👉Suspecting impaired thyroxine absorption:
👉Check the following:
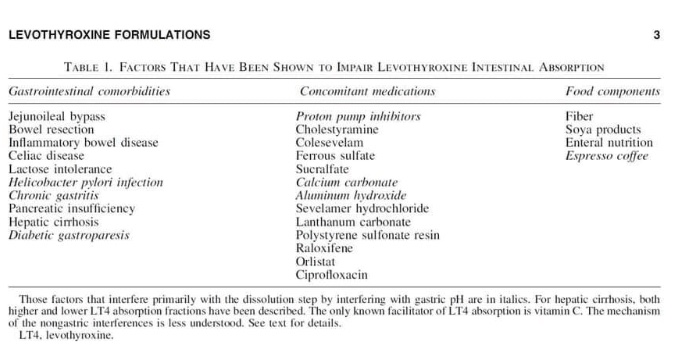
#Arrangoiz #ThyroidSurgeon
👉Suspecting impaired thyroxine absorption:
👉Check the following:
#Arrangoiz #ThyroidSurgeon
Investigators observed a survival benefit for patients receiving lenvatinib who had radioiodine-refractory differentiated thyroid cancer with lung metastases of 1 cm or greater.null
Patients with radioiodine-refractory differentiated thyroid cancer (RR-DTC) who had lung metastases of 1 cm or greater experienced improved overall survival (OS) when treated with lenvatinib (Lenvima) compared with placebo, according to data published in the European Journal of Cancer.
These data were taken from the phase 3 SELECT trial (NCT01321554), for which the research team hypothesized that initiating lenvatinib early may improve the outcomes of patients with RR-DTC.2 The current analysis looked at patients treated on the trial who had any baseline lung metastases.
“Although OS was not significantly prolonged with lenvatinib treatment versus placebo in patients with any lung metastases, it was significantly prolonged in patients with baseline lung metastases of 1.0 cm [or more],” wrote the investigators. “The results of this analysis also suggest that the treatment effect of lenvatinib may be greater when lenvatinib is initiated in patients with a lower burden of disease, rather than delaying initiation until a higher burden of disease is present.”
The study population included 392 patients with RR-DTC who were randomized 2:1 to receive either lenvatinib 24 mg daily (n = 261) or placebo (n = 131). Patients in the current analysis had any baseline metastases (n = 26) and were further grouped via size of target lung lesions at 1.0 cm or greater (n = 199), 1.5 cm or greater (n = 150), 2.0 cm or greater (n = 94), and more than 2.0 cm (n = 105).
For the group of patients with any lung metastases treated with lenvatinib, there was no statistically significant improvement in OS observed compared with the placebo arm (HR, 0.76; 95% CI, 0.57-1.01; P = .0549).
When analyzing the results by metastases size, a significant improvement in median OS was observed for patients with metastases of 1.0 cm or greater treated with lenvatinib at 44.7 months compared with 33.1 months for patients in the placebo arm (HR, 0.63; 95% CI, 0.47-0.85; P = .0025).
Compared with placebo, prolonged OS for patients treated with lenvatinib were observed in the 1.0 cm or greater (HR, 0.63; 95% CI, 0.47-0.85), 1.5 cm or greater (HR, 0.63; 95% CI, 0.45-0.89), 2.0 cm or greater (HR, 0.65; 95% CI, 0.44-0.98), and less than 2.0 cm (HR, 0.63; 95% CI, 0.40-0.99) patient groups. The median OS reported in the 2.0 cm or greater group (34.7 months) was shorter than that of the other subgroups (range, 44.1-49.2 months).
“In the overall population of patients from SELECT who had any lung metastases, a longer median OS was observed following lenvatinib treatment versus placebo, but the difference was not significant,” wrote the investigators. “…Additionally, lenvatinib treatment resulted in longer OS and PFS in all subgroups, regardless of the size of the lung metastasis at baseline.”
Eligible patients were 18 years or older, had measurable RR-DTC via RECIST v1.1, experienced progression within the last 13 months, had 1 prior VEGF or VEGFR-targeted therapy and had adequately controlled blood pressure.
Patients receiving placebo were allowed to transfer to open-label lenvatinib treatment following disease progression.
References:
1. Tahara M, Kiyota N, Hoff AO, et al. Impact of lung metastases on overall survival in the phase 3 SELECT study of lenvatinib in patients with radioiodine-refractory differentiated thyroid cancer. Eur J Cancer. 2021;147:51-57. doi: 10.1016/j.ejca.2020.12.032
2. Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. 2015;372(7):621-630. doi:10.1056/NEJMoa1406470
#Arrangoiz #ThyroidSurgeon #CancerSurgeon #SurgicalOncologist #HeadandNeckSurgeon #CASO #CenterforAdvancedSurgicalOncology

#Arrangoiz #BreastCancer #BreastSurgeon #CancrerSurgeon #Miami #SurgicalOncologist #CASO #CenterforAdvancedSurgicalOncology
https://drive.google.com/file/d/1u4JWeR7xE5oBV8f8acmBkmZTGmxabGlr/view
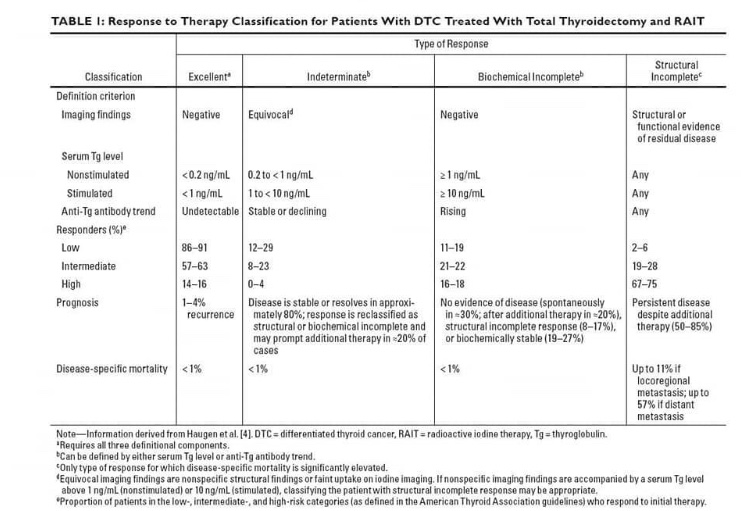
👉Dynamic risk stratification to determine need or benefit of RAI treatment for thyroid cancer patients
https://drive.google.com/file/d/1u4JWeR7xE5oBV8f8acmBkmZTGmxabGlr/view
👉Abstract: The term thyroid neoplasm incorporates tumors that originate from follicular cells and those that arise from parafollicular cells (C cells). Differentiated thyroid cancer, which originates from follicular cells, includes papillary thy- roid carcinoma (PTC), follicular thyroid carcinoma (FTC), oncocytic cell car- cinoma (Hürthle), poorly differentiated carcinoma, and anaplastic thyroid carcinoma (ATC). PTC tends to have an indolent clinical course with low morbidity and mortality. However, this entity has a broad range of biological and clinical behavior that can result in disease recurrence and death, de- pending on patient and tumor characteristics and the initial treatment ap- proach. PTC is the most common form of well-differentiated thyroid cancer (WDTC) and based on the most recent statistics, accounts for approximately 89.4% of all thyroid malignancies. PTC appears as an irregular solid or cystic nodule in normal thyroid parenchyma. PTC has the propensity for lymphatic invasion, but it is less likely to have hematogenous spread. Around 11% of patients with PTC present with distant metastases outside the neck and me- diastinum. This manuscript with review the current understanding of the ep- idemiology, pathology, molecular characteristics, prognostic factors, and dy- namic risk stratification of PTC centered on an evidence-based and persona- lized approach.
👉Keywords
Thyroid Cancer, Papillary Thyroid Cancer, Papillary Thyroid Microcarcinoma, Thyroid Nodule, Thyroid Cancer Treatment, Molecular
👉Arrangoiz, R., De Llano, J.G., Mijares, M.F., Fernandez-Chri- stlieb, G., Vasudevan, V., Sastry, A., Legas- pi, A., Fernandez, J., de la Cruz, F., Corde- ra, F. and Margain, D. (2021) Current Un- derstanding of Papillary Thyroid Carcino- ma. International Journal of Otolaryngolo- gy and Head & Neck Surgery, 10, 184-221. https://doi.org/10.4236/ijohns.2021.103019
👉https://www.scirp.org/pdf/ijohns_2021052114524635.pdf
#Arrangoiz #CancerSurgeon
The FDA granted fast track designation to the chimeric antigen receptor T-cell therapy AIC100 as treatment for patients with anaplastic thyroid cancer and refractory poorly differentiated thyroid cancer, according to the company responsible for this cellular therapy, AffyImmune Therapeutics, Inc.1
The designation allows for the rapid development and review of drug candidates with the potential to serve an unmet medical need. It also means the company will have better access to the FDA with more frequent interactions regarding the development process, earlier approval, and patient access.
“We are pleased to have received Fast Track designation for our first-in-human CAR T-cell product currently being tested in patients with refractory thyroid cancer,” Eric von Hofe, President and COO of AffyImmune, said in a press release. “It highlights the unmet need in treating refractory solid tumors and points to the potential of AIC100 to address that need. We look forward to a close relationship with the FDA to expedite development and future approvals.”
The cellular therapy is currently being examined in a phase 1 trial (NCT04420754) of 24 participants with either relapsed/refractory poorly differentiated thyroid cancer or anaplastic thyroid cancer. Patients are treated in 1 of 4 cohorts by dose levels of 1 × 10-6, 1 × 10-7, 1 × 10-8, or 5 × 10-8 CAR-positive T-cells. Treatment is planned as a single-dose infusion, but additional administrations may be necessary in the case of partial response or stable disease within 30 days, investigator decision, the absence of dose-limiting toxicities, or available cell doses already manufactured.
The primary end point of the trial is the overall incidence of grade 3 or greater adverse effects (AEs) and the incidence of CAR T-cell therapy–related AEs, such as cytokine release syndrome, immune effector cell-associated neurotoxicity syndrome, hemophagocytic lymphohistiocytosis or macrophage activation syndrome, and tumor lysis syndrome. Secondary outcome measures include detection, expansion, and persistence of AIC100 after infusion, analysis of CAR T-cell subsets in peripheral blood by flow cytometry, assessment and analysis of CAR T-cell infiltrate by tumor biopsy at treatment completion or progression, cytokine levels in plasma samples, and CAR T antibodies in peripheral blood.
Eligible patients will have anaplastic thyroid cancer that is either BRAF wild type or BRAF mutant after BRAF inhibitor failure or poorly differentiated thyroid cancer that has failed surgery, radioactive iodine, chemotherapy, radiation therapy and/or targeted therapies with measurable disease, and ECOG performance status of 2 or lower, and a life expectancy of 8 weeks or more. Adequate hepatic, kidney, bone marrow, and coagulation function and no lingering toxicities from prior anticancer therapy are also required.
AIC100 is 1 of several CAR T-cell therapies being developed by AffyImmune Therapeutics, Inc. to treat solid tumors. It is an affinity-tuned ICAM-1 targeted, third-generation, CAR T-cell product. In addition to indications in thyroid cancer, the therapy is also being explored in patients with gastric cancer and triple-negative breast cancer.2
References
1. AffyImmune Therapeutics’ AIC100 Granted Fast Track Designation for Treating Thyroid Cancer. News release. AffyImmune Therapeutics, Inc. May 17, 2021. Accessed May 24, 2021. https://prn.to/3fL5paW
2. AffyImmune Is Developing a Leading Pipeline of Affinity-Tuned CAR T-cell Therapies to Treat Solid Tumors. AffyImmune Therapeutics, Inc. Accessed May 24, 2021. https://bit.ly/3wwbrDa
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #ThyroidCancer #HeadandNeckSurgeon #CASO #CenterforAdvancedSurgicakOncology

#Arrangoiz #ParathyroidSurgeon #ParathyroidExpert #HeadandNeckSurgeon #EndocrineSurgery #Hyperparathyroidism #Hypercalcemia #CASO #CenterforAdvancedSurgicalOncology

#Arrangoiz #ThyriodSurgeon #ThyroidExpert #HeadandNeckSurgeon #CancerSurgeon #ThyroidDisease #ThyroidCancer #MultinodularGoiter #Goiter #SubsternalGoiter #CASO #CenterforAdvancedSurgicalOncology

#Arrangoiz #ThyroidSurgeon #ThyroidExpert #HeadandNeckSurgeon #CancerSurgeon #MultinodularGoiter #Goiter #SubsternalGoiter #CASO #CenterforAdvancedSurgicalOncology
👉After receiving a diagnosis of papillary thyroid cancer, intuitively, the thought has been that surgery is the next step.
👉While this was the standard in the past, we now know that in specific situations immediate surgery may not be necessary.
👉The incidence of thyroid cancer has increased significantly over the last three decades in large part due to tumors being identified incidentally on imaging studies. It is important to note that despite the increased rate of detection, the mortality rate from thyroid cancer remains very low and unchanged. Therefore, many of these cancers are low risk, and if left alone, would likely not pose a threat to the patient. There has been significant research looking at monitoring low risk thyroid cancers without surgery especially when surgically removing the tumor could potentially do more harm than good. This monitoring approach without surgical intervention is known as active surveillance.
