My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Published in 2003 the evaluation of combination chemotherapy for breast cancer:
Given by both dose dense and sequential therapy
The goal of the study was to evaluate the best way to administer the chemotherapy regimen:
Doxorubicin (A), cyclophosphamide (C) followed by paclitaxel (T)
The study assessed chemotherapy administration in:
A dose dense fashion:
Two weeks vs. three weeks
Treatment sequence:
Concurrent versus sequential
The findings of the study showed:
That dose density improved clinical outcomes significantly
Sequential chemotherapy was as effective as concurrent chemotherapy:
But required a longer time period of administration
Dose-dense chemotherapy:
Refers to decreasing the interval between cycles of treatment without the need of increasing doses and toxicity
Sequential therapy:
Refers to the administration of treatments one at a time rather than concurrently
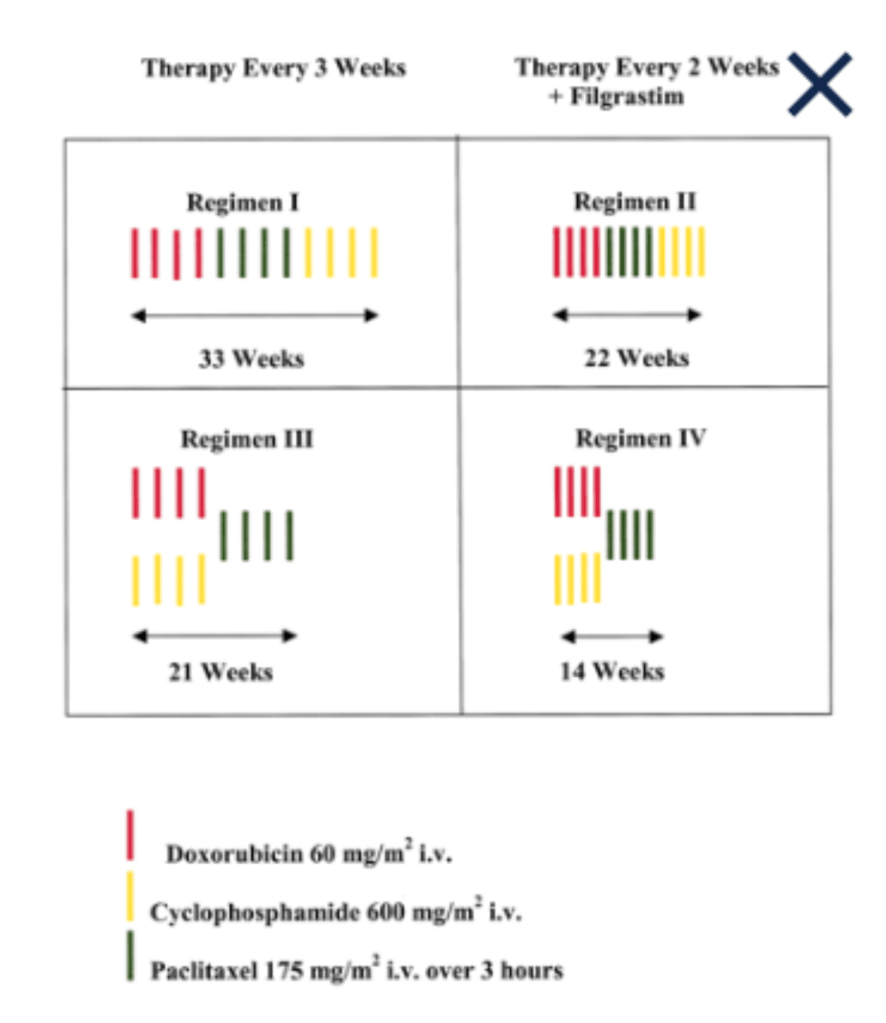
National Cancer Institute’s Breast Intergroup INT C9741 and CALGB 9741 trial:
Was a prospective, randomized trial designed to study adjuvant chemotherapy treatment regimens:
In women with axillary node-positive breast cancer conducted from September 1997 to March 1999
Doxorubicin (A), paclitaxel (T), and cyclophosphamide (C) were chosen for this study
Using a 2 x 2 factorial design, patients were assigned to receive one of the following 4 regimens:
Sequential A then C followed by T x 4 cycles every 3 weeks
Dose-dense, sequential A then C then T x 4 cycles every 2 weeks with filgrastim
Concurrent AC x 4 cycles followed by T x 4 cycles every 3 weeks
Dose-dense, concurrent AC x 4 cycles followed by T x 4 cycles every 2 weeks with filgrastim
Results showed that:
Dose-dense treatment improved the primary endpoints of:
Disease-free survival (DFS) and overall survival (OS):
Four-year DFS was 82% for dose-dense regimens and 75% for other groups (risk ratio, 0.74, P=0.01)
Three-year OS was 92% for dose-dense regimens and 90% in other groups (risk ratio, 0.69, P=0.013)
There was no difference in either DFS or OS:
Between the concurrent and sequential schedules
Severe neutropenia:
Was less common in patients who received the dose-dense regimens
As a result of this study:
Dose-dense and concurrent AC chemotherapy has become one of the standard components of breast cancer therapy
References:
Citron ML, Berry DA, Cirrincione C, Hudis C, Winer EP, Gradishar WJ, et al. Randomized trial of dose-dense versus conventionally scheduled and sequential versus concurrent combination chemotherapy as postoperative adjuvant treatment of node-positive primary breast cancer: first report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J Clin Oncol.2003;21(8):1431-1439.
Orzano JA, Swain SM. Concepts and clinical trials of dose-dense chemotherapy for breast cancer. Clin Breast Cancer. 2005;6(5):402-411
Was a randomized, double-blind, placebo-controlled trial:
Comparing tamoxifen to placebo in women with node-negative ER positive invasive breast cancer
It demonstrated a statistically significant improvement in 10-year disease-free survival (DFS)with the use of 5 years of tamoxifen:
69% vs. 57%, P<0.0001
Tamoxifen was also associated with a 37% reduction in contralateral breast cancers
The results of B-14 raised questions about the benefit of administration of additional adjuvant hormonal therapy following completion of 5 years of tamoxifen:
More specifically, the administration of aromatase inhibitors after completion of tamoxifen therapy became of interest
NSABP B-33:
Was developed to compare exemestane with placebo in recurrence-free postmenopausal women who completed 5 years of tamoxifen therapy
Accrual to this study was terminated prematurely when results of NCIC-CTG MA.17 showed:
A significant improvement with letrozole after 5 years of tamoxifen
With a median follow-up of 64 months:
The hazard ratios of letrozole after 5 years of tamoxifen compared to placebo after similar tamoxifen therapy were:
0.52 (95% confidence interval [CI], 0.45 to 0.61; P<.001) for DFS
0.51 (95% CI, 0.42 to 0.61; P<.001) for distant DFS
0.61 (95% CI, 0.52 to 0.71; P<.001) for overall survival
The patients in NSABP B-33 were then unblinded and offered 5 years of exemestane:
The improvement in relapse-free survival observed in B-33 with exemestane was similar to that observed in the NCIC-CTG MA.17 trial with letrozole
To further examine the benefits of aromatase inhibitors as primary therapy or after 2 to 5 years of tamoxifen:
In women with early-stage, hormone receptor-positive breast cancer:
The MA.17 R trial analyzed prolonging duration of therapy to 10 years:
With DFS as the primary endpoint
The study randomized 1,918 women to placebo versus letrozole
After a median follow-up of 6.3 years:
DFS was 95% for the letrozole group and 91% for the placebo group
There was also an improvement in the annual incidence of contralateral breast cancer:
With the letrozole group at 0.21% versus 0.49% for the placebo group.
These data support a new standard of care for this patient population, i.e., to improve DFS through 10-year treatment with aromatase inhibitors
References:
Fisher B, Dignam J, Bryant J, Wolmark N. Five versus more than five years of tamoxifen for lymph node-negative breast cancer: updated findings from the National Surgical Adjuvant Breast and Bowel Project B-14 randomized trial. J Natl Cancer Inst. 2001;93(9):684-690.
Fisher B, Jeong JH, Dignam J, Anderson S, Mamounas E, Wickerham DL, et al. Findings from recent National Surgical Adjuvant Breast and Bowel Project studies in Stage I breast cancer. J Natl Cancer Inst Monogr. 2001;93(30):62-66.
Mamounas EP, Jeong JH, Wickerham DL, Smith RE, Ganz PA, Land SR, et al. Benefit from exemestane as extended adjuvant therapy after 5 years of adjuvant tamoxifen: intention-to-treat analysis of the National Surgical Adjuvant Breast and Bowel Project B-33 trial. J Clin Oncol. 2008;26(12):1965-1971.
Ingle JN, Tu D, Pater JL, Muss HB, Martino S, Robert NJ, et al. Intent-to-treat analysis of the placebo-controlled trial of letrozole for extended adjuvant therapy in early breast cancer: NCIC CTG MA.17. Ann Oncol. 2008;19(5):877-882.
Jin H, Tu D, Zhao N, Shepherd LE, Goss PE. Longer-term outcomes of letrozole versus placebo after 5 years of tamoxifen in the NCIC CTG MA.17 trial: analyses adjusting for treatment crossover. J Clin Oncol. 2012;30(7):718-721.
Lemieux J, Goss PE, Parulekar WR, Ingle JN, Pritchard KI, Robert NJ, et al. Patient-reported outcomes from MA.17R: a randomized trial of extending adjuvant letrozole for 5 years after completing an initial 5 years of aromatase inhibitor therapy alone or preceded by tamoxifen in postmenopausal women with early-stage breast cancer. J Clin Oncol. 2016;34(18
Several preclinical studies have demonstrated that tamoxifen acts not only by blocking the ER pathway, but also by:
Modulating the production of transforming growth factor-alpha and transforming growth factor-beta
By increasing the levels of sex hormone-binding globulin in serum
By increasing natural killer cell counts
By decreasing insulin-like growth factor
The NSABP protocol B-23:
Was developed to determine whether tamoxifen has a role in patients with ER negative cancer
Patients with ER negative tumors were randomized to:
Four cycles of adjuvant doxorubicin and cyclophosphamide (AC) or 6 cycles of adjuvant cyclophosphamide, methotrexate, and fluorouracil (CMF)with or without tamoxifen
The results of B-23 demonstrated:
No significant improvement in DFS or overall survival (OS) with tamoxifen added to chemotherapy:
DFS: CMF, 83%; CMF plus tamoxifen, 83%; AC, 83%; AC plus tamoxifen, 82%
OS: CMF, 89%; CMF plus tamoxifen, 89%; AC, 90%; AC plus tamoxifen, 91%
Additionally, protocol B-23 confirmed the results of protocol B-15:
That found that four cycles of AC are equivalent to 6 cycles of CMF in terms of DFS and OS
NSABP B-24 also demonstrated the effectiveness of tamoxifen only on ER positive ductal carcinoma in situ (DCIS), as did a study by Allred et al. on the risk reduction of a subsequent breast cancer in ER positive DCIS treated with tamoxifen
References:
Fisher B, Anderson S, Tan-Chiu E, Wolmark N, Wickerham DL, Fisher ER,et al. Tamoxifen and chemotherapy for axillary node-negative, estrogen receptor-negative breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-23. J Clin Oncol. 2001;19(4):931-942.
Wapnir IL, Dignam JJ, Fisher B, Mamounas EP, Anderson SJ, Julian TB, et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J Natl Cancer Inst. 2011;103(6):478-488.
Allred DC, Anderson SJ, Paik S, Wickerham DL, Nagtegaal ID, Swain SM, et al. Adjuvant tamoxifen reduces subsequent breast cancer in women with estrogen receptor-positive ductal carcinoma in situ: a study based on NSABP protocol B-24. J Clin Oncol. 2012;30(12):1268-1273.
The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-31 and the North Central Cancer Treatment Group (NCCTG) N9831 trials
In 2000, two landmark trialscombined results:
That compared adjuvant chemotherapy with or without concurrent trastuzumab therapy in women with surgically removed HER2-positive breast cancer
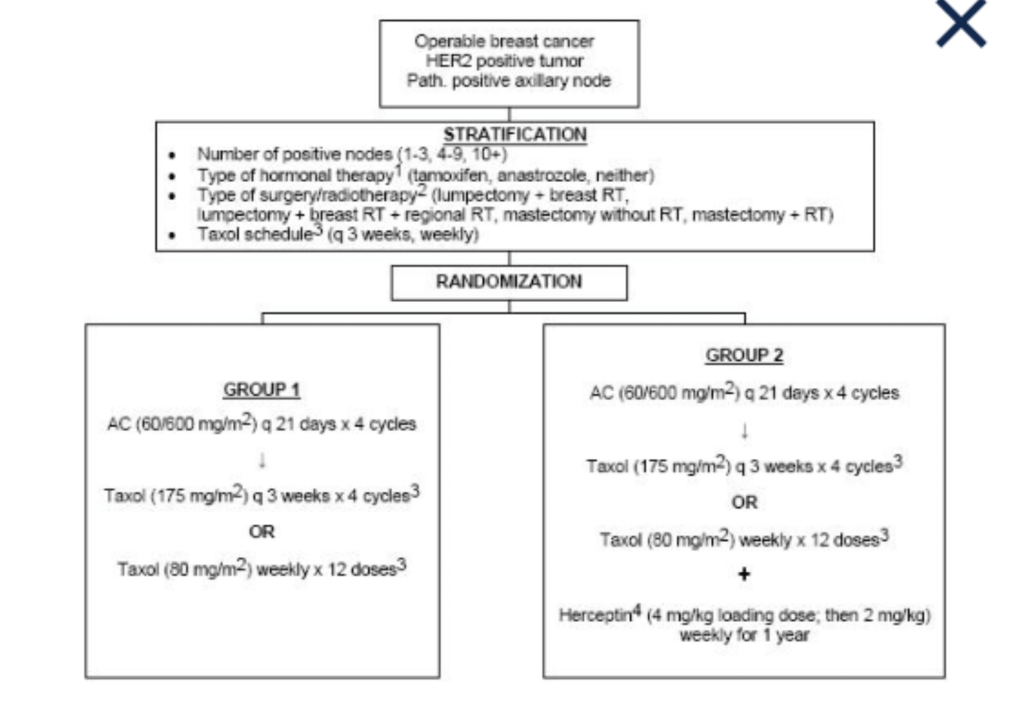
The NSABP B-31 trial compared:
Doxorubicin and cyclophosphamide followed by paclitaxelevery 3 weeks (group 1) with the same regimen plus 52 weeks of trastuzumab given concurrently with paclitaxel (group 2).
Trial Schema of NSABP B-31.
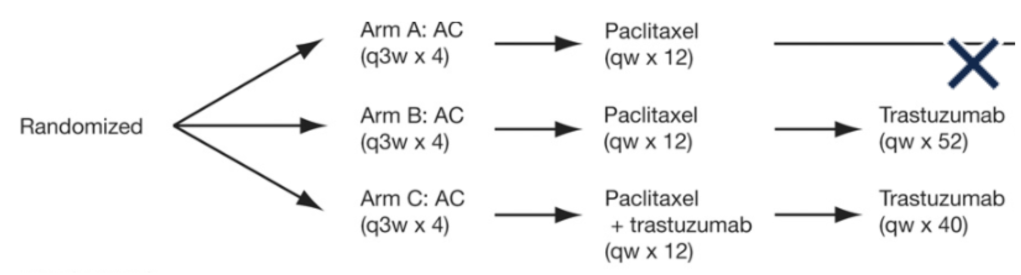
The North Central Cancer Treatment GroupNCCTG N9831 trial conducted a similar study that compared three regimens:
Group A:
Doxorubicin and cyclophosphamide followed by weekly paclitaxel
Group B:
Doxorubicin and cyclophosphamide followed by weekly paclitaxel, followed by 52 weeks of trastuzumab given after paclitaxel
Group C:
The same regimen in group A, followed by 52 weeks of trastuzumab initiated concurrentlywith paclitaxel
Trial Schema of NCCTG N9831.
The studies were combined to include a joint analysis:
Comparing groups 1 and group A (the control group) with groups 2 and group C (the trastuzumab group)
Group B was excluded
Results by 2005 reported 394 events (recurrence, second primary cancer, or death before recurrence):
Of these events, 133 were from the trastuzumab group and 261 were in the control group (hazard ratio, 0.48; P<0.0001)
At 3 years, the absolute difference in DFS between the trastuzumab group and the control group was:
12% and trastuzumab therapy was associated with a 33% reduction in the risk of death(P=0.015)
The interim analyses of these trials favored trastuzumab so strongly:
That the trials were stopped early and patients in the other arms were offered trastuzumab
Long-term analysis of these studies was reported in 2014:
At a median follow-up time of 8.4 years:
The addition of trastuzumab to chemotherapy led to a 37% improvement in OS and an increase in 10-year survival rate from 75.2% to 84%
Outcomes in DFS showed an improvement of 40% and an increase in the 10-year DFS rate from 62.2% to 73.7%
This study showed that all subgroups of HER2-positive patients (small and large tumors, hormone receptor-positive and -negative, low and high number of positive nodes, young and old patients):
Benefited from the addition of the targeted anti-HER2 agent, making trastuzumab an integral drug in the treatment of HER2-positive breast cancer
References
Perez EA, Romond EH, Suman VJ, Jeong J-H, Sledge G, Geyer Jr GE, et al. Trastuzumab plus adjuvant chemotherapy for human epidermal growth factor receptor 2-positive breast cancer: planned joint analysis of overall survival from NSABP B-31 and NCCTG N9831. J Clin Oncol. 2014;32(33):3744-3752.
Romond E, Perez E, Bryant J, Suman VJ, Geyer Jr GE, Davidson NE, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353(16):1673-1684.
