My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
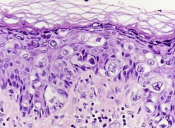
The clinical hallmarks of Paget’s disease of the breast are:
Scaling, erythema, and / or ulceration of the nipple sometimes extending to the areola
Because the main differential diagnosis for this clinical presentation is eczema:
A short course of topical steroids is an appropriate initial step:
Failure to resolve should prompt tissue biopsy by punch or wedge technique and not additional steroid therapy
Pathology revealing adenocarcinoma cells within the epidermis (Paget cells):
Confirms the diagnosis
HER2 amplification:
Is found in 60% to 90% of cases of Paget’s disease of the breast:
But the patient should be fully evaluated prior to making decisions regarding the need for targeted therapy
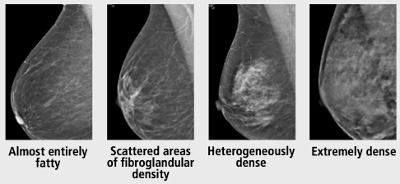
Appropriate diagnostic imaging includes:
Mammography, ultrasound, and / or breast MRI:
As Paget’s disease is associated with an underlying malignancy 85% of the time
The appropriate surgical management of Paget’s disease is:
Breast conservation with central mastectomy (resection of the nipple-areolar complex) with resection of the primary tumor and irradiation or mastectomy
References
Chen CY, Sun LM, Anderson BO. Paget disease of the breast: changing patterns of incidence, clinical presentation, and treatment in the U.S. Cancer. 2006;107(7):1448-1458.
Killelea BK, Chagpar AB, Horowitz NR, Lannin DR. Characteristics and treatment of human epidermal growth factor receptor 2 positive breast cancer: 43,485 cases from the National Cancer Database treated in 2010 and 2011. Am J Surg. 2017;213(2):426-432.
Caliskan M, Gatti G, Sosnovskikh I, et al. Paget’s disease of the breast: the experience of the European Institute of Oncology and review of the literature. Breast Cancer Res Treat. 2008;112(3):513-521.
Three important conclusions are agreed upon regarding this clinical entity:
Prognosis of occult primary breast cancer is the same or slightly better than women with classic stage IIA disease (T0, N1, M0)
An exhaustive workup for the non-breast primary is usually not fruitful
Treatment of the breast in some manner decreases the risk of local failure over time
Modified radical mastectomy has been the traditional surgical treatment for many years
Previously, the primary breast cancer was found in the mastectomy specimen:
40% to 80% of the time, but with the advent of much better mammography and ultrasound along with breast MRI, this rate is much lower now
However, what was true then and still holds today:
Is that no treatment to the breast itself results in an unacceptably high local recurrence rate
An alternative to a modified radical mastectomy:
Is complete ALND followed by whole-breast irradiation
Axillary dissection:
Provides local control while also fine tuning staging
Theoretically the whole-breast radiation:
Should control any subclinical disease in the breast not detected on imaging
Primary radiation to the breast, axilla, and supraclavicular area without any surgery of the breast or axilla:
Results in higher local and regional recurrence compared to surgery and radiation combined
Axillary node dissection and whole-breast irradiation:
Has been found to have equivalent survival as a modified radical mastectomy
A recent meta-analysis of 7 studies and more than 240 patients with occult primary breast cancers (0.3% to 0.8% of all breast cancers):
Found 39% were treated with ALND and radiation while 47% had modified radical mastectomy and 15% had ALND alone
With a mean follow-up of 5 years:
The study found no difference in local regional recurrence (12.7% vs 9.8%), distant metastasis (7.2% vs 12.7%), or mortality (9.5% vs 17.9%) between ALND and radiation vs modified radical mastectomy (all p>0.16)
ALND with radiation was superior to ALND alone in terms of local regional recurrence (12.7% vs 34.3%, p < 0.01) and trended towards improved survival but this was not statistically significant (P=0.09)
References:
Barton SR, Smith IE, Kirby AM, Ashley S, Walsh G, Parton M. The role of ipsilateral breast radiotherapy in management of occult primary breast cancer presenting as axillary lymphadenopathy. Eur J Cancer. 2011;47:2099-2106. PMID: 21658935. http://www.ncbi.nlm.nih.gov/pubmed/21658935
Macedo FI, Eid JJ, Flynn J, Jacobs MJ, Mittal VK. Optimal surgical management for occult breast carcinoma: a meta-analysis. Ann Surg Oncol. 2016;23:1838-1844. https://www.ncbi.nlm.nih.gov/pubmed/26832884
Rueth NM, Black DM, Limmer AR, et al. Breast conservation in the setting of contemporary multimodality treatment provides excellent outcomes for patients with occult primary breast cancer. Ann Surg Oncol. 2015;22:90-95. [epub ahead of print]. http://www.ncbi.nlm.nih.gov/pubmed/25249256
Walker GV, Smith GL, Perkins GH, et al. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis. Cancer. 2010;116:4000-4006. PMID: 20564117. http://www.ncbi.nlm.nih.gov/pubmed/20564117
Woo SM, Son BH, Lee JW, et al. Survival outcomes of different treatment methods for the ipsilateral breast of occult breast cancer patients with axillary lymph node metastasis: a single center experience. J Breast Cancer. 2013;16:410-416. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3893343/
The Society of Surgical Oncology – American Society for Radiation Oncology (SSO-ASTRO) 2014 Consensus Guidelines:
Regarding margins of resection for invasive carcinoma of the breast:
Recommend the use of “no ink on tumor” as the standard
Patients with invasive cancer, even with associated ductal carcinoma in situ (DCIS):
Are treated according to these guidelines
In a meta-analysis of 33 studies including 32,363 patients:
Odds of local recurrence were associated with margin status of positive vs. negative:
But not decreased with increasing margin distance for patients with invasive carcinoma
The study reported that rates of in-breast tumor recurrence are twice as high with positive marginsregardless of tumor biology, radiation boost, or endocrine therapy
There was no evidence that wide margins reduce recurrence, even in patients with extensive intraductal component
However, the American Society of Clinical Oncology (ASCO) guidelines recommend consideration of post-excision mammography to document adequate resection in patients with microcalcifications
References
Moran MS, Schnitt SJ, Giuliano AE, et al. SSO-ASTRO consensus guideline on margins for breast-conserving surgery with whole breast irradiation in stage I and II invasive breast cancer. Int J Radiat Oncol Biol Phys. 2014;88(3):553-564.