👉In general, to be eligible for active surveillance: the tumor should be ≤ 1cm -1.5cm, there should not be any evidence of lymph node metastases, there should not be suspicion of more aggressive subtypes such as tall cell or sclerosing variant papillary thyroid cancer, and the tumor should not be located near a vulnerable area where growth could compromise important structures such as the trachea or the recurrent laryngeal nerve.
👉Active surveillance should be done at a medical center with a multidisciplinary approach and ultrasound expertise. Active surveillance typically entails monitoring with ultrasound every 6 months initially with extension of the surveillance interval over time.
👉While undergoing surveillance, if there is significant growth (≥3mm) of the nodule, evidence of lymph node involvement, extension into adjacent structures, or change in patient preference, then surgical intervention is recommended.
👉Surgery at time of disease progression has been shown to have the same excellent prognosis. There have been ongoing prospective studies on active surveillance over the course of the last twenty years that have shown a low rate of progression (10-15%) and no deaths or development of distant metastasis during active surveillance.
👉The decision to pursue active surveillance is a shared decision between the patient and the physician after discussion of the risks and benefits based on each patient’s unique circumstances. Additional factors when considering active surveillance include: cost and time associated with appointments needed for surveillance, age of patient, medical comorbidities, and the possible increased emotional burden or anxiety that can result from opting to not remove the cancer at time of initial diagnosis.
👉The “best” treatment strategy will differ depending on each patient, so I hope that this information encourages discussion between patients and their endocrinologists to help decide which treatment option is best for them.
References:
1. Sugitani I, Ito Y, Takeuchi D, Nakayama H, Masaki C, Shindo H, Teshima M, Horiguchi K, Yoshida Y, Kanai T, Hirokawa M, Hames KY, Tabei I, Miyauchi A. Indications and Strategy for Active Surveillance of Adult Low-Risk Papillary Thyroid Microcarcinoma: Consensus Statements from the Japan Association of Endocrine Surgery Task Force on Management for Papillary Thyroid Microcarcinoma. Thyroid. 2021 Feb;31(2):183-192.
2. Molinaro E, Campopiano MC, Pieruzzi L, Matrone A, Agate L, Bottici V, Viola D, Cappagli V, Valerio L, Giani C, Puleo L, Lorusso L, Piaggi P, Torregrossa L, Basolo F, Vitti P, Tuttle RM, Elisei R. Active Surveillance in Papillary Thyroid Microcarcinomas is Feasible and Safe: Experience at a Single Italian Center. J Clin Endocrinol Metab. 2020 Mar 1;105(3):e172–80.
3. Tuttle RM, Alzahrani AS. Risk Stratification in Differentiated Thyroid Cancer: From Detection to Final Follow-up. J Clin Endocrinol Metab. 2019 Mar 15;104(9):4087–100.
4. Tuttle RM, Fagin JA, Minkowitz G, Wong RJ, Roman B, Patel S, Untch B, Ganly I, Shaha AR, Shah JP, Pace M, Li D, Bach A, Lin O, Whiting A, Ghossein R, Landa I, Sabra M, Boucai L, Fish S, Morris LGT. Natural History and Tumor Volume Kinetics of Papillary Thyroid Cancers During Active Surveillance. JAMA Otolaryngol Head Neck Surg. 2017 Oct 1;143(10):1015-1020.
5. Miyauchi A. Clinical Trials of Active Surveillance of Papillary Microcarcinoma of the Thyroid. World J Surg. 2016 Mar;40(3):516-22.
6. Ito Y, Miyauchi A, Inoue H, Fukushima M, Kihara M, Higashiyama T, Tomoda C, Takamura Y, Kobayashi K, Miya A. An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J Surg. 2010 Jan;34(1):28-35.
7. ATA Thyroid Patient Information- Microcarcinomas of the Thyroid Glandhttps://www.thyroid.org/microcarcinomas-thyroid-gland/
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #CancerSurgeon #ThyroidCancer #SurgicalOncologist #CASO #CenterforAdvancedSurgicalOncology
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #HeadandNeckSurgeon #CancerSurgeon #MultinodularGoiter #Goiter #SubsternalGoiter #CervicalGoiter #CASO #CenterforAdvancedSurgicalOncolgy
