- Biochemical Testing: Perioperative Calcium And PTH
- The ability to predict the occurrence of transient hypoPT:
- By subjective surgeon assessment during operation:
- Is highly variable
- By subjective surgeon assessment during operation:
- Objective serial measurement of serum calcium levels:
- Has traditionally been used to stratify for risk of symptomatic hypocalcemia development during the postoperative period
- And to determine the need for oral calcium and calcitriol administration
- After thyroidectomy:
- The absolute value of serum calcium levels
- As well as the trend and slope or rate of change of these values:
- Have also been employed to predict hypoPT:
- But this approach requires sufficient time to observe such a trend
- Have also been employed to predict hypoPT:
- In one study:
- Serum calcium levels were measured at 6 and 12 hours after total thyroidectomy
- Patients with a positive serum calcium slope (rise in level):
- Were deemed safe for hospital discharge with or without calcium supplementation
- For patients with a non-positive slope but with serum calcium levels equal or greater than 8 mg/dL:
- Discharge with calcium supplementation was also found to be safe
- Because trending calcium often requires sampling over a 12- to 24-hour or longer time period, and because postoperative calcium levels may be confounded by prophylactic calcium and calcitriol administration or by low preoperative vitamin D levels:
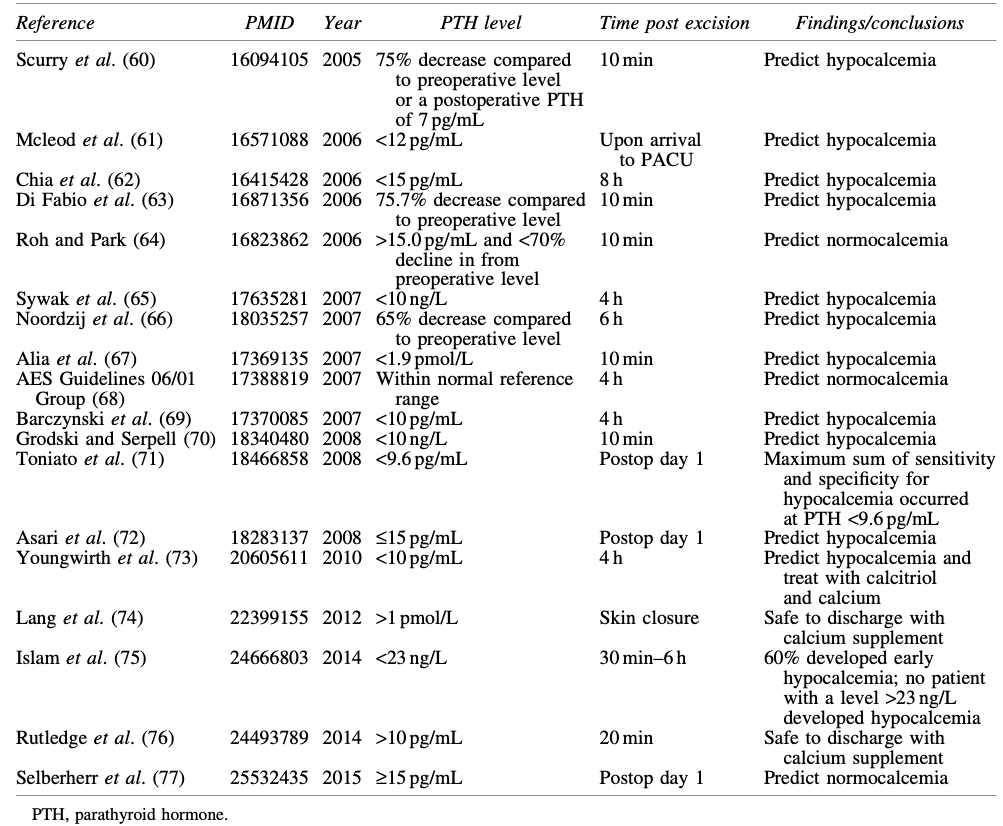
- Many groups have examined the utility of measuring intraoperative or postoperative intact PTH levels drawn at various time points in the early post-thyroidectomy period (Table)
- The ability to predict the occurrence of transient hypoPT:
- Intraoperative PTH (IOPTH) refers to:
- Rapid processing of blood specimens drawn during or shortly after thyroid or central neck surgery to determine PTH levels that will influence surgical or postoperative management
- At many institutions, the IOPTH assay provides a rapid, actionable result:
- Whereas the routine intact PTH assay may not have a turnaround time that is fast enough for perioperative decision making
- It is the normal short half-life of PTH (3–5 minutes):
- That enables decisions based on early postoperative PTH levels
- The timing of PTH measurements in published studies has ranged from 10 minutes to 24 hours post thyroidectomy:
- McLeod et al:
- Found that a low recovery room drawn postoperative PTH level (< 12 pg/mL) predicted the development of hypocalcemia:
- With a sensitivity of 100% and a specificity of 92%
- Found that a low recovery room drawn postoperative PTH level (< 12 pg/mL) predicted the development of hypocalcemia:
- Sywak et al:
- Reported that a low four-hour postoperative PTH level (3 to 10 pg/mL) had a sensitivity of 90% and a specificity of 84% for predicting post-operative hypocalcemia
- Asari et al:
- Reported that an intact PTH level of less than 15 pg/mL on postoperative day 1 predicted hypoPT, with a sensitivity of 97.7% and a specificity of 82.6%
- McLeod et al:
- Thus, the earliest opportunity to predict hypoPT reliably is:
- Through measurement of serum PTH level either at the conclusion of or immediately following surgery
- A PTH level < 15 pg/mL:
- Is usually predictive of impending hypocalcemia
- IOPTH levels measured alone or combined with serum calcium level measurements:
- May guide the decision to:
- Discharge versus monitor patients in the hospital setting
- To prescribe prophylactic oral calcium
- To take more aggressive measures to prevent or treat hypocalcemia
- May guide the decision to:
- Based on the available evidence, and acknowledging that reference ranges differ based on assay and institution:
- It is the opinion of the ATA Surgical Affairs Committee:
- That a PTH value equal or greater than 15 pg/mL measured in adults at equal or greater than 20 minutes following thyroidectomy:
- Would obviate the need for intensive serum calcium monitoring and/or calcium supplementation
- That a PTH value equal or greater than 15 pg/mL measured in adults at equal or greater than 20 minutes following thyroidectomy:
- It is the opinion of the ATA Surgical Affairs Committee:
- A postoperative PTH value of less than 15 pg/mL:
- Would suggest an increased risk for acute hypoPT that might prompt preemptive prescribing of oral calcium and calcitriol and/or serial serum calcium measurements until calcium stability has been confirmed
- The ability to predict transient as opposed to permanent hypoPT following thyroidectomy is uncertain:
- At least one study found that acute postoperative hypoPT specifically did not predict permanent hypoPT
- Several parameters, including postoperative PTH values, decline in PTH values between preoperative and postoperative measurements, degree of decrease in magnesium levels, and whether PA was carried out:
- Have been associated with the risk of permanent hypoPT:
- However, the utilization of these parameters is not consistently established and requires further investigation
- Have been associated with the risk of permanent hypoPT:
#Arrangoiz #ThyroidSurgeon #ParathyroidSurgeon #Hypoparathyroidism #HeadandNeckSurgeon #CancerSurgeon
