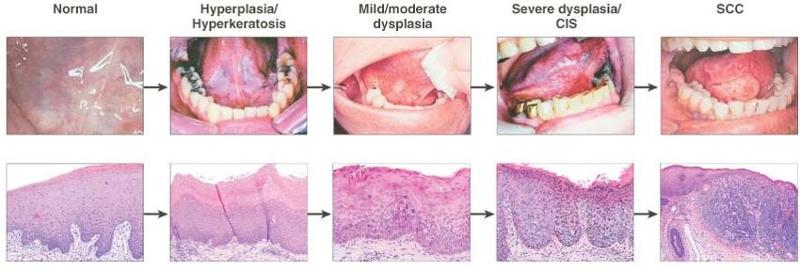
La característica histológica más importante del tumor primario que afecta la selección del tratamiento y el pronóstico final es su profundidad de infiltración.
-
Las lesiones delgadas y superficialmente invasivas tienen un riesgo menor de metástasis a los ganglios linfáticos regionales, son altamente curables y ofrecen un excelente pronóstico.

-
Por otro lado, las lesiones más gruesas que infiltran profundamente los tejidos blandos subyacentes tienen una incidencia significativamente mayor de metástasis en los ganglios linfáticos regionales y un impacto adverso en el pronóstico.

El riesgo de metástasis ganglionares y tasas de supervivencia en relación con el espesor de la lesión primaria para los carcinomas escamosos T1 y T2 de la lengua y el piso de la boca se muestran en la siguiente figura:
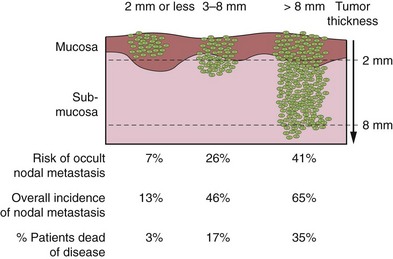
Aunque sería ideal conocer el espesor exacto de la lesión antes de la intervención quirúrgica, en muchos casos tener esa información antes de la extirpación quirúrgica del tumor primario es clínicamente poco práctico.
-
En general, sin embargo, el grosor de la lesión apreciado por la palpación es un indicador razonablemente bueno de lesiones profundamente invasivas versus lesiones superficiales para estimar el grado de resección de tejido blando y / o hueso para la lesión primaria y para decidir sobre la necesidad de disección electiva de los ganglios linfáticos regionales en riesgo en un cuello con hallazgos clínicos negativos.
Rodrigo Arrangoiz MS, MD, FACS
Cirugía General y Gastrointestinal
Michigan State University
Cirugía Oncológica
Cirugía General y Gastrointestinal
Michigan State University
Cirugía Oncológica
Fox Chase Cancer Center
Tumores de Cabeza y Cuello / Cirugía Endocrina
Fox Chase Cancer Center
Tumores de Cabeza y Cuello / Cirugía Endocrina
IFHNOS / Memorial Sloan Kettering Cancer Center
Maestría en Ciencias de Investigación
Drexel University
Certificado por el Colegio Americano de Cirugía
Drexel University
Certificado por el Colegio Americano de Cirugía
Fellow del Colegio Americano de Cirugía
Fellow de la Sociedad de Cirugia Oncológica
Sociedad Quirúrgica S.C.
Hospital ABC Santa Fé
Av. Carlos Graef Fernández #154
Sociedad Quirúrgica S.C.
Hospital ABC Santa Fé
Av. Carlos Graef Fernández #154
Consultorio 515
Col. Tlaxala, Delg. Cuajimalpa
México, D.F. 05300
Tel: 1103 – 1600 Ext 4515 a la 4517
Fax:1664 – 7164
Col. Tlaxala, Delg. Cuajimalpa
México, D.F. 05300
Tel: 1103 – 1600 Ext 4515 a la 4517
Fax:1664 – 7164