My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Failure to identify a parathyroid gland during cervical exploration:
Is most commonly explained by:
Ectopic location rather than true absence
Large anatomic and surgical series demonstrate that approximately 15% to 16% of parathyroid glands are ectopic:
With predictable distributions:
Based on embryologic origin (Taterra et al., Surg Radiol Anat, 2019):
Consequently, a structured search strategy:
Guided by embryology and prevalence data is recommended
General intra-operative principles:
Careful inspection of the orthotopic field:
Is mandatory before declaring a gland ectopic
Approximately 80% to 90% of parathyroid glands are located within a few millimeters of the posterior thyroid capsule (Taterra et al., 2019):
Gentle subcapsular dissection along the posterior surface of the thyroid should be completed before expanding the field
Intrathyroidal parathyroid glands:
Account for 2% to 3% of all glands and up to 20% to 22% of ectopic glands, particularly inferior glands (Phitayakorn & McHenry, Am J Surg, 2006):
For this reason, inspection and palpation of the thyroid specimen is considered standard practice in experienced centers (Noussios et al., Exp Clin Endocrinol Diabetes, 2012)
Reoperative series demonstrate that most “missed” glands:
Are found in standard embryologic locations:
Most commonly the tracheoesophagealgroove, thyrothymic ligament, or superior mediastinum:
Emphasizing the importance of a systematic rather than random exploration (Silberfein et al., Arch Surg, 2010)
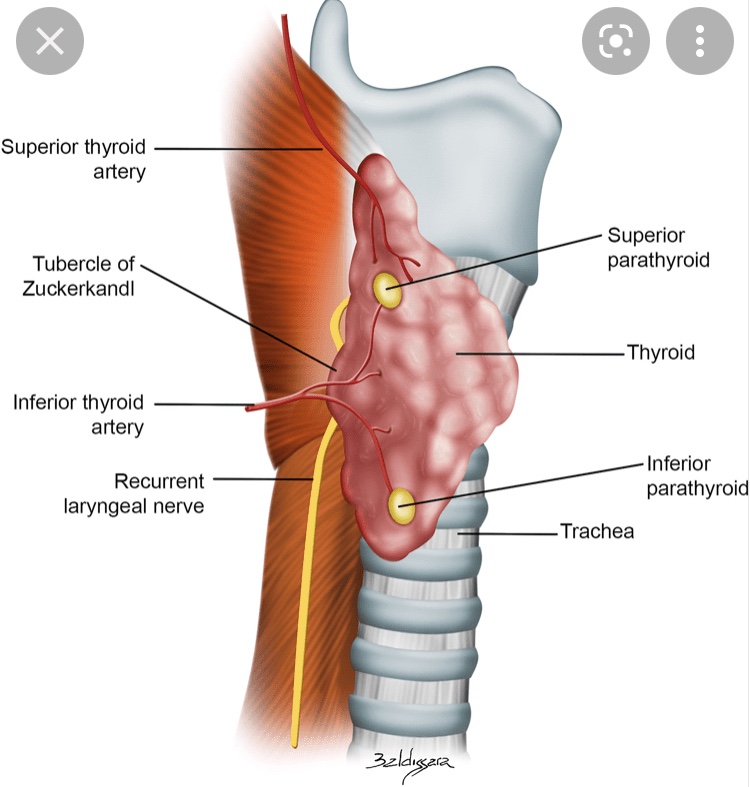
Superior parathyroid gland – Evidence-Based search pattern:
Typical location:
Superior parathyroid glands:
Fourth pharyngeal pouch origin:
Exhibit limited migration and are therefore relatively constant in position
They are typically located on the posterior aspect of the upper thyroid pole:
Approximately 1 cm above the intersection of the recurrent laryngeal nerve (RLN) and the inferior thyroid artery:
Frequently within the tracheoesophageal groove (Scharpf et al., Surg Oncol Clin N Am, 2016)
Common ectopic locations:
When ectopic:
Superior parathyroid glands are most often displaced posteriorly, rather than inferiorly:
Tracheoesophageal or para-esophageal groove the most common ectopic site for superior glands (Noussios et al., 2012; Taterra et al., 2019)
Retro-esophageal or retro-pharyngeal space, particularly in undescended glands (Scharpf et al., 2016)
Posterior mediastinum, where enlarged glands may descend along the esophagus but remain posterior in relation to the RLN (Phitayakorn & McHenry, 2006)
Stepwise surgical approach:
If a superior gland is not identified in its orthotopic location, the recommended sequence is:
Systematic exploration of the tracheoesophageal groove following the RLN superiorly
Blunt dissection of the para- and retro-esophageal spaces
Evaluation of the high posterior neck for undescended glands
Inspection of the thyroid specimen for an intrathyroidal gland (Noussios et al., 2012; Silberfein et al., 2010)
Descend with the thymus and demonstrate significantly greater variability
Orthotopically, they are most often located near the lower thyroid pole, anterior to the RLN, frequently within or adjacent to the thyrothymic ligament (Scharpf et al., 2016)
Common ectopic locations:
Inferior glands account for the majority of ectopic parathyroids:
Intrathymic or within the cervical thymus:
Approximately 30% of ectopic inferior glands (Phitayakorn & McHenry, 2006)
Anterosuperior mediastinum, often contiguous with thymic tissue (Noussios et al., 2012)
Intrathyroidal:
Accounting for ~ 20% to 22% of ectopic inferior glands (Phitayakorn & McHenry, 2006)
High cervical or carotid sheath locations, representing failed embryologic descent (Noussios et al., 2012)
Stepwise surgical approach:
When an inferior gland is not identified at the lower pole:
The thyrothymic ligament should be followed inferiorly toward the thymus
A limited cervical thymectomy should be performed when clinically appropriate:
Given the high incidence of intrathymic glands
The lower thyroid pole and specimen should be inspected for intrathyroidal tissue
The carotid sheath and high cervical region should be explored in cases suspicious for undescended glands (Phitayakorn & McHenry, 2006; Silberfein et al., 2010)
Lessons from re-operative surgery:
In contemporary re-operative parathyroidectomy series, previously missed glands were most commonly located in the:
Tracheoesophageal groove
Thyrothymic ligament
Superior mediastinum
Confirming that failure is usually related to incomplete exploration of predictable embryologic sites rather than unusual anatomy (Silberfein et al., Arch Surg, 2010)
Key references:
Taterra D, et al. The prevalence and anatomy of parathyroid glands: a meta-analysis. Surg Radiol Anat. 2019.
Phitayakorn R, McHenry CR. Incidence and location of ectopic abnormal parathyroid glands. Am J Surg. 2006;191:418–423.
Noussios G, et al. Ectopic parathyroid glands and their anatomical, clinical and surgical implications. Exp Clin Endocrinol Diabetes. 2012.
Silberfein EJ, et al. Reoperative parathyroidectomy: location of missed glands. Arch Surg. 2010.
Scharpf J, et al. Anatomy and embryology of the parathyroid glands. Surg Oncol Clin N Am. 2016.
Anaplastic thyroid cancer (ATC) is rare (<2%) but represents the most aggressive form of thyroid cancer. It behaves very differently from other thyroid cancers and requires urgent, multidisciplinary care.
🧠 Key characteristics of ATC
Rapidly growing neck mass Often presents with hoarseness, difficulty swallowing, or breathing problems Frequently diagnosed at an advanced stage Can arise from pre-existing differentiated thyroid cancer
🔍 How is ATC diagnosed?
Clinical suspicion due to rapid growth Imaging (CT/MRI) to assess airway and invasion Core needle biopsy or surgical biopsy for confirmation Molecular testing (e.g., BRAF V600E) to guide targeted therapy
⚖️ How is ATC treated?
Management requires a multidisciplinary approach:
Airway protection is often the first priority Surgery when feasible Radiation therapy and systemic therapy Targeted therapy and immunotherapy have significantly improved outcomes in selected patients
📈 Prognosis
Historically poor Modern targeted therapies have changed the landscape, improving survival in carefully selected patients Early referral to specialized centers is critical
🦋 ATC is a medical emergency—time matters.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Anaplastic thyroid cancer is aggressive, but early recognition and modern therapies are improving outcomes.
📚 References
Smallridge RC et al. ATA Guidelines for Anaplastic Thyroid Cancer. Thyroid Bible KC et al. Targeted therapy in ATC. NEJM NCCN Guidelines: Thyroid Carcinoma
ADH and atypical lobular hyperplasia (ALH) are now frequently diagnosed with use of core-needle biopsy
Although atypia can be difficult to distinguish from carcinoma in situ:
Pathologic criteria exist to distinguish the two entities
This distinction is important because, while in situ carcinoma is malignant and may progress to invasive disease:
ADH is a non-obligate cancer precursor and often represents a marker of an elevated future breast cancer risk
ADH is most frequently found by mammography
Atypia alone, with no other risk factors, confers an approximate:
Four-fold to five-fold risk of the development of breast cancer
Although breast MRI is more sensitive to detect intermediate- and high-grade ductal carcinoma in situ (DCIS) as well as invasive cancers:
Breast MRI lacks sufficient diagnostic ability to differentiate ADH versus DCIS or invasive cancers
Excision is indicated for ADH found on core needle biopsy:
As concomitant in situ or invasive cancer will be found in approximately 15% of cases (15% to 30% in some series)
The 10-year risk of developing a breast cancer after a diagnosis of ADH:
Is approximately 17%:
Risk is bilateral:
Breast cancers developing within 5 years of a biopsy of ADH more likely to occur in the ipsilateral breast than those developing more than 5 years (82% ipsilateral in the first 5 years vs 58% ipsilateral after 5 years)
The National Surgical Adjuvant Breast and Bowel Project (NSABP) P-1 trial:
Showed that when atypia is found on a sample obtained with needle biopsy and excision rules out cancer:
Tamoxifen reduces the risk of developing breast cancer by about 86%:
These patients should therefore be referred for discussion about this endocrine prophylaxis
Similarly, the Study of Tamoxifen and Raloxifene (STAR, NSABP P-2) trial:
Which randomized post-menopausal women to tamoxifen or raloxifene, found that raloxifene provided equivalent risk reduction to tamoxifen with less toxicity (e.g., endometrial cancer)
References:
Coopey SB, Mazzola E, Buckley JM, et al. The role of chemoprevention in modifying the risk of breast cancer in women with atypical breast lesions. Breast Cancer Res Treat. 2012;136:627-633.
Heller SL, Moy L. Imaging features and management of high-risk lesions on contrast-enhanced dynamic breast MRI. AJR Am J Roentgenol. 2012;198:249-255.
Krishnamurthy S, Bevers T, Kuerer H, Yang WT. Multidisciplinary considerations in the management of high-risk breast lesions. AJR Am J Roentgenol. 2012;198:W132-140.
Hartmann LC, Radisky DC, Frost MH, et al. Understanding the premalignant potential of atypical hyperplasia through its natural history: a longitudinal cohort study. Cancer Prev Res (Phila). 2014;7:211-217.
Vogel VG, Costantino JP, Wickerham DL, et al; National Surgical Adjuvant Breast and Bowel Project. Update of the National Surgical Adjuvant Breast and Bowel Project Study of Tamoxifen and Raloxifene (STAR) P-2 Trial: Preventing breast cancer. Cancer Prev Res (Phila). 2010;3:696-706.
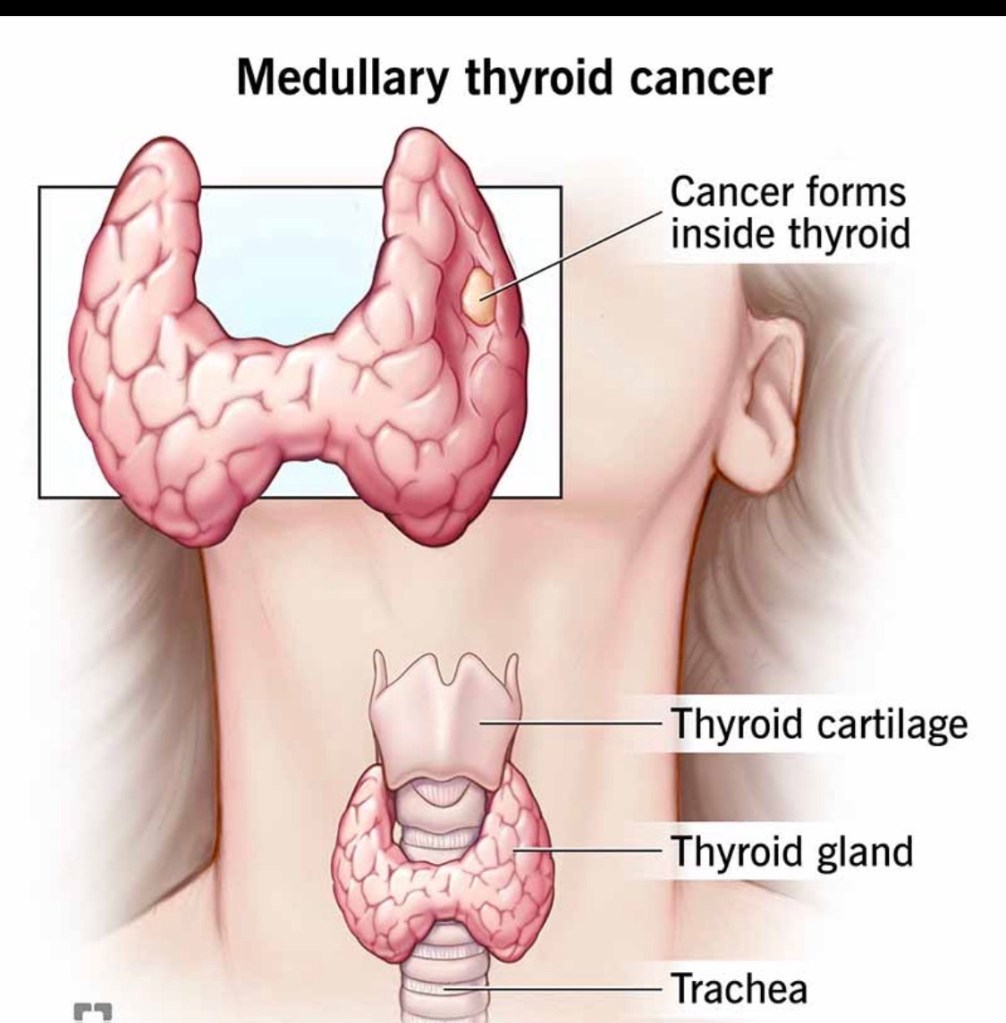
Medullary thyroid cancer (MTC) accounts for ~2–4% of all thyroid cancers and is biologically distinct from papillary and follicular thyroid cancers.
🧠 What makes MTC different?
Arises from parafollicular (C) cells, not follicular cells Produces calcitonin, a key tumor marker Does NOT respond to radioactive iodine Can be sporadic (~75%) or hereditary (~25%)
🧬 The genetic connection
Hereditary MTC is associated with RET mutations Seen in MEN2 syndromes (MEN2A, MEN2B, FMTC) All patients with MTC should undergo genetic testing, regardless of age or family history
🔍 How is MTC diagnosed?
Suspicious thyroid nodule on ultrasound Elevated serum calcitonin (often markedly high) Confirmed by FNA biopsy ± calcitonin washout Imaging to evaluate lymph node involvement
⚖️ How is MTC treated?
The cornerstone of treatment is surgery:
Total thyroidectomy Central neck lymph node dissection Lateral neck dissection when nodes are involved
➡️ Radioactive iodine has no role in MTC.
➡️ Targeted systemic therapies are used in advanced disease.
📈 Prognosis
Highly dependent on stage at diagnosis Early detection → excellent long-term outcomes Lymph node and distant spread worsen prognosis
🦋 Early recognition and expert surgical management are critical.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Medullary thyroid cancer is rare but requires prompt diagnosis, genetic evaluation, and expert surgical care.
📚 References
Wells SA et al. Revised ATA Guidelines for Medullary Thyroid Carcinoma. Thyroid Elisei R et al. Management of Medullary Thyroid Cancer. Lancet NCCN Guidelines: Thyroid Carcinoma
Hürthle cell carcinoma (HCC) is a distinct subtype of differentiated thyroid cancer, accounting for ~3–5% of cases. Although related to follicular tumors, it behaves differently and requires specific management considerations.
🧠 Key characteristics of Hürthle cell carcinoma
Composed of oncocytic (Hürthle) cells rich in mitochondria More common in older patients Less likely to spread to lymph nodes More likely to spread hematogenously (lungs, bone) in higher-risk disease Often less iodine-avid than papillary or follicular thyroid cancer
🔍 How is it diagnosed?
Ultrasound and FNA may suggest a Hürthle cell neoplasm Definitive diagnosis requires surgery, based on: Capsular invasion Vascular invasion
Thyroid lobectomy for small, minimally invasive tumors Total thyroidectomy for larger or invasive disease Radioactive iodine selectively (often less effective than in other subtypes) Close long-term surveillance
📈 Prognosis
Excellent outcomes for minimally invasive disease Prognosis worsens with: Extensive vascular invasion Large tumor size Distant metastases
🦋 Careful pathology review and individualized treatment are essential.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Hürthle cell carcinoma is uncommon but highly treatable when managed by an experienced thyroid team.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Lloyd RV et al. WHO Classification of Tumours of Endocrine Organs Ganly I et al. Hürthle cell carcinoma outcomes. J Clin Endocrinol Metab
Follicular thyroid cancer (FTC) accounts for ~10–15% of thyroid cancers. While less common than papillary thyroid cancer, it is still highly treatable, especially when diagnosed early.
🧠 Key characteristics of FTC
Tends to spread through the bloodstream rather than lymph nodes Can metastasize to lungs or bones (uncommon, usually in higher-risk disease) Often appears similar to benign nodules on ultrasound Diagnosis depends on capsular and/or vascular invasion, which cannot be confirmed by FNA alone
🔍 How is FTC diagnosed?
Ultrasound and FNA may suggest a follicular neoplasm Definitive diagnosis requires surgery and full histologic evaluation Pathology distinguishes: Minimally invasive FTC Widely invasive FTC
⚖️ How is follicular thyroid cancer treated?
Management is risk-adapted and may include:
Thyroid lobectomy for minimally invasive, low-risk tumors Total thyroidectomy for higher-risk disease Radioactive iodine selectively for tumors with vascular invasion or metastases Long-term surveillance with thyroglobulin and imaging
📈 Prognosis
Excellent outcomes for minimally invasive FTC Prognosis depends on: Degree of vascular invasion Tumor size Patient age
🦋 Early, appropriate management leads to very high cure rates.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Follicular thyroid cancer often requires surgery for diagnosis, but when managed correctly, outcomes are excellent.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Lloyd RV et al. WHO Classification of Tumours of Endocrine Organs. Tuttle RM et al. Risk-adapted management of differentiated thyroid cancer. Lancet Diabetes Endocrinol
Papillary thyroid cancer (PTC) accounts for ~80–85% of all thyroid cancers. It is also the subtype with the best overall prognosis.
🧠 Key characteristics of PTC
Typically slow-growing Often diagnosed at an early stage May spread to neck lymph nodes, especially in younger patients Even with lymph node involvement, long-term survival remains excellent
🔍 How is PTC usually detected?
Incidentally on high-resolution ultrasound Confirmed with ultrasound-guided FNA biopsy Often small tumors (≤2 cm) at diagnosis
⚖️ How is papillary thyroid cancer treated?
Treatment is risk-adapted and may include:
Active surveillance for selected very low-risk tumors Thyroid lobectomy for low-risk disease Total thyroidectomy for higher-risk cases Selective lymph node surgery when indicated Radioactive iodine only for patients who truly benefit
➡️ Not all patients need the same treatment.
📈 Prognosis
10-year survival >95% Many patients live normal lifespans Focus is increasingly on quality of life, not just cure
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Papillary thyroid cancer is common, highly treatable, and often requires less aggressive treatment than patients expect.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Tuttle RM et al. Risk-adapted management of papillary thyroid cancer. Lancet Diabetes Endocrinol SEER Cancer Statistics Review
Radioactive Iodine (RAI) for Thyroid Cancer – Who Really Needs It in 2026?
Radioactive iodine (RAI, I-131) is used after thyroid surgery in selected cases of differentiated thyroid cancer (papillary and follicular). Its goals are:
to destroy tiny remnants of thyroid tissue (“remnant ablation”), to reduce the risk of recurrence (“adjuvant therapy”), or to treat known persistent or metastatic disease.
Over the last decade, we’ve learned that many low-risk patients do just as well without RAI, so we now use it much more selectively.
1. When is RAI usually recommended?
Most societies (ATA, ETA, NCCN, SNMMI/EANM) and recent data support using RAI mainly for intermediate- and high-risk disease.
RAI is typically recommended when:
High-risk disease (ATA high risk) Gross extrathyroidal extension Large primary tumors Extensive nodal disease (multiple or large metastatic nodes) Distant metastases (lung, bone, etc.) Selected intermediate-risk disease Microscopic extrathyroidal extension Multiple involved lymph nodes Aggressive histologic variants Here, RAI is considered and individualized based on age, tumor biology, thyroglobulin, and patient preferences. Persistent or recurrent disease Elevated or rising thyroglobulin after surgery Iodine-avid metastatic disease on imaging
2. When is RAI often not needed?
For many patients with true low-risk differentiated thyroid cancer, excellent outcomes can be achieved with surgery and careful follow-up without RAI.
The ESTIMABL2 randomized trial showed that in low-risk patients (small, node-negative tumors), follow-up without RAI was non-inferior to routine RAI at 5 years, with no loss of oncologic opportunity. The 2015 ATA guidelines and subsequent analyses recommend that RAI is not routinely used in ATA low-risk patients, particularly for tumors ≤4 cm without worrisome features.
For many patients, this means less treatment, fewer side effects, and the same excellent prognosis.
3. Common short-term side effects
Most side effects are mild and temporary:
Neck discomfort or swelling Nausea, metallic taste, or loss of taste Dry mouth or thick saliva Swollen, tender salivary glands (parotid/submandibular sialadenitis) Fatigue for days to weeks Temporary changes in blood counts (mild bone-marrow suppression)
Some patients also report:
Dry eyes, tearing problems, or a “gritty” sensation Nasal dryness and crusting
4. Less common or long-term risks
These are less frequent but important to discuss before treatment:
Chronic salivary gland dysfunction Persistent dry mouth (xerostomia) Difficulty with chewing/swallowing dry foods Increased dental caries and oral infections Lacrimal (tear duct) problems Nasolacrimal duct obstruction → watery or irritated eyes Sometimes requires ophthalmology intervention Fertility and pregnancy Transient effects on sperm parameters and ovarian reserve have been described at higher cumulative doses, so we usually recommend avoiding pregnancy for 6–12 months after RAI and consider sperm banking in selected young men likely to need repeated high-dose treatments. Second primary malignancies (very rare) Large observational studies suggest a small increase in risk of secondary malignancies (e.g., leukemia, salivary gland tumors) at higher cumulative doses, which reinforces the move toward lower doses and more selective use.
5. How we minimize and manage side effects
a) Use the lowest effective dose
Trials such as HiLo and related studies have shown that low-dose (≈30 mCi) RAI with recombinant TSH is as effective as higher doses for remnant ablation in low-risk patients, with fewer side effects.
b) Protect salivary glands
Aggressive hydration for several days after therapy Frequent chewing (sugar-free gum) and sour candies starting after the first 24 hours, as guided by the treating team, to stimulate saliva flow Good oral and dental hygiene, with dental follow-up for patients receiving higher doses In selected patients with significant chronic symptoms, sialogogues (pilocarpine, cevimeline) and targeted ENT/salivary management may help
c) Protect eyes and tear ducts
Artificial tears and ocular lubricants from the early post-treatment period Early evaluation by ophthalmology if tearing, pain, or recurrent eye infections develop In selected complex cases, interventional approaches to the nasolacrimal duct can be considered.
d) Monitor blood counts and overall health
Baseline and follow-up blood counts in patients receiving moderate/high doses Correct nutritional deficiencies and manage anemia or other cytopenias if they occur
e) Clear radiation-safety instructions
Temporary restrictions on close contact with children and pregnant women, sleeping in the same bed, and travel, adapted to the administered dose and national regulations.
6. Take-home messages for patients
Not everyone with thyroid cancer needs RAI. Many low-risk patients do very well with surgery and surveillance alone. When indicated, RAI can reduce recurrence and treat iodine-avid metastatic disease, particularly in higher-risk patients. Most side effects are short-term and manageable; long-term complications are less common and are more likely with higher cumulative doses. Careful risk stratification, dose selection, and prevention strategies (hydration, salivary and ocular care, blood count monitoring) are key to minimizing toxicity. Decisions about RAI should be personalized, ideally made in a multidisciplinary team with a thyroid surgeon, endocrinologist, and nuclear medicine specialist.
Suggested references (for the post footer)
Haugen BR, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016. Pacini F, et al. What are the indications for post-surgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022. Leboulleux S, et al. Thyroidectomy without radioiodine in patients with low-risk thyroid cancer (ESTIMABL2, 5-year follow-up). Lancet Diabetes Endocrinol. 2025. Mallick U, et al. Ablation with low-dose radioiodine and thyrotropin alfa. N Engl J Med. 2012. (HiLo trial) Nguyen NC, et al. Radioactive Iodine Therapy in Differentiated Thyroid Cancer: An Update on Dose Recommendations and Risk of Secondary Primary Malignancies. Semin Nucl Med. 2024. Orosco RK, et al. Radioactive iodine in differentiated thyroid cancer. Head Neck. 2019. Jeong SY, et al. Salivary gland function 5 years after radioactive iodine ablation. J Nucl Med. 2013. Solans R, et al. Salivary and lacrimal gland dysfunction after radioiodine therapy. J Nucl Med. 2001. Baudin C, et al. Dysfunction of the salivary and lacrimal glands after radioiodine therapy: START study. Thyroid. 2023. Rahmanipour E, et al. Eye-related adverse events after I-131 radioiodine therapy: systematic review. Endocr Pract. 2024. Berta DM, et al. Effect of radioactive iodine therapy on hematological parameters: systematic review and meta-analysis. Front Endocrinol. 2025.
Why Not All Thyroid Cancers Need Aggressive Treatment
Not all thyroid cancers behave the same. Modern care is personalized—the goal is to treat what matters while avoiding unnecessary treatment.
🧠 The key concept: Risk-adapted management
Many thyroid cancers—especially low-risk papillary thyroid cancers—are:
Slow-growing Unlikely to spread Associated with excellent long-term survival
Because of this, more treatment is not always better.
⚖️ Treatment options today
Depending on risk, options may include:
Active surveillance (careful ultrasound follow-up, no immediate surgery) Thyroid lobectomy instead of total thyroidectomy Selective use of radioactive iodine (not routine for everyone)
➡️ These approaches are evidence-based and safe for appropriately selected patients.
📉 Why avoid overtreatment?
Unnecessary aggressive treatment can:
Increase risk of hypocalcemia and voice changes Require lifelong thyroid hormone replacement Affect quality of life without improving outcomes
🦋 What matters most
Treatment decisions should be guided by:
✔️ Tumor size and ultrasound features
✔️ Pathology and risk of recurrence
✔️ Patient age, preferences, and values
✔️ Expertise of a multidisciplinary thyroid team
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
The best thyroid cancer treatment is the right treatment for the right patient—not the most aggressive one.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Tuttle RM et al. Active surveillance for low-risk papillary thyroid cancer. JAMA Brito JP et al. Overdiagnosis and overtreatment of thyroid cancer. BMJ
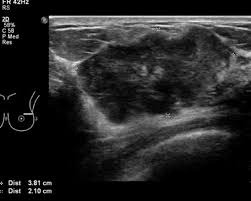
Mucinous carcinoma of the breast (also known as colloid carcinoma) is a special type of breast cancer:
Presenting with a large amount of extracellular mucin:
That is associated with a relatively favorable prognosis
These tumors are uncommon:
In most series account for approximately 1% to 2% of all invasive breast carcinomas of the breast
It is divided into two main subtypes based upon the quantification of cellularity:
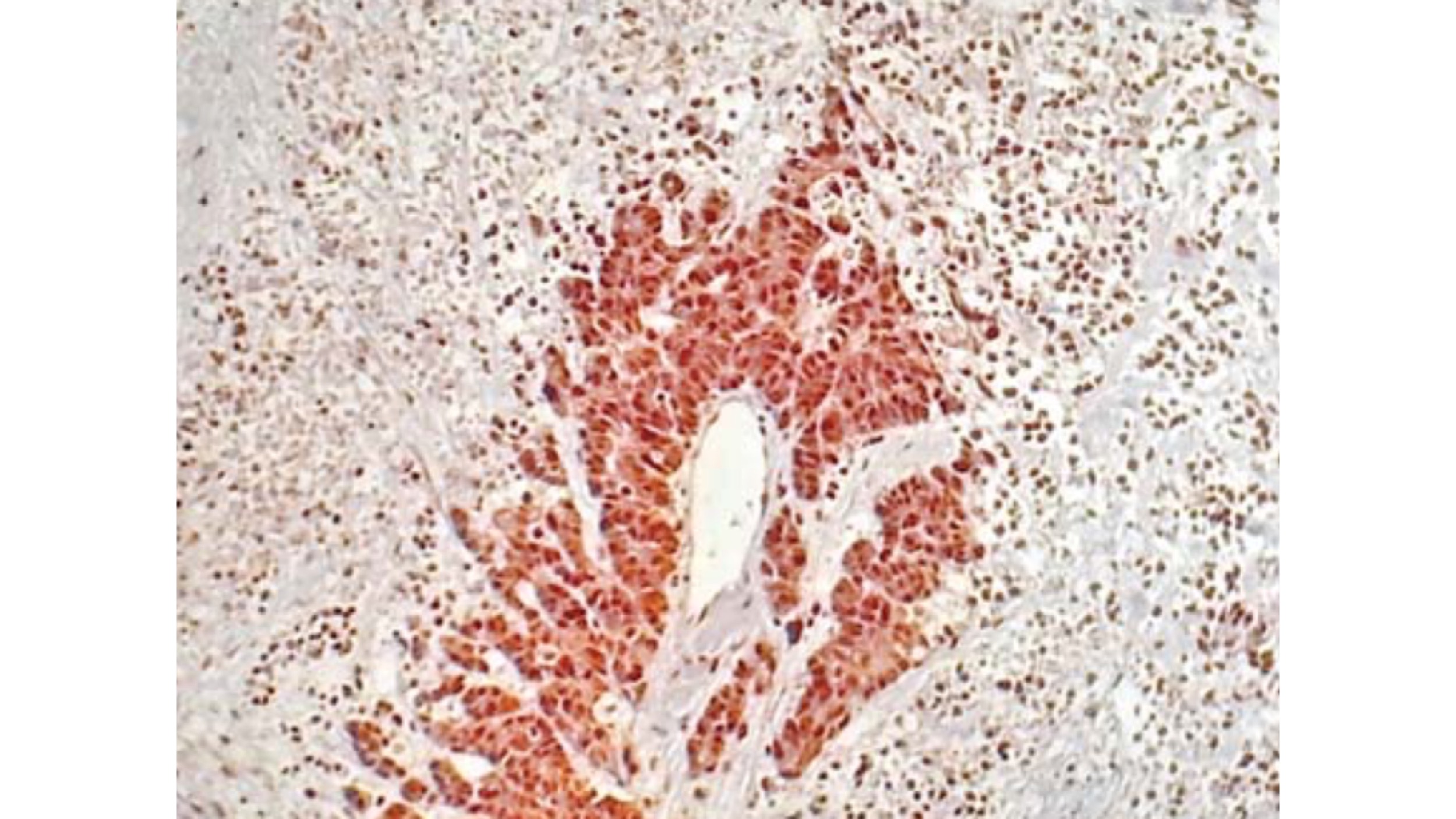
The pure type:
In pure mucinous carcinomas:
Over 90% of the tumor is made up of malignant cell clusters floating in pools of mucin (see images)
Frequently, pure mucinous carcinomas can have posterior enhancement by ultrasound imaging:
That can lead to mistaking these lesions for cysts
Patients with pure mucinous carcinomas:
Tend to be postmenopausal:
Between the ages of 59 and 71 years:
But it can occasionally occur in patients who are younger than age 40 years:
The incidence of mucinous breast cancer in women under 35 years of age is less than 1%
The mixed type:
Tumors in which 50% to 90% of the mass is composed of malignant cell clusters floating in mucin are considered to be a mixed NOS and mucinous category:
Mixed mucinous carcinomas show a less distinct margin, a higher grade, and more mitotically active cytology
Their clinicopathologic features:
Are similar to those of invasive ductal carcinoma, NOS type
Some mucinous breast carcinomas (mainly mixed type) are associated with lobular or ductal neoplasia (in situ or invasive) and some have neuroendocrine differentiation:
Mucinous breast carcinomaassociated with lobular neoplasiacomponents:
Seems to be a biologically distinct subset that frequently shows decreased cell to cell adhesion, loss of cell polarity molecules and lack of neuroendocrine differentiation:
Also in this subset of tumors, the neoplastic cells with signet-ring features are most likely to be found
Mucinous breast cancer is a slow-growing neoplasm:
With an estimated growth rate of one third of invasive breast cancer no special type
This malignancy also shows:
Fewer axillary lymph node metastases
Conventional, pure mucinous carcinomas:
Exhibit a rate of metastasis of less than 15%
Current studies have shown that a subset of patients diagnosed with mucinous carcinoma:
Do not manifest such favorable outcomes:
Some authors suggested that specific subtypes of pure mucinous carcinoma:
Those with a micropapillary pattern demonstrate significantly worse prognosis:
In one study more than half of the patients with this particular type of pattern were found to have vascular invasion and synchronous axillary lymph nodes
A subset of mucinous breast carcinomas shows neuroendocrine differentiation:
Defined by cytoplasmic argyrophilia or immunoreactivity to markers such as:
Synaptophysin
Chromogranin
Neuronal specific enolase
Although in one study neuroendocrine differentiation:
Was associated with a favorable histology and a good outcome others did not find this association
Rodrigo Arrangoiz MS, MD, FACS a surgical oncologist and is a member of Mount Sinai Medical Center in Miami:
He is an expert in the management of breast cancer:
If you have any questions about breast cancer statistics please fill free to ask Dr. Arrangoiz
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center: