My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
👉Anaplastic thyroid cancer T4A- OS 15.8months T4B- OS 6.1months T4C – OS 2.8 months
Onoda N, Sugitani I, Ito KI, Suzuki A, Higashiyama T, Fukumori T, et al. Evaluation of the 8th edition TNM classification for anaplastic thyroid carcinoma. Cancers. 2020;12:1–11.
Rodrigo Arrangoiz MS, MD, FACS cirujano de tumores de cabeza y cuello / cirugia endocrina / cirugía oncológica es experto en el manejo de patología de la glándula tiroides.
Su entrenamiento fue el siguiente:
• Cirugia general y gastrointestinal:
• Michigan State University:
• 2004 al 2010• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012• Maestria en ciencias (Clinical research for healthprofessionals):
• Drexel University (Filadelfia):
• 2010 al 2012• Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016
The evaluation of patients with thyroid nodules requires adequate stratification to estimate the risk of thyroid cancer:
Evaluation also requires an understanding of the patient’s situation
To assist clinicians in this task, multiple thyroid nodule sonographic risk-stratification systems (RSSs) have been developed, including:
The American Thyroid Association (ATA) system
The American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS)
The Korean Thyroid Imaging Reporting and Data System (K-TIRADS)
The European Thyroid Imaging Reporting and Data System (EU-TIRADS)
The Artificial Intelligence Thyroid Imaging Reporting and Data System (AI TI-RADS)
In general, studies assessing the performance of these RSSs have been retrospective and have included patients who have undergone a diagnostic intervention (i.e., thyroid nodule biopsy or surgery):
This type of study design can introduce bias into the assessment of diagnostic properties by increasing the proportion of high risk cases
Although RSSs for thyroid nodules aim to standardize thyroid cancer risk assessment and recommendations:
The ACR TI-RADS is associated with a lower number of recommendations for thyroid biopsy:
This is due, in part, to the system’s relatively more conservative thresholds for recommending thyroid biopsy
In the current study, a comparison of thyroid nodule RSSs is evaluated:
In thyroid nodule risk distribution in an unselected group of patients undergoing thyroid ultrasound
By assessing the impact of risk distribution, in addition to the size thresholds, on biopsy recommendations
Methods:
This was a multi-institutional study of seven radiology practices that participate in the ACR registry
Each practice prospectively submitted thyroid ultrasound reports on adult patients between October 2018 and March 2020
Sites provided the maximum size of the thyroid nodules and followed structured reporting according to the five ACR TI-RADS ultrasound features
Patients with thyroid cancer, nodule size less than 5 mm or greater than 5 cm, and incomplete / unrealistic data were excluded
The submitted reports were then retrospectively categorized following the criteria of ACR TI-RADS, the ATA system, K-TIRADS, EU-TIRADS, and AI TI-RADS
The distribution of risk categories and thyroid biopsy recommendation rates were compared
Because of the large sample size, even small differences in the proportions observed were expected to be statistically significant
Results:
The study population consisted of:
12,208 patients, mostly women (84%), encompassing a total of 27,933 thyroid nodules
The mean patient age was 60.7 years, and the mean (±SD) nodule size was 1.5 ± 0.92 cm
There were 1896 nodules that could not be classified according to the ATA system
Placed more nodules in the TR2 category (8.2% and 10%, respectively) than the other systems (range, 1.2%–2.5%)
EU-TIRADS:
Placed more nodules in the high suspicion / TR5-equivalent category (18.9%) than did the other systems (range, 9.1–12.5%)
AI TI-RADS had the lowest level of TR3 nodules (26.1%) as compared with the other systems (range, 31–44.4%)
In all, the most common category for all nodules was TR4 and its equivalents (42.1–48.3%)
ACR TI-RADS recommended biopsies in 29.1% of the thyroid nodules:
One of the lowest rates as compared with other systems (ATA, 58.7%; EU-TIRADS, 38.9%; K-TIRADS, 57%)
AI TI-RADS recommended biopsy for 26.3% of the nodules
Finally, when evaluating thyroid biopsy recommendations according to risk category:
The rate of recommended biopsy was similar in the TR5 categories and equivalents (68.7–75.5%)
There was variability for TR2:
With ACR TI-RADS recommending biopsy in 0% of the nodules (range for others, 2.8–17.7%)
The largest differences were for TR3 and TR4 nodules:
For which ACR TI-RADS and AI TI-RADS recommended biopsy in 19.0% to 22.3% and 32.7% to 33.7 %, respectively; the range for the other systems was 33.3 to 53.7% for TR3 and 29.0 to 64.0% for TR4
Conclusions:
Differences in the distribution of sonographic thyroid nodule risk categories and biopsy size thresholds among the various RSSs contribute to variability in clinical recommendations for thyroid biopsies
ACR TI-RADS generally recommends a lower number of biopsies:
Because of a combination of its risk assignment criteria and more conservative biopsy thresholds
This large multi-center study validates the clinical utility of thyroid nodule risk stratification:
By evaluating patients who underwent thyroid ultrasound regardless of their diagnostic workup
Using ACR TI-RADS, 11.3% of the thyroid nodules were considered either benign or very low risk for thyroid cancer, while 9.4% were considered high risk
Most patients had nodules considered either T3 or T4 (31.0% and 48.3%, respectively)
This distribution highlights the importance of high-quality ultrasound risk stratification in the evaluation of patients with thyroid nodules, as it can facilitate reassurance in patients with low-risk nodules
Similarly, a robust RSS may appropriately justify the consideration of biopsy in those at higher ris
In addition, the study evaluated the impact of size thresholds across the different risk categories to guide the need for thyroid biopsies
Application of ACR TI-RADS was associated with a biopsy rate of 29.1%:
Lower than that for all the other systems except for AI TI-RADS
This was driven, in part:
By fewer biopsy recommendations for nodules in categories TR3 and TR4
As well as a greater proportion of nodules in the TR2 category:
For which biopsy is not recommended
Taken together, these findings suggest that, in addition to different size thresholds for biopsy, the distribution of risk categories affects biopsy recommendation rates
In fact, the overall proportion of nodules recommended for biopsy varied between the systems, from 26.3% in AI TI-RADS to 58.7% in the ATA system
These findings highlight the urgent need for and value of current efforts to harmonize thyroid nodule RSSs, particularly in terms of risk-category definitions and management recommendations by malignancy estimates and size thresholds for biopsy
This endeavor might be challenging, given that clinical evidence that can guide the selection of biopsy size thresholds is limited
More importantly, in this large study, most nodules were categorized as TR3 or TR4, and overall the mean nodule size was 1.5 cm, representing a group of patients in whom management recommendations by the major RSSs are highly variable
These findings underscore the value of a care model that uses the best available evidence to understand thyroid cancer risk and supports the collaboration of patients and clinicians when deciding how to respond to this risk
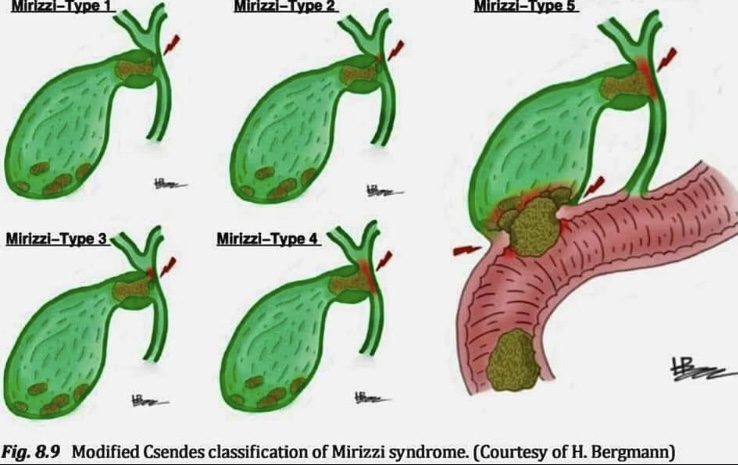
-Mirizzi syndrome is subclassified in to 5 types :
🔴𝗜: Is obstruction of the extrahepatic bile duct stone/s in the Hartmann’s pouch or cystic duct.
🔴𝗜𝗜: Is with a cholecystocholedochal fistula (diameter < 1/3 or the common hepatic duct wall).
🔴𝗜𝗜𝗜: Is with a cholecystocholedochal fistula (diameter < 2/3 of the common hepatic duct wall).
🔴𝗜𝗩: Is with a cholecystocholedochal fistula (involving the whole common hepatic duct wall).
🔴𝗩: Any type associated with a cholecystoenteral fistula (i.e,fistula to stomach, duodenum or hepatic flexure or transverse colon). This is sometimes sub-classiied depending on whether gallstone ileus is present or not.
In a phase III randomized trial in patients with unresectable, locally advanced, or metastatic MTC (n = 331):
Vandetanib increased PFS when compared with placebo (HR, 0.46; 95% CI, 0.31– 0.69; P < .001)
OS data are not yet available
A post-hoc subgroup analysis including 184 patients with symptomatic and progressive disease at baseline:
Also showed increased PFS (HR, 0.43; 95% CI, 0.28–0.64; P < .001) in patients who received vandetanib, compared to the placebo:
Although time to worsening pain was not significantly different between the two groups (HR, 0.67; 95% CI, 0.43–1.04; P = .07)
In this subgroup, the overall response rate (ORR) was:
37% in the patients who received vandetanib and 2% in patients who received the placebo (P < .001)
The FDA approved the use of vandetanib for patients with locally advanced or metastatic MTC:
Who are not eligible for surgery and whose disease is causing symptoms or growing:
However, access is restricted through a vandetanib Risk Evaluation and Mitigation Strategy (REMS) program:
Because of potential cardiac toxicity
The NCCN Panel recommends vandetanib (category 1):
As a preferred option for patients with recurrent or persistent MTC
Cabozantinib:
Is a multi-targeted kinase inhibitor:
That inhibits:
RET
VEGFR2
MET
In a phase 3 randomized trial (EXAM) in patients with locally advanced or metastatic MTC (n = 330):
Cabozantinib increased median PFS when compared with placebo:
11.2 vs. 4.0 months:
HR, 0.28; 95% CI, 0.19–0.40; P < .001
Following long-term follow-up:
The median OS for patients treated with cabozantinib was:
26.6 months compared to 21.1 months for placebo:
Although this difference was not statistically significant (stratified HR, 0.85; 95% CI, .64–1.12, P = .24)
Exploratory analyses have suggested that cabozantinib:
May have a greater clinical benefit:
For medullary thyroid cancers harboring:
RET M918T or RAS mutations:
Although prospective trials are needed to confirm
In 2012:
The FDA approved the use of cabozantinib for patients with progressive, metastatic MTC
The NCCN Panel recommends cabozantinib (category 1):
As a preferred option based on the phase III randomized trial and FDA approval
Rare adverse events with cabozantinib include:
Severe bleeding and gastrointestinal perforations or fistulas:
Severe hemorrhage is a contraindication for cabozantinib
RET mutations account for a significant percentage of MTC cases:
Supporting investigation into the impact of recently developed RET inhibitors on RET-mutated MTC
The phase I–II LIBRETTO-001 study:
Evaluated the efficacy of the RET inhibitor selpercatinib in 143 patients with RET-mutant MTC in patients previously treated with vandetanib or cabozantinib (n = 55):
The ORR and 1-year PFS rates were:
69% (95% CI, 55%–81%) and 82% (95% CI, 69%–90%), respectively
In patients with no previous vandetanib or cabozantinib treatment (n = 88):
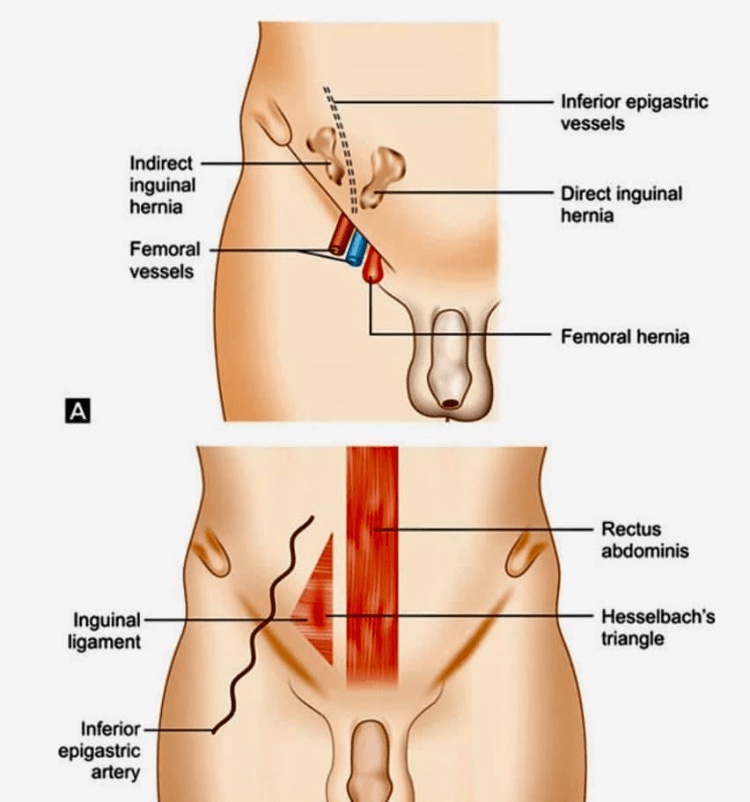
Busoga hernias, also known as Gill-Ogilvie hernias
🔴They are a variant of the direct inguinal hernia involving the conjoint tendon.
🔴Busoga herniae have been noted to occur most commonly in young, athletic men with a well-developed abdominal musculature. There is an increased incidence of Busoga hernia in Uganda.
🔴The conjoint tendon medially reinforces the posterior wall of the inguinal canal. It is protrusion here, at the medial aspect of the posterior aspect of the inguinal canal were weakening can result in herniation. Weakening in the conjoint tendon is thought to be secondary to rigorous training, with kicking, running, and sharp turns
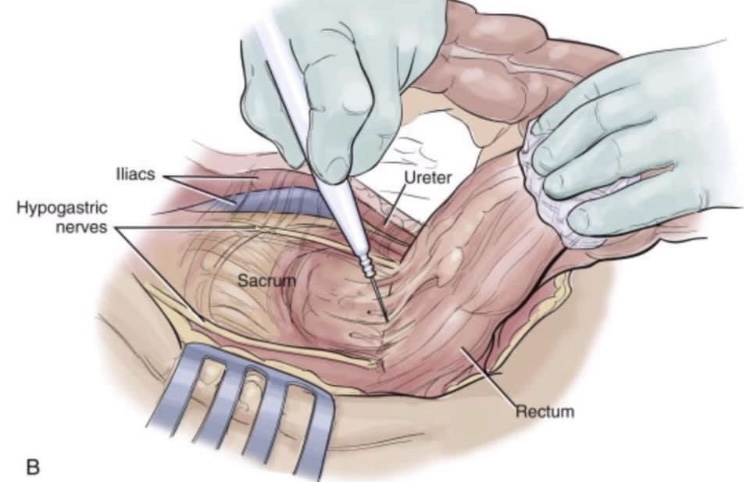
🔴Dissection is along the avascular alveolar plane between the presacral and mesorectal fascia, described as holy plane (Heald’s “holy plane”).
🔴The mesorectum refers to a fatty connective tissue layer, measuring 2–3 cm in thickness, with associated vessels, lymphatics and lymph nodes, which surrounds the rectum and is enveloped by fascia.
🔴mesorectal dissection occurs in a total avascular plane that, once identified, can be easily dissected, exposing ‘the white side of the yellow’ as Heald first described in 1979. As the posterior dissection continues downward, the mesorectum looks more and more bilobate (indicating a good quality of the dissection) until it thins out and disappears. Once again traction and counter traction are essential in lateral and anterior resection to identify the dissection plane.
🔴The relationship of the rectum and pelvic autonomic nerves during open surgery when standing on the patient’s left. The ligation of the inferior mesenteric artery should be performed 1.5–2 cm from its origin from the aorta to avoid damaging the superior hypogastric plexus. At the pelvis, for posterior and lateral tumours, dissection should be directed below the Denonvillliers fascia to avoid damaging the neurovascular bundles that run along the tip of the seminal vesicle (2 and 10 o’clock directions).
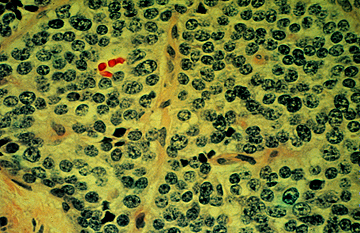
Surgical specimens from patients with MTC show spindle-shaped and frequently pleomorphic cellswithout follicle development because these cells originate from the calcitonin-producing parafollicular C cells of the thyroid
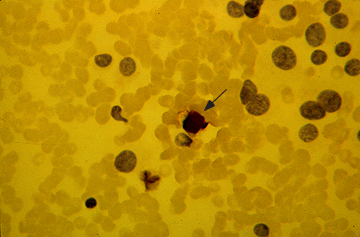
Fine-needle aspirate with immunostaining for calcitonin in medullary cancer of the thyroid. The nuclei of the tumor cells are placed eccentrically and are larger and more pleomorphic than those of normal follicular cells. Immunocytologic staining for calcitonin is positive (brown staining, which is best seen at the arrow). The background contains many red cells that nonspecifically take up the stain.
 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Maestria en ciencias (Clinical research for healthprofessionals):
• Maestria en ciencias (Clinical research for healthprofessionals): • Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina