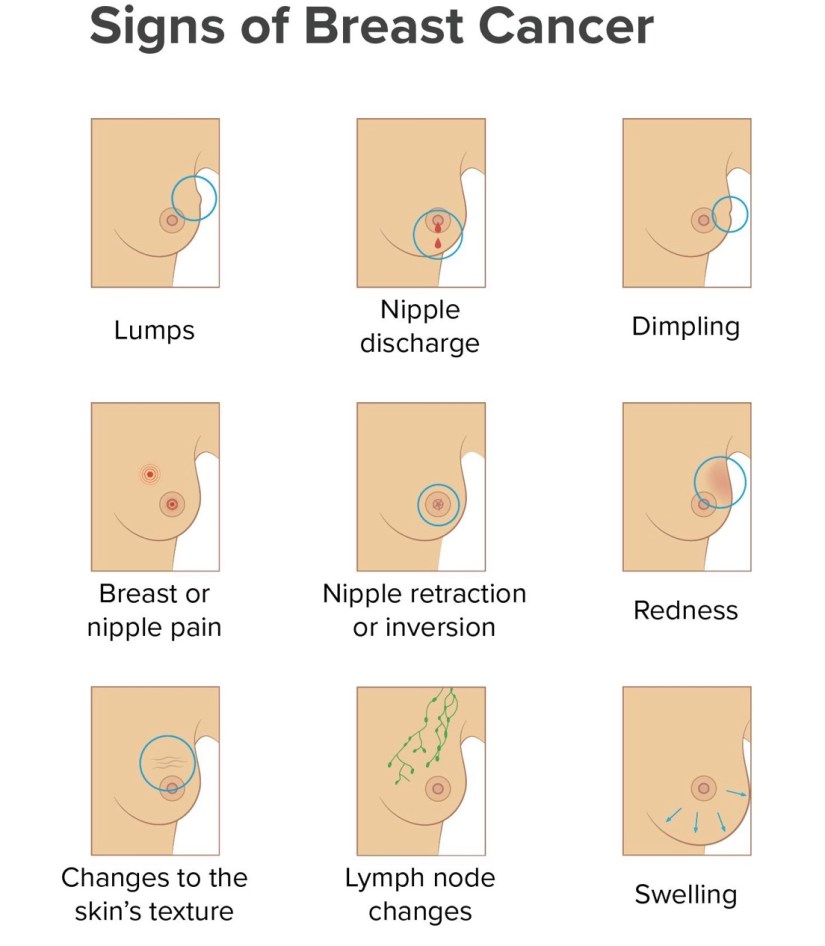
👉Pathologic nipple discharge usually is unilateral, presents from a single duct, and is spontaneous, bloody, or serous.
👉Physiologic nipple discharge can be green or white, bilateral, from multiple ducts, or present only with manual expression of the breast.
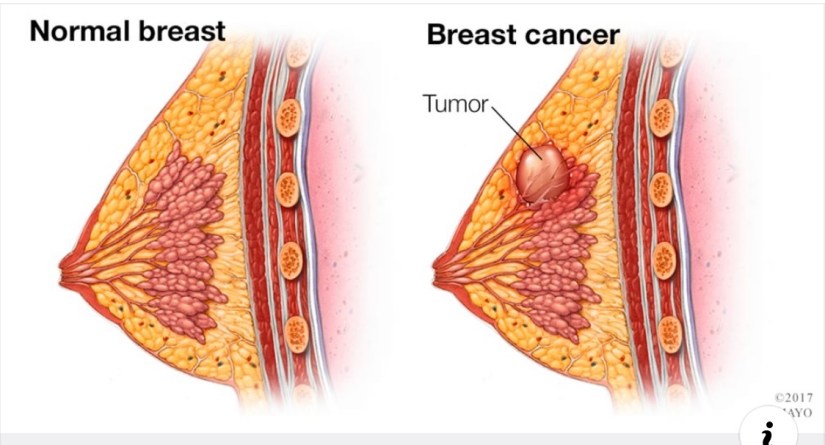
👉When pathologic discharge is present, the most common etiology remains a benign intraductal papilloma.
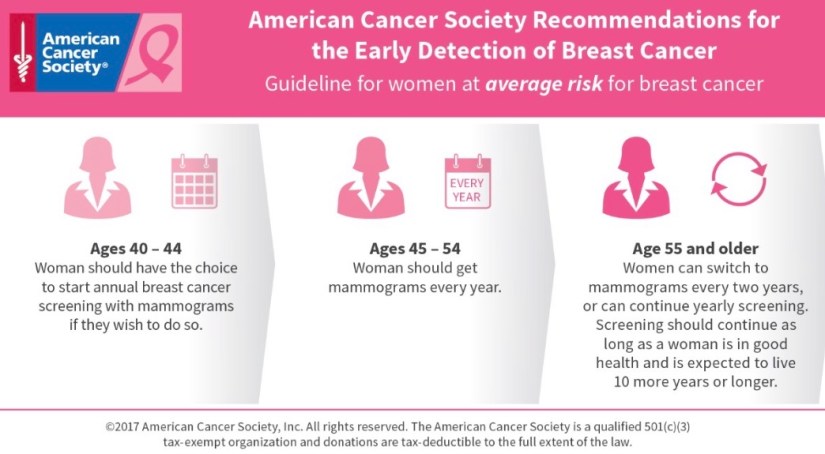
👉Mammography in this setting is limited by its low sensitivity for intraductal lesions.
👉Ultrasound in conjunction with mammography can improve sensitivity for intraductal masses but imaging alone cannot reliably distinguish benign from malignant lesions.
👉When imaging identifies an abnormal finding in the setting of nipple discharge, needle biopsy is helpful to determine etiology and guide future excision.
👉When imaging work-up is otherwise negative, investigators have attempted to identify patients with nipple discharge in whom operation can be avoided.
👉One study showed 192 patients with unilateral, single duct, spontaneous, bloody, or serous nipple discharge and a normal mammogram had a less than 3% chance of malignancy. When they had a normal subareolar ultrasound as well, no patient had a cancer, but the numbers were small.
👉On the other hand, a separate study found conflicting results as researchers identified cancer in 10% of patients who had normal physical examination, mammography, and ultrasound. The same group found that when additional evaluation was done with cytology, ductography, or MRI, 7% (19/287) of patients were still diagnosed with cancer on duct excision.