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21(3):717-730.
Buchholz TA, Somerfield MR, Griggs JJ, et al. Margins for breast-conserving surgery with whole-breast irradiation in stage I and II invasive breast cancer: American Society of Clinical Oncology endorsement of the Society of Surgical Oncology/American Society for Radiation Oncology consensus guideline. J Clin Oncol. 2014;32(14):1502-1506.
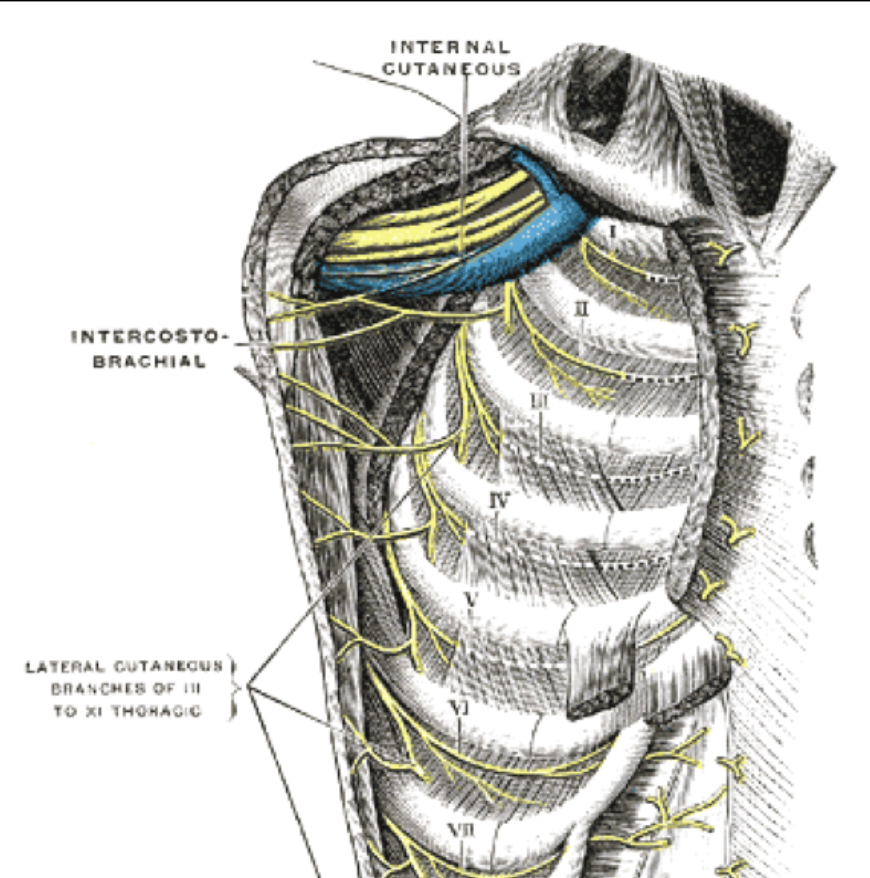
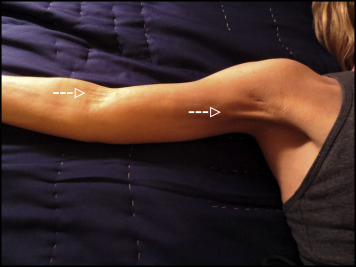
The symptoms of neuropathy are due to injury of the intercostobrachial nerve:
This nerve is a cutaneous branch of the intercostal nerves:
Most commonly the second intercostal nerve:
Which gives off a lateral cutaneous nerve:
Which continues as the intercostobrachial nerve
The intercostal nerves arise from the anterior rami of the thoracic spinal nerves
The intercostobrachial nerve pierces the serratus anterior, and crosses the axilla to the medial side of the upper arm:
The intercostobrachial nerve is commonly in the surgical field during axillary lymph node dissections and may be severed during surgery, or subject to traction or postsurgical inflammation:
Thus leading to intercostobrachial neuralgia
The larger intercostal nerves can be preserved with meticulous dissection
Neuropathic symptoms:
May be limited to numbness or tingling, but may also include a burning sensation
Techniques such as a regional nerve block have been described to alleviate symptoms in severe cases
In a study of 200 patients who underwent axillary dissection:
76% had symptoms of intercostobrachial neuralgia postoperatively:
Of these patients, 82% reported improvement or resolution of these symptoms within 1 year:
Reflecting the richness of the sensory nerve supply to the axilla and upper arm
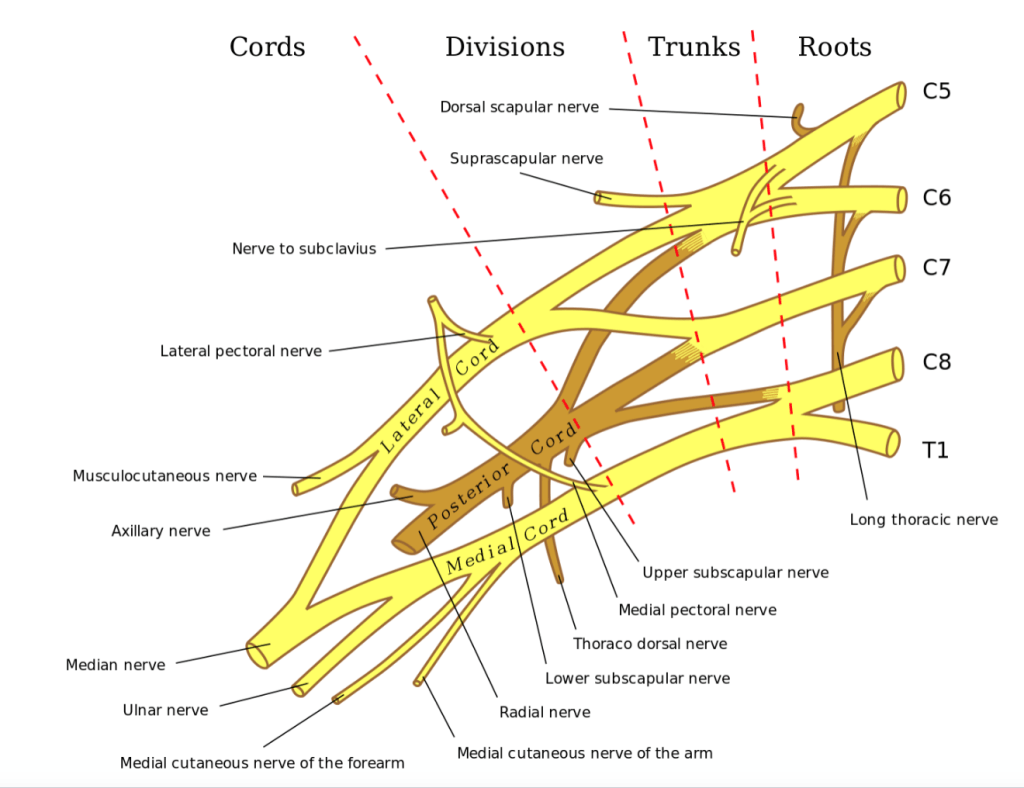
The thoracodorsal nerve:
Is a branch of the posterior cord of the brachial plexus:
Supplies motor function to the latissimus dorsi
If injured:
Patients experience weakness with arm abduction, lateral flexion, and difficulty with activities such as climbing, swimming, and using the arms to pull the body up
The medial cord of the brachial plexus gives rise to the medial pectoral nerve:
Which innervates both the pectoralis minor muscle and the pectoralis major muscle
The medial pectoral nerve typically pierces the pectoralis minor muscle, but may wrap around the lateral aspect of the pectoralis minor before traveling on to innervate the distal pectoralis major muscle
The lateral cord of the brachial plexus:
Gives rise to the lateral pectoral nerve, which innervates the pectoralis major muscle
This nerve travels along the medial border of the pectoralis minor muscle, and then along the undersurface of the pectoralis major muscle along with the pectoral branch of the thoracoacromial artery to supply the proximal pectoralis major muscle
The medial pectoral nerve bundle is often encountered during axillary dissection, as it is located lateral to the lateral pectoral nerve
If either of these nerves is injured, pectoralis muscle atrophy can occur, which can present as a late complication of surgery:
With weakness of shoulder adduction, interior rotation, and flexion
The long thoracic nerve:
Typically arises from anterior rami of the cervical spinal nerve roots C5 to C7:
It courses along the chest wall and supplies the serratus anterior muscle
Injury to this nerve causes a winged scapula
References
Sclafani LM, Baron RH. Sentinel lymph node biopsy and axillary dissection: added morbidity of the arm, shoulder and chest wall after mastectomy and reconstruction. Cancer J. 2008;14(4):216-222.
Wisotzky EM, Saini V, Kao C. Ultrasound-guided intercostobrachial nerve block for intercostobrachial neuralgia in breast cancer patients: a case series. Prev Med Rep, 2016;8(3):273-277.
Roses DF, Brooks AD, Harris MN, Shapiro RL, Mitnick J. Complications of level I and II axillary dissection in the treatment of carcinoma of the breast. Ann Sur. 1999;230(2):194-201.
Porzionato A, Macchi V, Stecco C, Loukas M, Tubbs RS, De Caro R. Surgical anatomy of the pectoral nerves and the pectoral musculature. Clin Anat. 2012;25(5):559-575.
The administration of neoadjuvant chemotherapy (NAC) offers several advantages in locally advanced breast cancer:
It allows for down staging the disease:
Which can potentially allow for less extensive surgery in the breast and axilla
It also provides information regarding the responsiveness of the cancer to systemic therapy while the tumor remains in vivo:
Which can guide the course of therapy
Administering chemotherapy in the neoadjuvant vs. adjuvant setting:
Does not change overall survival:
As demonstrated in the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-18 and NSABP B-27 trials
The patient’s response to chemotherapy:
Does offer prognostic information:
Particularly in patients with hormone receptor negative (HR-) disease
Patients who achieve pathologic complete response (pCR):
Which is typically defined as no residual invasive disease in the breast or axilla:
Appear to have improved event-free survival (EFS) and overall survival (OS) compared with patients with residual disease:
This finding was demonstrated by a recent meta-analysis that included 36 studies including 5,768 patients with HER2 positive breast cancer
This correlation was strongest in patients with HR- disease
Further, among patients with HER2 positive disease that do not have a pCR:
The degree of residual cancer burden appears to correlate with outcomes
Patients with HER2 positive tumors:
May complete up to one year of HER2-targeted therapy:
With trastuzamab ± pertuzamab.
When planning surgery:
The pre-treatment volume does not need to be excised if the tumor has responded to chemotherapy:
However if multifocal disease is present:
The satellite lesion(s) should be localized and excised with the index lesion
When considering the appropriateness for breast conservation following NAC:
The distance between the lesions, location, and breast size must be considered
Placement of clips in the index lesion and any satellite lesions prior to initiation of NAC is critical for appropriate surgical planning post-NAC
References
Rastogi P, Anderson SJ, Bear HD. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol. 2008; 10;26(5):778-785.
Broglio KR, Quintana M, Foster M, et al. Association of pathologic complete response to neoadjuvant therapy in HER2-positive breast cancer with long-term outcomes: a meta-analysis. JAMA Oncol. 2016;2(6):751-760.
Symmans WF, Wei C, Gould R, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35(10):1049-1060.
Boughey JC, Peintinger F, Meric-Bernstam F, et al. Impact of preoperative versus postoperative chemotherapy on the extent and number of surgical procedures in patients treated in randomized clinical trials for breast cancer. Ann Surg. 2006;244(3):464-470.
Multiple ipsilateral breast cancers (MIBC) include:
Both multifocal and multicentric disease
The term multifocal (MF):
Typically refers to two or more foci of disease within a single quadrant of the breast,
Multicentric (MC):
Refers to two or more foci in more than one quadrant of the breast
When staging:
An “m” modifier, is added to TNM classification to identify MF / MC disease
In the setting of MIBC:
The size of the largest focus is used for staging:
Rather than a cumulative measurement of the tumor sizes
Historically, it was believed that multiple ipsilateral breast cancers should be treated surgically with mastectomy:
This thought is based on early retrospective studies (1980s-90s):L
That reported a higher locoregional recurrence (LRR) in patients with MF / MC disease who underwent breast conserving therapy (BCT)
More current studies, which include patients treated in a contemporary multidisciplinary setting:
Have demonstrated a more promising role for BCT in MF / MC disease
A systematic review included six retrospective studies evaluating patients with multiple ipsilateral breast cancers undergoing BCT vs. mastectomy:
The rate of LRR overall was 2% to 23% for BCT:
With similar rates of LRR for BCS compared to mastectomy
The largest of these compared 887 patients who underwent mastectomy vs. 300 who underwent BCT:
And found that BCT was not inferior to mastectomy:
With respect to:
5-year (2.5% vs. 4.5%) LRR
10-year (6.5% vs 5.7%) LRR
In a study reviewing surgical management of 6,134 patients undergoing neoadjuvant chemotherapy:
1,401 (23%) were found to have MF / MC disease
617 patients (44%) underwent BCT
Local recurrence-free survival, disease-free survival (DFS), and overall survival (OS):
We’re not inferior in patients with MF / MC compared with unifocal disease:
If negative margins or a pathologic complete response was obtained
In a study evaluating 110 patients with MF / MC disease compared to 263 matched-case controls with unifocal disease:
MF / MC disease had worse local control and DFS:
But was not impacted by the type of surgery performed
The heterogeneity of findings related to the management of multiple ipsilateral breast cancers underscores the need for a prospective clinical trial to address this issue:
The Alliance Z11102 prospective trial aimed to evaluate the feasibility and safety of breast conservation in women with multiple ipsilateral breast cancers:
Defined as having tumors separated by 2 cm or more of normal breast tissue:
The authors found that of the 198 patients enrolled:
93% underwent successful lumpectomy:
67% underwent lumpectomy in a single operation
Conversion to mastectomy occurred in 7.1% of patients due to positive margins
Primary endpoint is LRR at 5 years, and these results will be forthcoming as the data mature
Thus, based on available data:
MF / MC is not an absolute contraindication to BCT
Oncoplastic techniques:
Can be considered as needed for an improved cosmetic outcome, with high rates with disease-free survival and low risk of local recurrence
Chemotherapy can be given as her primary treatment:
Which may improve her surgical options
References
Kurtz JM, Jacquemier J, Amalric R, et al. Breast-conserving therapy for macroscopically multiple cancers. Ann Surg. 1990;212(1):38-44.
Winters ZE, Horsnell J, Elvers KT et al. Systematic review of the impact of breast-conserving surgery on cancer outcomes of multiple ipsilateral breast cancers. BJS Open. 2018;2(4):162-174. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6069349/. Accessed August 25, 2019.
Yerushalmi R, Tyldesley S, Woods R, et al. Is breast-conserving therapy a safe option for patients with tumor multicentricity and multifocality? Ann Oncol. 2012;23(4):876-881.
Ataseven B, Lederer B, Blohmer JU, et al. Impact of multifocal or multicentric disease on surgery and locoregional, distant and overall survival in 6134 breast cancer patients treated with neoadjuvant chemotherapy. Ann Surg Oncol. 2015;22(4):1118–1127.
Shaikh T, Tam T, Li T, et al. Multifocal and multicentric breast cancer is associated with increased local recurrence regardless of surgery type. Breast J. 2015;21(2):121-126.
Rosenkranz, K.M., Ballman, K., McCall, L. et al. The feasibility of breast-conserving surgery for multiple ipsilateral breast cancer: an initial report from ACOSOG Z11102 (Alliance) Trial. Ann Surg Oncol. 2018;25(10):2858-2866.
De La Cruz L, Blakenship SA, Chatterjee A, et al. Outcomes after oncoplastic breast-conserving surgery in breast cancer patients: a systematic literature review. Ann Surg Oncol. 2016;23(10):3247-3258.
Rastogi P, Anderson SJ, Bear HD. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol. 2008;10;26(5):778-785.
Fisher B, Anderson S, Bryant J, et al. Twenty-year followup of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. New Engl J Med. 2002;347(16):1233-1241.
Litiere S, Werutsky G, Fentiman IS, et al. Breast-conserving therapy versus mastectomy for stage I-II breast cancer: 20 year followup of the EORTC 10801 phase 3 randomized trial. Lancet Oncol. 2012;13(4):412-419.
Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. New Engl J Med. 2002;347(16):1227-1232.
Is characteristically spontaneous, unilateral, uniductal, or bloody
Physiologic discharge is:
Nonspontaneous, bilateral, multiductal, and milk
The most common causes for pathologic nipple discharge are benign:
Intraductal papillomas
Duct ectasia)
The presence of abnormal clinical findings on imaging or physical exam:
Is associated with increased risk of malignancy:
38% vs. 2%
Contemporary workup for nipple discharge includes:
Mammography and evaluation of the retroareolar region with ultrasound
Patients with normal findings on mammography, ultrasound, and physical exam can be further evaluated with breast MRI:
As it is highly sensitive and specific for cancer
Surgical management of nipple discharge includes:
Excision of a single duct or central duct apparatus:
Depending on the number of ducts involved
References
Li GZ, Wong SM, Lester S, Nakhlis F. Evaluating the risk of underlying malignancy in patients with pathologic nipple discharge. Breast J. 2018;24(4):624-627.
de Paula IB, Campos AM. Breast imaging in patients with nipple discharge. Radiol. Bras. 2017;50(6):383-388.
Yilmaz R, Bender O, Celik Yabul F, Dursun M, Tunaci M, Acunas G. Diagnosis of nipple discharge: value of magnetic resonance imaging and ultrasonography in comparison with ductoscopy. Balkan Med J. 2017;34(2):119-126.
Appears to be a common complication following axillary surgery
It consists of the appearance of a visible web of axillary skinoverlying palpable cords of tissue:
That are made taut and painful by shoulder abduction
These cords can result in painful abduction of the shoulder and reduced range of motion
It typically results from axillary lymphadenectomies for treatment of breast cancer or melanoma
In general, axillary web syndrome is poorly defined and misunderstood:
In a large systematic review:
The incidence ranged from 0.6% to 85.4%
Risk factors:
Extent of surgery (number of nodes removed)
Low body mass index
Age
Although smoking, receipt of neoadjuvant chemotherapy, and radiation may play a role in its development:
These factors have not been described in the literature
In the majority of cases, axillary web syndrome:
Appears to develop within 2 to 8 weeks of axillary surgery
Although patients generally do well with resolution of their symptoms:
Current evidence for the treatment of axillary web syndrome is insufficient to provide clear guidance for clinical practice
Suggested interventions have included:
Early education
Physiotherapy
Thermal therapy
Medications
Surgery
References
Koehler LA, Haddad TC, Hunter DW, Tuttle TM. Axillary web syndrome following breast cancer surgery: symptoms, complications and management strategies. Breast Cancer. 2018;11:13-19.
Yeung WM, McPhail SM, Kuys SS. A systematic review of axillary web syndrome (AWS). J Cancer Surviv. 2015;9(4):576-598
Current consensus guidelines from the American Society of Breast Surgeons:
Do not recommend CPM for women with sporadic breast cancers
A Cochrane review of eight studies evaluating patients who underwent CPM:
Concluded that while CPM reduces risk of contralateral breast cancer:
It is not associated with improved survival
Reasons for not recommending CPM include:
A low estimated risk of cancer in the contralateral breast:
2% to 6% over 10 years)
Increased complication rates
Studies showing that CPM does not improve survival or recurrence from the index cancer
References
Lostumbo L, Carbine N, Wallace J, Ko H. Prophylactic mastectomy for the prevention of breast cancer. Cochrane Database Syst Rev 2004(4):CD002748.
Boughey JC, Attai DJ, Chen SL, et al. Contralateral prophylactic mastectomy consensus statement from the american society of breast surgeons: additional considerations and a framework for shared decision making. Ann Surg Oncol. 2016;23(10):3106-3111.