Biochemical Testing: Perioperative Calcium And PTH
The ability to predict the occurrence of transient hypoPT:
By subjective surgeon assessment during operation:
Is highly variable
Objective serial measurement of serum calcium levels:
Has traditionally been used to stratify for risk of symptomatic hypocalcemia development during the postoperative period
And to determine the need for oral calcium and calcitriol administration
After thyroidectomy:
The absolute value of serum calcium levels
As well as the trend and slope or rate of change of these values:
Have also been employed to predict hypoPT:
But this approach requires sufficient time to observe such a trend
In one study:
Serum calcium levels were measured at 6 and 12 hours after total thyroidectomy
Patients with a positive serum calcium slope (rise in level):
Were deemed safe for hospital discharge with or without calcium supplementation
For patients with a non-positive slope but with serum calcium levels equal or greater than 8 mg/dL:
Discharge with calcium supplementation was also found to be safe
Because trending calcium often requires sampling over a 12- to 24-hour or longer time period, and because postoperative calcium levels may be confounded by prophylactic calcium and calcitriol administration or by low preoperative vitamin D levels:
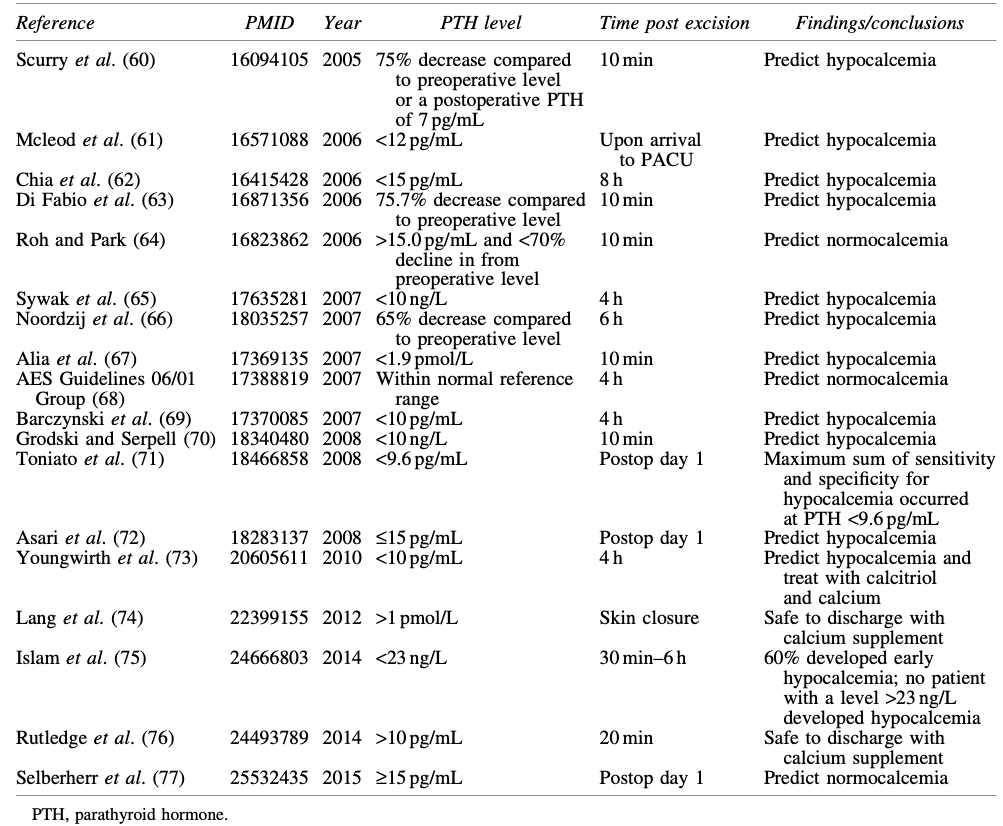
Many groups have examined the utility of measuring intraoperative or postoperative intact PTH levels drawn at various time points in the early post-thyroidectomy period (Table)
Studies of Post-Thyroidectomy Intact PTH Threshold Levels That Are Predictive of Normocalcemia or Hypocalcemia
Intraoperative PTH (IOPTH) refers to:
Rapid processing of blood specimens drawn during or shortly after thyroid or central neck surgery to determine PTH levels that will influence surgical or postoperative management
At many institutions, the IOPTH assay provides a rapid, actionable result:
Whereas the routine intact PTH assay may not have a turnaround time that is fast enough for perioperative decision making
It is the normal short half-life of PTH (3–5 minutes):
That enables decisions based on early postoperative PTH levels
The timing of PTH measurements in published studies has ranged from 10 minutes to 24 hours post thyroidectomy:
McLeod et al:
Found that a low recovery room drawn postoperative PTH level (< 12 pg/mL) predicted the development of hypocalcemia:
With a sensitivity of 100% and a specificity of 92%
Sywak et al:
Reported that a low four-hour postoperative PTH level (3 to 10 pg/mL) had a sensitivity of 90% and a specificity of 84% for predicting post-operative hypocalcemia
Asari et al:
Reported that an intact PTH level of less than 15 pg/mL on postoperative day 1 predicted hypoPT, with a sensitivity of 97.7% and a specificity of 82.6%
Thus, the earliest opportunity to predict hypoPT reliably is:
Through measurement of serum PTH level either at the conclusion of or immediately following surgery
A PTH level <15 pg/mL:
Is usually predictive of impending hypocalcemia
IOPTH levels measured alone or combined with serum calcium level measurements:
May guide the decision to:
Discharge versus monitor patients in the hospital setting
To prescribe prophylactic oral calcium
To take more aggressive measures to prevent or treat hypocalcemia
Based on the available evidence, and acknowledging that reference ranges differ based on assay and institution:
It is the opinion of the ATA Surgical Affairs Committee:
That a PTH value equal or greater than 15 pg/mL measured in adults at equal or greater than20 minutes following thyroidectomy:
Would obviate the need for intensive serum calcium monitoring and/or calcium supplementation
A postoperative PTH value of less than 15pg/mL:
Would suggest an increased risk for acute hypoPT that might prompt preemptive prescribing of oral calcium and calcitriol and/or serial serum calcium measurements until calcium stability has been confirmed
The ability to predict transient as opposed to permanent hypoPT following thyroidectomy is uncertain:
At least one study found that acute postoperative hypoPT specifically did not predict permanent hypoPT
Several parameters, including postoperative PTH values, decline in PTH values between preoperative and postoperative measurements, degree of decrease in magnesium levels, and whether PA was carried out:
Have been associated with the risk of permanent hypoPT:
However, the utilization of these parameters is not consistently established and requires further investigation
Graves’ disease is a common cause of hyperthyroidism that impacts quality of life
Treatment choices for Graves’ disease include:
Antithyroid drugs
Radioactive iodine (RAI)
Thyroidectomy
Patients are frequently treated with longterm anti-thyroid drugs or RAI:
With relief of biochemical hyperthyroidism as a common treatment end point
However, euthyroid patients with Graves’ disease:
May continue to have impaired quality of life
Validated tools that study patient-reported outcomes for benign thyroid disease identify general quality-of-life indicators and thyroid-specific symptoms
This study prospectively evaluated, at three intervals (preoperative, short-term postoperative, and long-term postoperative), patients with Graves’ disease undergoing thyroidectomy to assess differences in thyroid-specific symptoms, quality of life, and symptom burden over time
Clin Thyroidol 2022;34:17–19
Methods:
Adult patients who underwent total thyroidectomy for Graves’ disease between 2015 and 2020 were administered the MD Anderson Symptom Inventory (MDASI) survey:
A thyroid-specific patient-reported outcomes (PRO) survey, and a core symptom score to develop a composite Total Symptom Burden Score
Patient factors collected included age, race/ethnicity, sex, marital status, employment status, religion, and insurance status
Timing of survey data was defined as presurgery (< 120 days prior to surgery), short-term postsurgery (< 30 days), and long-term postsurgery (> 30 days)
In addition to measuring general quality-of-life indicators, the tool assesses common hyperthyroid patient symptoms, including hoarseness, heat and cold sensitivity, palpitations, dysphagia, and diarrhea
Results:
The 85 patients included in this study had:
A median age of 42 years
83.5% were female
Of these patients, 38.8% were obese (BMI >30)
Long-term postsurgery data were collected at a median of 205 days (range, 94–548 days) following thyroidectomy
Nearly all patients (95.3%) had started and were still taking an antithyroid drug
From the overall cohort, 63.5% of patients had a normal serum free thyroxine (FT4) level prior to surgery
The Thyroid Symptom Score improved significantly from before surgery to after, in both the short and the long term, with the most significant improvement realized between preoperative and short-term assessments
Specific thyroid symptoms that improved significantly after surgery included “feeling hot,” “racing heartbeat,” “diarrhea,” and “difficulty swallowing.”
The quality-of-life symptoms that significantly improved at short-term assessment included “general activity,” “mood,” “relationships with other people,” “walking,” “enjoyment of life,” and “work.”
The Total Symptom Burden Score improved significantly within 30 days after surgery
Conclusions:
In this cohort study of patients with Graves’ disease who underwent thyroidectomy, nearly all patients were treated initially with antithyroid drugs and 63.5% of the overall sample had normal serum FT4 levels before undergoing thyroid surgery
Patient-reported outcomes, including thyroid-specific symptoms and the Total Symptom Burden Score, improved significantly within 30 days of surgery
This study highlights important improvements in quality of life in patients with Graves’ disease who undergo thyroidectomy
The most significant improvement in symptoms was realized at short-term follow-up (<30 days):
Emphasizing the utility of thyroidectomy for treatment of Graves’ disease in patients who are seeking immediate remedy of symptoms
By contrast, a longitudinal study of the efficacy of Graves’ disease treatment in Sweden (with only 4.6% of participants treated with thyroidectomy) found that by 6 to 10 years posttreatment, over one quarter of patients reported that they had not fully recovered
Understanding the anticipated time course for treatment effects is critical to effective patient counseling
Nearly two thirds of patients in this study were euthyroid at the time of initial assessment
Although prior studies have recognized more pronounced impairments in quality of life in hyperthyroid Graves’ disease patients:
This research demonstrated that even patients who were euthyroid preoperatively experienced significant improvement in thyroid symptoms and quality of life
This finding argues for a nuanced approach to long-term management of patients with Graves’ disease beyond achieving a biochemically euthyroid state
Many patients with Graves’ disease request or self-refer for evaluation for thyroidectomy
Their thyroid-specific neck symptoms, including local symptoms of dysphagia, compression, perceived shortness of breath, and neck tightness, may be discounted, particularly if their hyperthyroidism is biochemically controlled
Recognizing the immediate and substantial symptom improvement after thyroidectomy should prompt consideration of thyroidectomy in initial, rather than last resort, Graves’ disease management, even in patients who are able to be rendered euthyroid with antithyroid drugs
Iatrogenic injury of the recurrent laryngeal nerve (RLN) is a serious complication during thyroid surgery
Reports from the literature show that the rates of RLN injury during thyroidectomy range from:
0.3 to 8%
Generally, the complication is unilateral and transient:
But it can be bilateral and / or permanent
Anatomic variations of the RLN:
Can potentially compromise the safety of the nerve during surgery
The current gold standard is:
Visualization of the RLN before beginning dissection of the thyroid:
But an anatomically intact nerve does not substantiate a functional nerve
In recent years, intraoperative neuromonitoring (IONM) and continuous intraoperative nerve monitoring (CONM):
Have been a useful adjunct in RLN identification and are helpful in assessing RLN electrophysiologic function during surgery
The objective of this study was to provide a global assessment of RLN anatomic variation and to identify potential correlations between RLN anatomy and electrophysiologic responses using IONM, with the aim of minimizing the rate of RLN injury during thyroidectomy
Clin Thyroidol 2022;34:35–37.
Methods:
This was a large multi-institutional prospective survey of patients undergoing thyroidectomy with or without central or lateral neck dissections following the standards set forth by International Neural Monitoring Study Group guidelines across 17 institutions on five continents between March 2015 and November 2017
A total of 1000 RLNs from 574 patients were assessed
All patients underwent preoperative and postoperative laryngoscopy
Individuals with postoperative vocal-cord paralysis and paresis (VCP) were followed using laryngoscopy for 12 months postoperatively
The International RLN Anatomic Classification System was used to assist in the classification of RLN anatomic variations
Patients with extensive lymph node metastases and cases with technical IONM failure or failure to visualize the RLN were excluded from the study
Results:
Nearly one-quarter (23%) of the RLNs:
Deviated from their anticipated anatomical course
30% of RLNs were fixed, splayed, or entrapped:
At the level of the capsule of the thyroid
Entrapment at the ligament of Berry was observed in 41% of nerves
Loss of signal during surgery was more likely when there was:
Abnormal nerve trajectory
Fixed, splayed or entrapped nerves
Cancer invasion
In cases that included lateral lymph node dissection
Although the right RLN had loss of signal more often than the left:
Laterality was not statistically significant (P = 0.12)
Using IONM loss of signal as a test of postoperative VCP:
The positive predictive value was 74.3%
The negative predictive value was 99.8%
Traction injury:
Was the most common cause of RLN injury (63%):
Especially at the site of the ligament of Berry
Conclusions:
Anatomical variations of the RLN could not be predicted preoperatively, but nearly one quarter of RLNs followed an abnormal trajectory
Anatomical variations were associated with higher rates of RLN injury
The use of IONM was a helpful risk-minimization tool
Traction was the most common cause of injury, and although most VCP resolved within 1 year, the recovery rate was less than previously reported
Intraoperative verification of functional and anatomical RLN integrity:
Is needed for safe thyroid surgery
Furthermore, there is significant value in identifying anatomical RLN variants and possible risk factors in order to maximize preservation of nerve function
This study sought to further understand anatomical RLN variants and to intraoperatively assess nerve injury and electrophysiologic responses using IONM during thyroid surgery
Even though there are several studies in the literature that assessed anatomic RLN variation, there are very few with such a large and diverse sample size that prospectively investigated anatomical data
This study supports findings from other studies, including traction injuries as a common cause of vocal-cord paralysis
This work is an important addition to the literature:
Not only is it a large multicenter international study, but it also included intraoperative electrophysiologic responses using IONM and longterm follow-up to assess functional outcomes of VCP
As surgeons, we often are limited by individual or institutional experience and are not always able to pinpoint the root cause of inadvertent nerve injury
Such a broad study more comprehensively illustrates the startling diversity of anatomic RLN variants
This heterogeneity is perhaps not surprising given the anatomic variation observed in other major nerves, such as the facial nerve in parotidectomy or the nerve to the vastus lateralis in microvascular surgery
The rates of variation, loss of signal, and eventual recovery can help surgeons better inform patients about the underlying risks of an operation
The study is particularly noteworthy in its assessment of the RLN position at the ligament of Berry, reporting rates at which the nerve is fixed, splayed, or entrapped
This area is of high interest to surgeons, who must balance nerve preservation, nerve traction, and safe removal of the maximal amount of thyroid tissue
Paradoxically, cancer is not often found at this junction, yet leaving too much thyroid issue behind may lead to higher levels of thyroglobulin and the potential need for radioactive iodine
The study’s findings will likely increase focus on the variation observed and better enlighten surgeons about their approach to this sensitive area
A Protocol for the Evaluation of Radical Mastectomy and Total Mastectomy with and without Radiation in the Primary Treatment of Cancer of the Female Breast
Enrolled 1,079 patients:
With clinically node-negative disease
Randomized patients to:
Radical mastectomy (RM)
Total mastectomy (TM) plus local-regional axillary irradiation, or
TM alone
An additional 586 patients:
With clinically node-positive disease
Were randomized to:
RM or
TM plus radiation
An important point of this trial:
Is that none of these patients received systemic therapy
After 25 years of follow-up:
The study showed no significant difference in long-term outcome:
Between clinically node-negative patients:
Who received RM and those who received TM with or without radiation
Between clinically node-positive patients:
Who received RM vs.TM with nodal irradiation
When comparing the hazard ratio for death within the two arms:
The results show no survival advantage from RM
In patients with clinically node-negative disease:
Pathologic examination of the mastectomy specimen in patients treated with radical mastectomy:
Revealed that 40% of the patients had pathologically positive nodes
However, only 19% of patients treated with TM alone and no axillary surgeryhad an axillary recurrence:
Suggesting that not all occult axillary disease will progress into clinically meaningful disease:
Even in the absence of systemic therapy
NSABP B-06:
Phase III Total Mastectomy / Axillary Dissection vs Segmental Mastectomy / Axillary Dissection with or without Radiotherapy for Potentially Curable Breast Carcinoma
Compared lumpectomy and axillary node dissectionwith or without breast irradiation with modified radical mastectomy (MRM):
In patients with tumors 4 cm or less in greatest diameter
The results of this trial:
Demonstrating equivalent survival between the two surgical options:
Establish BCS as a viable surgical option for most patients with invasive breast cancer
The Milan I trial:
Compared 701 patients with invasive breast cancer up to 2 cm in size without clinically positive axillary lymph nodes
Randomized them into those who:
Received radical mastectomy and those who received quadrantectomy plus axillary dissection and radiotherapy
A recent analysis of the trial:
Showed no differences in OS between the two study groups
The NSABP B-17:
Phase III Randomized Study of Postoperative Radiotherapy Following Segmental Mastectomy and Axillary Dissection in Patients with Noninvasive Intraductal Adenocarcinoma of the Breast:
Compared lumpectomy alone to lumpectomy plus breast irradiation:
In 818 patients with localized ductal carcinoma in situ
This trial concluded that:
Radiotherapy did not improve OS but that it did significantly decrease the rate of invasive or in situ in breast tumor recurrence in the ipsilateral breast
The EORTC Trial 10801:
Was a randomized multicenter trial:
That compared breast-conserving therapy with MRM for patients with invasive breast cancer less than 5 cm in diameter
At 10 years:
There was no difference between the two groups in:
OS or in distant metastasis-free rates
Locoregional recurrence at 10 years was:
12% for the mastectomy group and 20% for the breast-conserving therapy group
References:
Fisher B, Montague E, Redmond C, Barton B, Borland D, Fisher ER, et al. Comparison of radical mastectomy with alternative treatments for primary breast cancer: a first report of results from a prospective randomized clinical trial. Cancer. 1977;39(6 Suppl):2827-2839.
Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347(16):1233-1241.
Mamounas EP, Wickerham DL, Fisher B, Geyer CE, Julian TB, Wolmark N. The NSABP experience. In: Kuerer HM, ed. Kuerer’s Breast Surgical Oncology. New York, NY: McGraw-Hill Companies; 2010:475-508.
Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347(16):1227-1232.
Fisher B, Dignam J, Wolmark N, Mamounas E, Costantino J, Poller W, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998;16(2):441-452.
Curran D, van Dongen JP, Aaronson NK, Kiebert G, Fentiman IS, Mignolet F, et al. Quality of life of early-stage breast cancer patients treated with radical mastectomy or breast-conserving procedures: results of EORTC Trial 10801. The European Organization for Research and Treatment of Cancer (EORTC), Breast Cancer Co-operative Group (BCCG
Andtbacka RH, Babiera G, Singletary SE, Hunt KK, Meric-Bernstam F, Feig BW, et al. Incidence and prevention of venous thromboembolism in patients undergoing breast cancer surgery and treated according to clinical pathways. Ann Surg. 2006;243(1):96-101.
El-Tamer MB, Ward BM, Schifftner T, Neumayer L, Khuri S, Henderson W. Morbidity and mortality following breast cancer surgery in women: national benchmarks for standards of care. Ann Surg. 2007;245(5):665-671.
Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuünemann HJ; American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl);7S-47S.
Neumayer L, Schifftner TL, Henderson WG, Khuri SF, El-Tamer M. Breast cancer surgery in Veterans Affairs and selected university medical centers: results of the patient safety in surgery study. J Am Coll Surg. 2007;204(6):1235-1241.