👉Ductogram is a challenging technique that requires breast imaging expertise. It is often helpful in localizing an intraductal lesion and guiding percutaneous vacuum-assisted or surgical removal, but it does not reliably exclude a malignant lesion.
👉Negative imaging does not obviate the need for surgical excision in a woman with spontaneous, single duct, bloody nipple discharge.
👉The standard management for unilateral bloody nipple discharge that is without an imaging abnormality therefore remains duct excision that is selective of the offending duct or as a major duct excision.
👉When a retroareolar imaging abnormality is identified in the setting of nipple discharge it should be localized and removed.
👉Starting in October (Breast Cancer Awareness Month) Rodrigo Arrangoiz MS, MD, FACS member of Sociedad Quirúrgica S.C. will be writing daily post on breast diseases.

Rodrigo Arrangoiz MS, MD, FACS is surgical oncologist / breast cancer specialist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


For more information visit: http://www.cirugiatiroides.com
#Arrangoiz
#Teacher
#Surgeon
#Cirujano
#BreastExpert
#BreastSurgeon
#CirujanodeMama
#ExpertoenCancerdeMama
#CancerdeMama
#SurgicalOncologist
#CirujanoOncologo
#CancerSurgeon










 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Maestria en ciencias (Clinical research for healthprofessionals):
• Maestria en ciencias (Clinical research for healthprofessionals): • Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina