectoral muscles so that any other areas of retraction can be visualized
Inspection of the breast includes:
Asymmetry – Observe the breast outline and contour for any bulging areas
Skin changes – Check for dimpling or retraction, edema, ulceration, erythema, or eczematous appearance, such as scaly, thickened, raw skin
Nipples – Assess for symmetry, inversion or retraction, nipple discharge, or crusting
Palpation – After careful inspection, proceed with the palpation of regional lymph nodes and the breasts
Regional lymph node examination – While the patient is sitting, the regional lymph nodes are examined, with attention to the cervical, supraclavicular, infraclavicular, and axillary nodal basins:
The best examination of the axillary nodes requires that the patient relax her shoulders and allow the examiner to support her arm while the axilla is palpated
This allows relaxation of the latissimus and pectoralis muscles for ease in palpating high into the axilla
It is important to note the presence of any palpable nodes and their characteristics, whether they are soft and mobile or firm, hard, tender, fixed, or matted
Breast examination – A bimanual examination of the breasts is performed while the patient is still in the sitting position, supporting the breast gently with one hand and examining the breast with the other hand
The examination is completed with the patient in a supine position, with the ipsilateral arm raised above her head:
This allows the examiner to flatten the breast tissue against the patient’s chest
It is sometimes useful to have the patient roll onto her contralateral hip to flatten the lateral part of the breast
The entire breast must be examined, including the breast tissue that comprises the axillary tail of Spence, which extends laterally toward the axilla
To be sure that all breast tissue is included in the examination, it is best to cover a rectangular area bordered by the clavicle superiorly, the midsternum medially, the midaxillary line laterally, and the lower rib cage inferiorly
The examination technique should be systematic, using concentric circles, a radial approach, or vertical strips
Palpation should be done with the finger pads rather than the fingertips
Circular motions with light, medium, and deep pressure ensure palpation of all levels of breast tissue
One hand stabilizes the breast while the other hand is used to perform the examination
Documentation:
The location of the mass as well as any abnormality found on examination should be accurately documented
The size of any mass should be measured in centimeters and its location, mobility, and consistency recorded
It is helpful to record the location of any abnormality by documenting both the position on the breast and the distance in centimeters from the areola:
In this manner, the precise location can be easily identified on subsequent follow-up examinations by the initial examiner as well as other practitioners
The “clock” system can be used for documentation, comparing the breast to a clock and using the location on the clock to indicate the location of a lesion (eg, 1 o’clock position)
The entire examination should be clearly and completely documented in detail, including significant negatives, even if it is completely normal. Distance from the nipple or from the radial edge of the areola can be used to document location of the mass
Timing of examination:
In premenopausal patients:
The breast examination is best performed when hormonal stimulation of the breasts is minimized:
Which is usually seven to nine days after the onset of menses in premenopausal women:
However, the evaluation of a clinically suspicious mass should not be influenced by the phase of the menstrual cycle
Accuracy of examination :
The physical examination of patients with benign breast disease parallels the examination of patients with cancer since normal breast tissue in women is often somewhat nodular
The first goal of the physical examination is to determine whether a dominant mass, thickening, or asymmetry is present:
This is particularly important in younger women, whose breasts are more likely to be generally nodular than older women:
In a retrospective review of 605 women under the age of 40 years who were referred to a breast clinic for evaluation of a breast mass:
A dominant mass was palpated by the surgeon in 36% of self-detected masses (n = 484) and 29% of clinician-detected masses (n = 121)
However, the physical examination findings cannot always distinguish between a benign mass and a malignancy, even for clinical experts, as the findings may be subtle
Studies that have examined the usefulness of the physical examination for diagnosing benign versus malignant breast masses have found that clinicians can often make the right diagnosis but are not perfect:
In one report, from a study of symptomatic women, experienced examiners who diagnosed “definite cancer” on palpation were correct in 93% of cases
In another series, the physical examination had a positive predictive value of 73% and a negative predictive value of 87%
Diagnostic evaluation:
Imaging options include diagnostic mammography, including tomosynthesis where available, and targeted breast ultrasound, the choice of which depends on patient age and the degree of clinical/radiologic suspicion
There is little role for advanced imaging modalities such as breast magnetic resonance imaging
The diagnosis of a benign or malignant breast mass is confirmed by a breast biopsy:
The definitive diagnosis of a benign or malignant breast mass is based upon the histopathology from a core, incisional, or excisional tissue biopsy or a fine needle aspiration (cytologic evaluation)
The appropriate interval of follow-up for patients with benign biopsy is controversial and depends on the histology:
Although various intervals (four or six months) have been proposed, no evidence-based guidelines are available to aid this decision
For patients with a benign biopsy:
I suggest repeating clinical examination and imaging every six months for two years, and if stable, patients may return to routine screening after that
Biopsy-proven benign masses that change clinically or radiographically, such as increasing in size on follow-up examinations, should be reevaluated and excised.
Whether a short follow-up interval is necessary has been questioned:
A study using the Breast Cancer Surveillance Consortium (BCSC) registry compared cancer detection rates and stage for patients with short-interval follow-up (three to eight months) with those who returned to routine screening (9 to 18 months) following benign core breast biopsy (stereotactic or ultrasonography guided):
A total of 17,631 biopsies with benign findings were identified
Similar cancer detection rates were found for the short-interval follow-up and routine screening groups with no significant differences in stage, tumor size, or nodal status
Thus, it may be safe for those with a benign radiologic-pathologic-concordant percutaneous breast biopsy to return to routine screening
However, the study did not identify the spatial relationship between the finding that prompted the initial biopsy and the site of the subsequent cancer (which could have represented a false-negative result)
Which manifests as axillary lymph node metastasis without the evidence of a primary breast tumor on clinical examination or mammography:
Accounts for 0.3% to 1.0% of all breast cancers
The American College of Radiology:
Recommends the use of MRI for occult breast cancer patients:
Who do not have evidence of a breast primary on traditional radiological examination (mammogram and ultrasound) and clinical examination:
Level I evidence has shown MRI is significantly more sensitive in detecting a primary lesion than mammography or ultrasound:
Identifying a primary tumor in 72% of cases that were originally deemed occult
Patients with occult breast cancer who have abnormalities demonstrated on MRI:
Should then undergo evaluation with targeted ultrasound plus ultrasound-guided needle biopsy or MRI-guided needle biopsy and receive treatment according to the clinical stage of the breast cancer
Treatment recommendations for those with negative MRI results and occult breast cancer presenting as isolated axillary metastases:
Are based on nodal status and breast cancer subtype
Most patients with axillary metastasis from an unknown breast primary:
Are candidates for neoadjuvant therapy
A meta-analysis reported outcomes for occult breast cancer in patients undergoing axillary lymph node dissection (ALND) (with or without radiation therapy [RT]) versus mastectomy:
It included 7 international studies, with 241 patients presenting between 1973 and 2011
The mean follow up was 62 months
There was no difference in survival, locoregional recurrence rate, or distant metastatic rate:
Between those occult breast cancer patients who underwent mastectomy versus those who underwent ALND + breast RT (without breast surgery):
Radiotherapy improves locoregional recurrence and possibly mortality rates of patients undergoing ALND
Based on this meta-analysis, combined ALND and RT is an acceptable approach
The current National Comprehensive Cancer Network guidelines:
Recommend that patients with negative MRI results should be treated with mastectomy plus axillary lymph node dissection (modified radical mastectomy) OR ALND plus whole-breast irradiation
Approximately 40% of patients undergoing neoadjuvant chemotherapy for clinically node-positive disease:
Are successfully down staged in the axilla, and may be able to avoid ALND:
Although this may prove to be safe for patients with primary occult breast cancer, there are no studies that have specifically addressed the safety of sentinel lymph node biopsy with targeted axillary dissection in this highly select subset:
Treatment gold standard for occult breast cancer presenting with axillary metastases which remain clinically positive after neoadjvuant chemotherapy, remains ALND
References
Ge L-P, Liu X-Y, Xiao Y, et al. Clinicopathological characteristics and treatment outcomes of occult breast cancer: a SEER population-based study. Cancer Manag Res. 2018;10:4381-4391. doi: 10.2147/CMAR.S169019
Ofri A, Moore K. Occult breast cancer: where are we at? Breast. 2020;54:211-215. doi: 10.1016/j.breast.2020.10.012
de Bresser J, de Vos B, van der Ent F, Hulsewé K. Breast MRI in clinically and mammographically occult breast cancer presenting with an axillary metastasis: a systematic review. Eur J Surg Oncol. 2010;36(2):114-119. doi: 10.1016/j.ejso.2009.09.007
Macedo FIB, Eid JJ, Flynn J, Jacobs MJ, Mittal VK. Optimal surgical management for occult breast carcinoma: a meta-analysis. Ann Surg Oncol. 2016;23(6):1838-1844. doi: 10.1245/s10434-016-5104-8
Contralateral mastectomy (CM) can be considered in:
Patients who have a high risk of contralateral breast cancer:
Due to:
A germline mutation
Prior chest irradiation
Strong family history
CM is contraindicated in:
Patients with comorbidities in whom the increased risk of surgical complications and / or the longer time under general anesthesia may be detrimental to their health
CM should be discouraged in:
Patients with metastatic disease:
Even if a palliative unilateral mastectomy is being considered
Patients with oligometastatic disease in whom a unilateral mastectomy, as recommended by a multidisciplinary care team or as part of a clinical trial:
Is being performed for curative intent
Patients with locally advanced breast cancer or inflammatory breast cancer:
For whom the expeditious delivery of adjuvant therapy may impact outcomes
Patients whose main reason for choosing CM is improving survival or decreasing the risk of a recurrence of their index cancer:
Despite proper counseling
Patients with a significant competing risk of mortality secondary to their breast cancer, other malignancies, or comorbidities
Is a rare complication of longstanding lymphedema.
Clinical suspicion should be high:
As this syndrome is easily misdiagnosed and treatment is advertently delayed
Once diagnosed:
Surgical excision is the treatment of choice:
Sometimes requiring forequarter amputation
Chemotherapy may have some role:
However its benefit is unclear.
Multiple studies have shown the 5-year survival to be very poor:
At less than 10%.
The mean survival is 20 months.
References
Cui L, Zhang J, Zhang X, et al. Angiosarcoma (Stewart-Treves syndrome) in postmastectomy patients: report of 10 cases and review of literature. Int J Clin Exp Pathol. 2015;8(9):11108-11115.
Penel N, Bui BN, Bay JO, et al. Phase II trial of weekly paclitaxel for unresectable angiosarcoma: the ANGIOTAX Study. J Clin Oncol. 2008;26(32):5269-5274.
The average time from radiation to presentation is:
10 years
The mainstay of treatment remains:
Surgical excision with negative margins:
However, local recurrence and distant recurrence remains quite high, and close monitoring is recommended
The role of chemotherapy is unclear:
Therefore, surgery should remain the primary treatment of choice
Preoperative radiation with hyperfractionated and accelerated radiation therapy:
Has also been identified as a potential alternative to surgery alone, with improved survival and should be considered
More trials are needed to improve outcomes for this aggressive but rare complication of radiation
References
Torres, K.E., Ravi, V., Kin, K. et al. Long-term outcomes in patients with radiation-associated angiosarcomas of the breast following surgery and radiotherapy for breast cancer. Ann Surg Oncol.2013;20(4):1267-1274.
Palta M , Morris CG, Grobmyer SR, Copeland EM, Mendenhall NP. (2010), Angiosarcoma after breast‐conserving therapy. Cancer. 116(8):1872-1878.
Smith TL, Morris CG, Mendenhall NP. Angiosarcoma after breast-conserving therapy: long-term disease control and late effects with hyperfractionated accelerated re-irradiation (HART). Acta Oncol. 2014;53(2):235-241.
Penel N, Bui BN, Bay JO, et al. Phase II trial of weekly paclitaxel for unresectable angiosarcoma: the ANGIOTAX Study. J Clin Oncol. 2008;26(32):5269-5274.
Palta M, Morris CG, Grobmyer SR, Copeland EM 3rd, Mendenhall NP. Angiosarcoma after breast-conserving therapy: long-term outcomes with hyperfractionated radiotherapy. Cancer. 2010;116(8):1872-1878.
Axillary sentinel node biopsy has been shown to be feasible for axillary staging:
In patients with in-breast recurrence or ipsilateral breast second primary tumors
Limited prior axillary sampling (less than 9 nodes) has been shown to have greater success in localization
Preoperative lymphoscintigraphy:
Should be considered given the possibility of aberrant lymphatic drainage due to alterations secondary to prior surgery and radiation
References
Tokmak H, Kaban K, Muslumanoglu M, Demirel M, Aktan S. Management of sentinel node re-mapping in patients who have second or recurrent breast cancer and had previous axillary procedures. World J Surg Oncol. 2014;12:205.
Kothari MS, Rusby JE, Agusti AA, MacNeill FA. Sentinel lymph node biopsy after previous axillary surgery: a review. Eur J Surg Oncol. 2012;38(1):8-15.
It is much less likely to have nodal involvement and is more common in postmenopausal women:
With a mean age of 66
Distant metastases are rare:
However, the lung is the most common site
It has a better prognosis than infiltrating ductal triple negative breast cancer:
With a 5-year overall survival rate of 88%.3
References
Treitl D, Radkani P, Rizer M, El Hussein S, Paramo JC, Mesko TW. Adenoid cystic carcinoma of the breast, 20 years of experience in a single center with review of literature. Breast Cancer. 2018;25(1)28-33.
Welsh JL, Keeney MG, Hoskin TL, et al. Is axillary surgery beneficial for patients with adenoid cystic carcinoma of the breast? J Surg Oncol. 2017;116(6):690-695.
Kulkarni N, Pezzi CM, Greif JM, et al. Rare breast cancer: 933 adenoid cystic carcinomas from the National Cancer Data Base. Ann Surg Oncol. 2013;20(7):2236-2241
In the last 10 years there has been a significant focus on the role of contralateral prophylactic mastectomy and the risk of contralateral breast cancer
Single-institution studies and Surveillance, Epidemiology, and End Results program (SEER) data:
Have found contralateral prophylactic mastectomy rates to be as high as 25%:
Which continue to increase
Further, this trend seems to be limited to the United States
Nichols et al:
Reviewed rates of contralateral breast cancer between 1976 and 2006 using the SEER database
Overall, they found the rate of contralateral breast cancer to be declining:
Approximately 3% per year since 1985
From 1990 forward, they found this benefit to be restricted to those presenting with an ER+ breast cancer:
With annual incidence rates of contralateral breast cancer of 0.25% to 0.37%:
When the index cancer was diagnosed after age 30 years
The rates of contralateral breast cancer were higher in patients with ER– negative breast cancers:
But still remained reasonably low with annual incidence rates of contralateral breast cancer of 0.45% to 0.65% when the index cancer was diagnosed after age 40 years
The use of adjuvant endocrine therapy:
Has contributed to this decline as it reduces the risk of contralateral breast cancer by approximately 50%
Contralateral prophylactic mastectomy:
Is attributed with approximately a 90% to 94% overall reduction in the risk of contralateral breast cancer:
Not 100%
Contralateral prophylactic mastectomy:
Does not improve overall survival:
Recent modeling suggests the added absolute benefit of contralateral prophylactic mastectomy to overall survival:
Is less than 1.45%
The American Society of Breast Surgeons published a consensus statement with indications and suggestions for patient management and decision making with regard to contralateral prophylactic mastectomy:
Discouraging the procedure for women with unilateral breast cancer at average risk for contralateral cancer
References
Nichols HB, Berrington de Gonzalez A, Lacey JV, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564-1569.
Early Breast Cancer Trialists’ Collaborative Group, Davies C, Godwin J, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771-784.
King TA, Sakr R, Patil S, et al. Clinical management factors contribute to the decision for contralateral prophylactic mastectomy. J Clin Oncol. 2011;29(16):2158-2164.
Metcalfe K, Lynch HT, Ghadirian P, et al. Contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2004;22(12):2328-2335.
Portschy PR, Kuntz KM, Tuttle TM. Survival outcomes after contralateral prophylactic mastectomy: a decision analysis. J Natl Cancer Inst. 2014;106(8).
Boughey JC, Attai DJ, Chen SL, et. al.. Contralateral prophylactic mastectomy consensus statement from the American Society of Breast Surgeons: additional considerations and a framework for shared decision making. Ann Surg Oncol. 2016 Oct;23(10):3106-3111.