The thyroid gland as well as the adrenal glands have the greatest blood supply per gram of tissue. The significance is that hemostasis is a major problem of thyroid surgery, especially in patients with goiter.
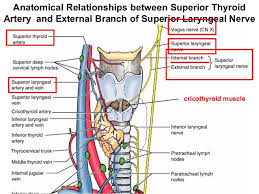
The arterial irrigation to the thyroid gland comes from two paired arteries, the superior and inferior thyroid arteries and, sometimes, from the thyroidea ima. These arteries have abundant collateral anastomoses with each other, ipsilaterally and contra-laterally (Figure). The thyroid ima is a single vessel that, when present (1% to 4% of individuals), originates from the aortic arch or the innominate artery and enters the thyroid gland at the inferior border of the isthmus. Its position anterior to the trachea makes it important in tracheostomy.
The superior thyroid artery is the first anterior branch of the external carotid artery. In rare cases, it may arise from the common carotid artery just before its bifurcation. The superior thyroid artery passes downward and anteriorly to reach the superior pole of the thyroid gland under the cover of the superior belly of the omohyoid and sternohyoid muscles. In part of its track, the artery parallels the external branch of the superior laryngeal nerve (SLN) which supplies the cricothyroid muscle and the cricopharyngeus muscle, the lowest voluntary part of the pharyngeal musculature. The artery runs superficially on the anterior border of the lateral lobe, dividing into anterior and posterior branches at the apices of the thyroid lobes. These branches send branches (terminal) deep into the thyroid gland before curving toward the isthmus, where they anastomose with the contralateral artery (usually the anterior branch).
The superior thyroid artery has six branches: the infrahyoid, sternocleidomastoid, superior laryngeal, cricothyroid, inferior pharyngeal constrictor, and terminal branches of the artery for the supply of the thyroid and parathyroid glands. There are usually two branches to the thyroid gland (anterior and posterior) but in rare instances there may be a third branch, the so-called lateral branch. The anterior branch anastomoses with the contralateral artery, the posterior branch anastomoses with the ipsilateral inferior thyroid artery. The posterior branch gives off a small parathyroid artery which supplies the superior parathyroid gland in 45% of the cases. Nobori et al. noted that in 67% of the cases the superior parathyroid glands received their blood supply from a single vessel, and in 1/3 of the cases two or more branches reached the superior parathyroid glands.
High ligation of the superior thyroid artery during thyroidectomy places the external branch of the SLN at risk of inadvertent injury, which would produce dysphonia by altering pitch regulation. The cricothyroid artery, a potentially troublesome branch of the superior thyroid artery, runs superior to the upper pole and runs toward the midline on the cricothyroid ligament. This vessel can be lacerated during emergent cricothyroidotomy.
The inferior thyroid artery usually arises from the thyrocervical trunk (Figure 5), a branch of the subclavian artery, but in 15% of individuals it may arise from the subclavian artery. The inferior thyroid artery ascends vertically behind the carotid sheath curving medially and posteriorly on the anterior surface of the longus coli muscle before entering the tracheoesophageal groove. After penetrating the prevertebral fascia, the artery divides into two or more branches as it crosses the RLN. The lowest branch sends a tinny branch to supply the inferior parathyroid gland and supplies the lower pole of the thyroid gland [2]. The upper branch of the inferior thyroid artery supplies the posterior surface of the gland, usually anastomosing with the descending branch of the superior thyroid artery (posterior branch). On the right-hand side the inferior thyroid artery is absent in approximately 2% of individuals, on the left-hand side it is absent in 5% of the cases. A duplicated artery is a rare occurrence.
The RLN ascends in the tracheoesophageal groove and enters the larynx between the inferior cornu of the thyroid cartilage and the arch of the cricoid cartilage (Figure). The RLN can be found after it emerges from the superior thoracic outlet, in a triangle bounded laterally by the common carotid artery, medially by the trachea, and superiorly by the thyroid lobe. The relationship between the inferior thyroid artery and the RLN is highly variable, as established by the work of Reed A.F., who in 1943 described 28 variations in this relationship. The RLN can be found deep to the inferior thyroid artery (40% of the cases), superficial to the RLN (20% of the cases), or between the branches of the inferior thyroid artery (35% of the cases). Notably, the association between the RLN and the inferior thyroid artery on one side of the neck is comparable to that found on the other side in only 17% of individuals. Furthermore, at the level of the inferior thyroid artery, branches of the RLN that are extra laryngeal may be present in 5% of the cases. Preservation of all of those branches is very important during thyroid surgery.
Veins of the thyroid gland form a plexus of vessels lying in the substance and on the surface of the gland. The plexus is drained by three pairs of veins that provide venous drainage for the thyroid (Figure). The superior thyroid vein accompanies the superior thyroid artery. As it emerges from the superior pole of the thyroid gland, the vein passes superiorly and laterally across the superior belly of the omohyoid muscle and the common carotid artery to enter the internal jugular vein alone or with the common facial vein. The middle thyroid vein arises on the lateral surface of the thyroid gland at about two-thirds of its anteroposterior extent. It crosses the common carotid artery following a direct course to the internal jugular vein (no artery escorts it). This vein may be absent or, in very rare occurrences it may be double. The extra vein is inferior to the normal vein (fourth thyroid vein). The importance of these thyroid veins is in their vulnerability during thyroid surgery. The inferior thyroid veins are the largest and most variable of the thyroid veins (the right and left side are usually asymmetric. They follow different pathways on each side. The right inferior thyroid vein passes anterior to the innominate artery to drain into the right brachiocephalic vein, rarely in may cross anterior to the trachea and drain into the left brachiocephalic vein. The left vein crosses the trachea to enter the left brachiocephalic vein. Sporadically, both inferior thyroid veins form a common trunk called the thyroid ima vein, which empties into the left brachiocephalic vein.
Rodrigo Arrangoiz MS, MD, FACS
Cirugía Oncológica
Fox Chase Cancer Center
Tumores de Cabeza y Cuello / Cirugía Endocrina
Fox Chase Cancer Center
Tumores de Cabeza y Cuello / Cirugía Endocrina
IFHNOS / Memorial Sloan Kettering Cancer Center
Maestría en Ciencias de Investigación
Drexel University
Certificado por el Colegio Americano de Cirugía
Fellow del Colegio Americano de Cirugía
Fellow de la Sociedad de Cirugia Oncológica
Sociedad Quirúrgica S.C.
Hospital ABC Santa Fé
Av. Carlos Graef Fernández #154
Consultorio 515
Col. Tlaxala, Delg. Cuajimalpa
México, D.F. 05300
Tel: 1103 – 1600 Ext 4515 a la 4517
Fax:1664 – 7164