My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Cancers derived from thyroid follicular cells are classified into five main types:
Papillary thyroid carcinoma (PTC:
Representing 65% to 93% of all thyroid cancers worldwide
Follicular thyroid carcinoma (FTC):
6% to 10% of cases
Oncocytic thyroid carcinoma (OC):
3% to 7% of cases
Poorly differentiated thyroid carcinoma (PDTC):
0.5% to 2%
Anaplastic thyroid carcinoma (ATC)
1% of cases
PTC, FTC and OC:
Are generically termed differentiated thyroid carcinomas (DTCs):
Most patients present with localized disease and have a 5-year survival rates of greater than 98% by contrast to PDTC, which has a 5-year survival rate of 76%
The 2022 WHO classification of thyroid tumors:
Introduced a new intermediate clinical entity:
Differentiated high-grade thyroid carcinoma:
To define DTCs with a high mitotic rate and / or tumor necrosis:
As these have a 5-year survival rate comparable with that of PDTC
ATC is an extremely aggressive form of the disease:
Until recently, patients with ATC had a dismal median overall survival of 4 months:
Although this has improved markedly since 2018 with the FDA approval of new oncoprotein-targeted treatments coupled to evidence that immunotherapies may confer additional benefit
Thyroid parafollicular or C cells are a neuroendocrine lineage that gives rise to medullary thyroid cancers:
Which account for less than 5% of all thyroid cancers
Is a malignant intra-ductal proliferation of epithelial cells within the tubular-lobular system of the breast:
With no microscopic evidence of permeation across the basement membrane
There appears to be a progression between:
Flat epithelial atypia, atypical ductal hyperplasia (ADH), and DCIS:
In which DCIS is final step prior to the development of invasive disease
The clinical risk factors and molecular aberrations related with malignant transformation:
Are almost indistinguishable between DCIS and invasive cancer
The concurrence of DCIS and invasive carcinoma within one lesion suggests that:
DCIS is a precursor lesion to invasive carcinoma
Evidence of the ability of DCIS to progress is that:
50% of all recurrences after breast-conserving surgery (BCS) for DCIS, with or without adjuvant treatment, are invasive
Data is sparse on the natural history of DCIS:
But some series have reported the outcomes for women many years after undergoing a surgical biopsy that was interpreted as benign that contained an unrecognized area of DCIS:
These data identified that approximately 20% to 53% of these women developed:
Ipsilateral invasive carcinoma
Sanders et al. reported on 28 women with unrecognized low-grade DCIS in the surgical biopsy specimen:
Of which 11 developed invasive carcinoma:
All of these cancers developed in the same breast and quadrant as the biopsy containing the DCIS
The vast majority of these invasive cancers developed within 10 years, but three were diagnosed after 20 years
Collins et al, in the Nurses’ Health Study, singled out 13 women who were found to have DCIS on reexamination of the surgical biopsies that were previously diagnosed as benign:
Ten of these women subsequently developed breast cancer
All were ipsilateral
Four were DCIS and six were invasive
The interval between the biopsy and the progression to invasive cancer was on average nine years
Approximately one in eight women (12%) in the United States (US) will be diagnosed with breast cancer in her lifetime:
20% to 25% of these newly diagnosed cases will be DCIS (Siegel 2015, CA Cancer J Clin)
In 2020, an estimated 51, 400 cases of DCIS will be diagnosed in US
Universal screening mammography:
Has resulted in a 10-fold increase in the incidence of DCIS since the mid-1980s:
But since 2003:
The incidence of DCIS has decreased in women age 50 years and older:
Conceivably secondary to decline in the use of hormone replacement therapy
While the incidence in women younger than 50 continues to increase:
Altekruse SF, Kosary CL, Krapcho M, et al.: SEER Cancer Statistics Review, 1975-2007. Bethesda, Md: National Cancer Institute, 2010. Also available online. Last accessed April 3, 2020
Roughly one in every 1,300 mammograms performed in US:
Will lead to a diagnosis of DCIS:
Representing 17% to 34% of all mammographically detected breast cancers
Before the institution of widespread screening mammography in the mid-1980s:
Most of the cases of DCIS were not identified until a palpable tumor developed:
But today:
80% to 85% of DCIS cases are screen detected
The incidence of DCIS in necropsy studies is higher than in the general population:
Proposing that not all DCIS lesions become clinically significant:
Supporting concerns that most of the increase in DCIS incidence is due to the detection of non-aggressive subtypes:
That are unlikely to progress to invasive cancer
Most women with DCIS are diagnosed at a median age:
That ranges from 47 to 63 years:
Similar to that reported for patients with invasive carcinoma
However, the age of peak incidence for DCIS (96.7 per 100,000 women):
Occurs between the ages of 65 and 69 years:
Which is younger than that for invasive breast cancer:
For which peak incidence (453.1 per 100,000 women):
Occurs between the ages of 75 and 79 years
The incidence of first-degree relatives having breast cancer (i.e., 10% to 35%) as well as deleterious mutations in the breast cancer associated (BRCA) genes:
Are similar for patients with DCIS as for women with invasive breast cancer
Other risk factors for DCIS include:
Older age
Proliferative breast disease
Increased breast density
Nulliparity
Older age at first live birth
History of breast biopsy
Early menarche
Late menopause
Long-term use of postmenopausal hormone replacement therapy
Elevated body mass index in postmenopausal women
Are the same as those for invasive breast cancer, but in many cases:
The relationship between a given characteristic and invasive cancer is stronger than the relationship between that characteristic and DCIS
Is the mucosal lining of the inner surface of the cheek
The area extends from:
The oral commisure anteriorly to the retromolar trigone posteriorly:
The junction between the buccal mucosa and retromolar trigone:
Is an arbitrary line drawn from the maxillary tuberosity to the distobuccal aspect of the mandibular third molar (or its anticipated position if not present)
The inferior and superior boundaries of the area are delineated by:
The mandibular and maxillary gingivobuccal sulci, respectively
The buccal mucosa is not exposed to masticatory loads:
So is covered by a lining mucosa with nonkeratinizing stratified squamous epithelium:
The mucosa is firmly attached to the underlying buccinator muscle
Minor salivary glands are located within the cheek (submucosa)
The parotid duct:
Pierces the buccinator muscle to enter the oral cavity adjacent to the second maxillary molar tooth
Sensory innervation to the area:
Is via the buccal branch of the mandibular division of the trigeminal nerve
Lymphatic drainage of the site:
Is via the ipsilateral facial and submandibular nodes:
To the deep cervical chain
The thickness of the cheek, from mucosal lining to external skin:
Is 1 cm to 3 cm
Epidemiology
The buccal mucosa is the most common site for oral cancer:
In South East Asia:
Up to 40% of oral cancers arising at this site
This contrasts with North America and Western Europe:
Where buccal carcinoma only accounts for 2% to 10% of oral carcinomas
The consumption of betel quid:
Is socially and culturally embedded in the countries of South East Asia:
It is responsible for the difference in site predilection
The ingredients of betel quid (paan / paan masala) varies throughout South East Asia:
The main ingredients include:
The piper betel leaf
Slaked lime
Spices
Tobacco
Areca nut
For many years, the tobacco content alone was credited as being the carcinogenic agent in betel quid:
However it is now recognized that the areca nut is also carcinogenic:
As well as being the main etiological agent in:
Oral submucous fibrosis
Individuals who consume betel quid frequently have a preference regarding which side they chew betel:
This corresponding to the side of tumor development
There is a strong association with smoking and alcohol consumption:
In populations where betel chewing is not prevalent
The male-to-female ratio:
In Western countries approximates 1:1:
However in South East Asia the ratio reflects the consumption of betel quid
In India, the male-to-female ratio:
Is approximately 4:1
In the Taiwanese population, where betel quid use occurs primarily in the male population:
The ratio may be as high as 27:1
Buccal carcinoma typically occurs over the age of 40 years:
Although it may occur in younger patients:
Particularly when associated with the habit of betel chewing
Presentation:
Buccal carcinoma may be described as:
Verrucous, exophytic or ulceroinfiltrative in character
Squamous cell carcinoma buccal mucosa of verrucous appearanceSquamous cell carcinoma buccal mucosa of ulceroinfiltrative appearance
Presentation of buccal carcinoma of the oral cavity:
Patients may present with:
Pain
An intraoral mass
Ulceration
Trismus
Patients who chew betel often have areas of:
Erythroleukoplakia of the buccal mucosa or submucous fibrosis and consequent trismus:
Making the detection of invasive squamous cell carcinoma difficult
Advanced buccal carcinomas may extend into adjacent sites to include:
External skin, mandible or maxilla
It is not unusual for patients to present with advanced disease:
40% or more presenting with stage III / IV disease
Palpable lymphadenopathy on presentation:
May be as high as 57% for T3 / T4 lesions
Occult nodal metastasis:
May be present in 26% of those who are clinically N0 at presentation:
Tumors greater than T2, are poorly differentiated, have a poor lymphocytic response or are thicker than 5 mm:
Are more likely to demonstrate cervical metastasis
Tumors are usually well differentiated
Work up:
Biopsies of buccal carcinomas should be of sufficient depth to help the pathologist give an indication of depth of invasion:
Since this will help decide on management of the neck
Buccal carcinoma may rapidly extend to adjacent sites:
Thus accurate imaging is required:
Most patients will require MRI / CT imaging:
Augmented with ultrasound scan if necessary to help in the assessment of depth of primary and cervical lymphadenopathy
Treatment
Primary site:
Traditional treatment of buccal carcinoma is:
Surgery with postoperative radiation therapy (PORT) for selected patients
T1 / T2 disease:
Can typically be resected perorally
T3 / T4 disease:
May require facial access incisions and bony resection of the maxilla and / or mandible
The primary tumor should be resected with:
A 1 cm margin and up to 2 cm if skin is involved
The buccinator muscle:
Should be included as the deep margin at the very least
The parotid duct:
May need to be repositioned or ligated
External skin should be taken with the specimen:
If there is any evidence clinically or on imaging that it is involved
Partial maxillectomy or mandibular resection (rim (marginal) or segmental) may be required.
Small T1 tumors:
May be resected and reconstructed by primary closure
Healing by secondary intention may be considered:
However postoperative trismus may be anticipated:
Unless vigorous mouth opening exercises are conducted
Split thickness skin grafts may be used:
The use of silicone sheets to stabilize the graft being useful
The use of a skin graft to reconstruct deeper resections:
May leave a very thin cheek with potentially poor aesthetics
Local flaps such as:
The buccal fat pad or temporoparietal fascial flap:
May be used for reconstruction if tumor extension does not compromise their use
Microvascular free flap reconstruction with a radial free forearm flap or anterolateral thigh flap:
Restores the thickness of the cheek and if external skin is involved:
The flaps can be bipaddled to provide reconstruction of mucosal and skin surfaces
T4 tumors requiring segmental resection of the mandible:
May require composite free flap reconstruction
Reconstruction with a radial free forearm flap:
Has been shown to give better postoperative mouth opening than reconstruction with a split skin graft or buccal fat pad
As a single treatment modality for T1 / T2 tumors has been advocated:
However, a change of practice from radiotherapy to surgery at Memorial Sloan Kettering Cancer Center was associated with improved prognosis
Brachytherapy or external beam irradiation may be considered
Management of the Neck:
Regional spread of disease in buccal carcinoma is usually to:
The ipsilateral level I and II lymph nodes
Patients with palpable lymphadenopathy or pathological nodes on imaging:
Should have a comprehensive neck dissection:
Although if pathological nodes are only located in level I, a level I to III selective neck dissection (SND) may be considered
Nodes in the region of the facial artery as it crosses the mandible:
Should be removed with the neck dissection specimen
Patients with a cN0 neck:
With a T2 or greater primary tumors or tumors with a thickness greater than 5 mm:
Should have an elective neck dissection:
Some institutions will conduct an elective neck dissection (END) if the tumor is 3 to 4 mm thick or if histological examination of the tumor demonstrates lymphatic infiltration
PORT:
The indications for postoperative radiotherapy to the loco-regional area are similar to other sites:
Notably two or more nodes in the neck, extracapsular spread (ECS), positive margins or stage III / IV disease
The beneficial role of PORT in selected patients with buccal carcinoma has been demonstrated by several authors:
Some authors suggest that PORT should be considered even in stage I and II disease, or tumors greater than 10 mm thick
Recurrence:
Recurrence rates for buccal carcinoma are 26% to 80%:
Usually occurring within two years
Involvement of the parotid duct and buccinatormuscle:
Have not been found to be significant indicators of recurrence
Outcomes and prognosis in ILC are generally favorable:
Consistent with the luminal A phenotype
The majority of evidence supporting similar or better survival as IDC:
These include a large SEER study of 263,408 women (27,639 with ILC and 235,769 with IDC) treated between 1993 and 2003:
A stage-matched analysis showed that ILC was more likely to be:
Greater than 2 cm
Lymph node positive
ER positive
The 5-year disease-free survival was significantly better for ILC than for IDC after matching for stage:
With an overall 14% survival benefit (HR 0.86) identified on multivariable analysis
As such, although overall stage-corrected prognosis appears to be favorable, some propose that this may be offset by a higher stage at presentation and higher rates of late metastatic recurrences, often occurring in atypical sites
The pleomorphic subtype of ILC is:
Also a known exception to the generally favorable prognosis, having been shown in retrospective series to more frequently develop metastatic disease than other nonpleomorphic ILCs
Currently, there are no unique specifications for surveillance of ILC:
For all treated nonmetastatic breast cancers, NCCN guidelines recommend a history and physical examination one to four times per year as clinically appropriate for 5 years and then annually
Annual mammography should be performed for patients treated with BCT
The role of MRI in surveillance is unclear and presently recommended only for those with a lifetime risk greater than 20% of developing a second primary breast cancer
Adherence to hormonal therapy should be encouraged for those prescribed and yearly gynecologic assessment arranged for those without a previous hysterectomy
Signs of disease recurrence, either locoregional or systemic, should prompt evaluation with appropriate laboratory work and diagnostic imaging, which may include diagnostic CT or fluorodeoxyglucose PET/CT scans followed by biopsy to prove first recurrence of disease
It should be noted that the generally low-grade nature of ILC may limit the sensitivity of traditional PET/CT scans, and studies are ongoing for the use of alternative radiotracers using ER ligands for increased sensitivity
Confirmed LRRs (those of the breast / chest wall and / or regional lymph nodes alone):
Can be managed with complete surgical resection and systemic therapy
Distant metastatic disease (stage IV) is managed with individualized systemic therapy
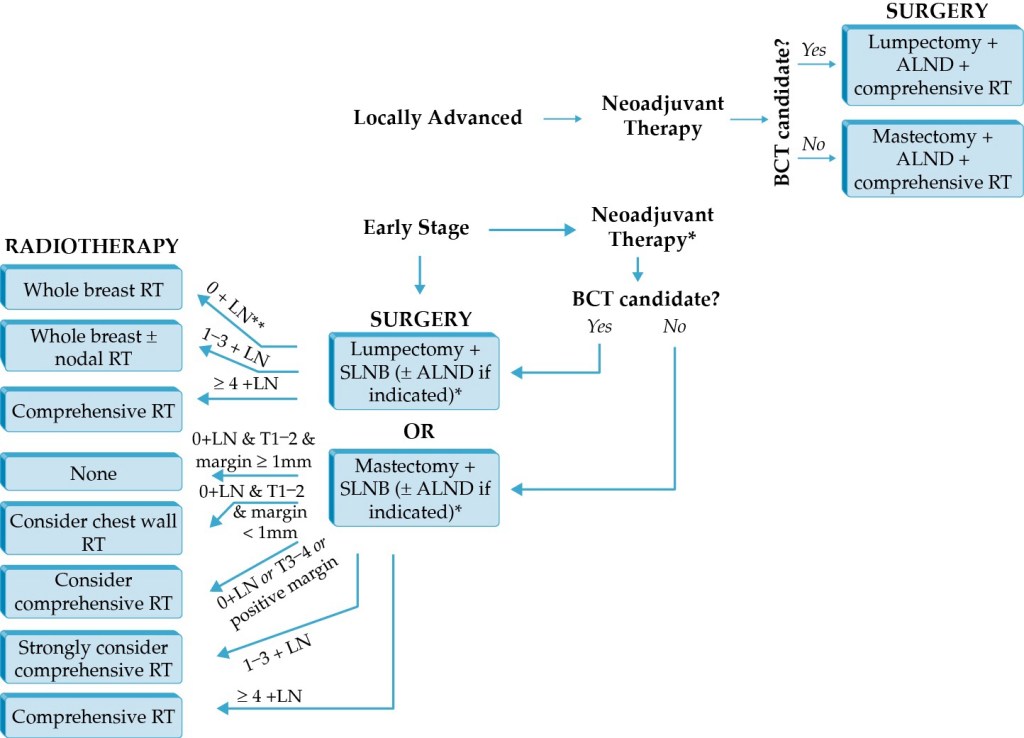
Considerations for radiation therapy (RT) in locoregional control, once more generally common among the ductal and lobular cancer types, are summarized here (Figure)
Adjuvant whole breast RT:
Reduces the risk of both local regional recurrence (LRR) and death from breast cancer after BCS and is a necessary element of BCT
Additional regional nodal irradiation:
May also be indicated for those with involvedlymph nodes or high-risk tumors
It is noteworthy that it may be acceptable to omit RT:
Among elderly women with select low-risk, ER-positive tumors:
Data to support this include the Cancer and Leukemia Group B (CALBG) 9343 randomized trial of women age 70 years or older with stage I ER-positive cancers treated with lumpectomy and tamoxifen with or without RT:
Which demonstrated no advantage in overall survival:
Although there was a small improvement in LRR among those treated with RT
Accelerated partial breast irradiation (APBI):
Is a newer technique involving more focused RT delivered in higher doses over a shorter time span
Notably, the recent American Society for Radiation Oncology (ASTRO) guideline update cites lobular histology as a criterion for “cautionary” use of APBI outside of a clinical trial
Postmastectomy RT:
May also benefit selected patients, a decision generally made by consideration of the presence of:
Macrometastatic nodal involvement
Large tumor size
High-risk disease features
It is important to note that the implications of margins at mastectomy remain controversial among radiation oncologists, and there are no data to support a definite benefit of postmastectomy RT in patients with close margins
Similar to surgical and systemic therapy trials, ILC patients comprise a minority in postmastectomy RT trials
A recent study using Survival, Epidemiology, and End Results (SEER) data including 12,703 ILC patients treated from 2004 to 2009, of which 26% had a definite indication for postmastectomy RT:
Found an improvement in 5-year overall survival and disease-specific survival from 80.9% to 84.7% (p = .0003) among ILC patients, a benefit to the same degree as IDC:
These data support continued decision making for radiotherapy using existing criteria, regardless of cancer histology
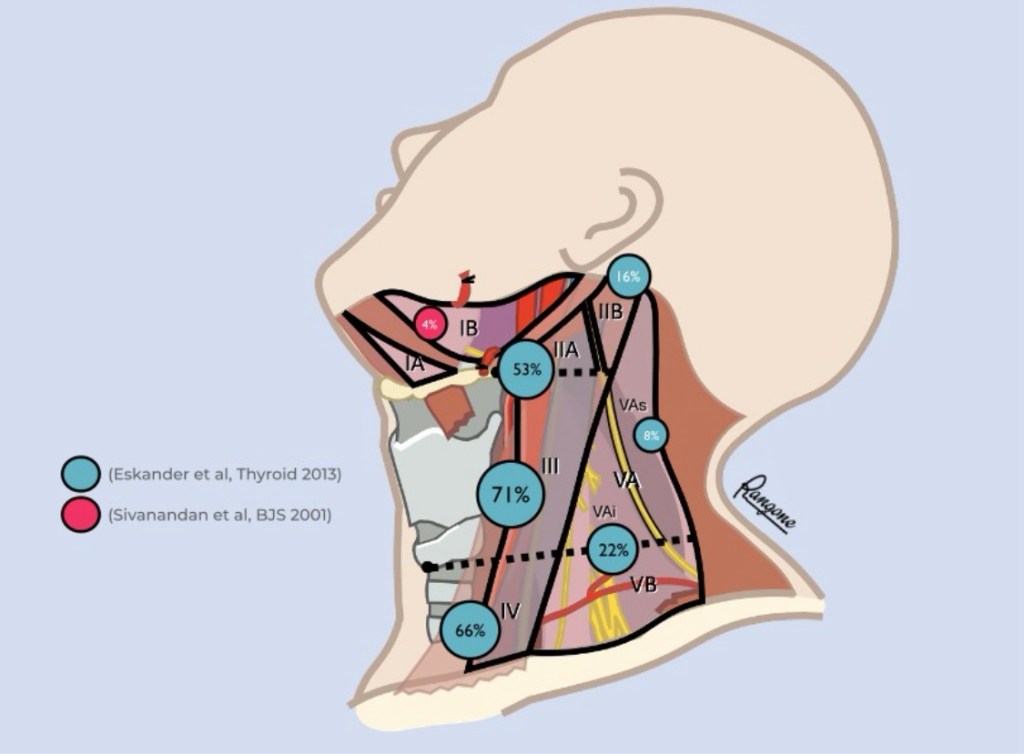
What lymph node levels does a lateral [therapeutic] neck dissection for differentiated thyroid cancer (DTX) include?
Although the rate of clinical nodal involvement in the lateral compartment was initially described by the Japanese (Noguchi et al. 1970) and Germans (Gimm et al. 1998):
Sivanandan et al (2001) were the first to systematize it by levels
In 2013, the Canadian group of Jeremy L. Freeman (Eskander et al. Thyroid) conducted a systematic review that included the meta-analysis of 18 publications (including his 2012 retrospective work with 185 patients; Merdad et al. Head Neck) agglutinating 1298 lateral neck dissections for DTC:
Emptying of sublevel IIb (retrospinal recess):
Is usually indicated when clinical, radiological or macroscopic involvement:
Is evident intraoperatively
Macroscopic involvement evident in the intraoperative sublevel IIa:
Usually determines the addition of sublevel IIb to the neck dissection
“Skip metastases” within the lateral compartment are uncommon and occur in around 9% of patients:
Level II with level III and IV
Level V with level III and IV
(Merdad et al. 2012)
Selective lymphadenectomy IIa to Vb:
Currently dissects levels IIa, III, IV, Vb and the “infraspinal” portion of the VA [VAi] in order to avoid the functional sequelae of cranial nerve XI dissection
Although heterogeneity was a constant in all comparisons by levels (I2: 31% to 87%), it is the best evidence to date that justifies the use of selective emptying IIa-Vb in this cohort of patients with this pathology:
Level III is the most frequently compromised
The majority (73%) of patients have more than one level involved:
Level III and IV: 46%
Level II, III and IV: 26%
Level III, IV and V: 11%
Level II, III, IV and V: 13%
(Merdad et al. 2012)
Levels I and sublevel Va (cranial to the distal spinal nerve pathway):
Are rarely involved, usually in patients with high disease volume and multilevel invasion
The list of cancer-associated genes continues to expand, and it is therefore increasingly important to obtain a thorough family history to assess any potential for hereditary cancer syndromes:
The BRCA1 and 2 genes account for the majority of hereditary breast cancer cases
The BRCA1 gene is located on chromosome 17q21:
It is part of the DNA repair pathway:
Functioning as a tumor suppressor gene
Presence of a deleterious BRCA1 mutation is associated with:
A lifetime breast cancer risk of:
72% by age 80
A lifetime ovarian cancer risk of:
44%
In addition, BRCA1 mutations have been associated with:
An increased risk of pancreatic cancer and melanoma
BRCA1 associated breast cancers:
Tend to occur at younger ages and are more likely to have aggressive phenotypes compared to non-BRCA-associated tumors
Lynch syndrome, also known as hereditary nonpolyposis colorectal cancer syndrome:
Is caused by genetic mutations in the mismatch repair system:
With the most common associated gene mutations being MLH1, MSH2, MSH6, and PMS2
Lynch syndrome is the most common hereditary form of colorectal cancer, and is also associated with an increased risk of:
Endometrial, urogenital, pancreatic, biliary tract and ovarian cancers:
Women with Lynch syndrome have a 20% to 60% lifetime risk of endometrial cancer
Germline mutations in the PTEN gene:
Are associated with Cowden syndrome:
Characterized by the formation of multiple hamartomas as well as an increased risk of:
Breast, endometrial, non-medullary thyroid, and renal cell cancers
Hereditary diffuse gastric cancer syndrome:
Is associated with a mutation in the CDH1 gene
It leads to an increased risk of early onset gastric cancer and lobular breast cancer
PALB2 is a breast cancer susceptibility gene:
With an estimated breast cancer risk of 45%:
PALB2 mutations have also been reported to increase the risk of:
Ovarian cancer and possibly pancreatic and prostate cancer
BRIP1 mutations:
Have been shown to confirm a high-risk of ovarian cancer (OR 20.97), but no increase in breast cancer risk
References
Shulman LP. Hereditary breast and ovarian cancer (HBOC): clinical features and counseling for BRCA1 and BRCA2, Lynch syndrome, Cowden syndrome, and Li-Fraumeni syndrome. Obstet Gynecol Clin North Am. 2010;37(1):109-133, Table of Contents.
Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. Jama. 2017;317(23):2402-2416.
Mersch J, Jackson MA, Park M, et al. Cancers associated with BRCA1 and BRCA2 mutations other than breast and ovarian. Cancer. 2015;121(2):269-275.
Southey MC, Winship I, Nguyen-Dumont T. PALB2: research reaching to clinical outcomes for women with breast cancer. Hered Cancer Clin Pract. 2016;14:9.
Weber-Lassalle N, Hauke J, Ramser J, et al. BRIP1 loss-of-function mutations confer high risk for familial ovarian cancer, but not familial breast cancer. Breast Cancer Res. 2018;20(1):7.
Has a high predilection for spread to locoregional lymph nodes (LNs):
Occurring in up to 40% to 90% of cases:
When prophylactic nodal dissection is performed:
Though such high rates of metastatic disease may prove enticing to recommend routine prophylactic node dissection:
Recurrence-free survival is not effected by the removal of sonographically normal, microscopically diseased nodes
Instead, prophylactic central neck dissection may be individually considered for those patients with:
T3 or T4 tumors, or in the presence of lateral neck metastases
Clinically suspicious or biopsy-proven nodal disease warrants a “therapeutic” dissection of the involved compartments
“Berry picking,” or selective removal of suspicious LN metastases, is not recommended:
As it is associated with significantly higher recurrence rates and does not lower the rate of postoperative complications compared with systematic compartmental dissections
The risk of surgical complications with nodal dissection should be weighed against the benefit of LN removal:
Central neck dissections may result in temporary or permanent injury to the RLN and hypoparathyroidism
Surgeon case volume predicts patient outcomes:
Those performing less than 10 cases compared with those performing more than 100 cases per year had complications in 24% and 14.5% of cases, respectively
Although dissection of the lateral neck is less often associated with adverse events:
Injury to the spinal accessory nerve may occur with dissection of level II or V
Similarly, chyle leaks may be seen after removal of nodes in level IV: