My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
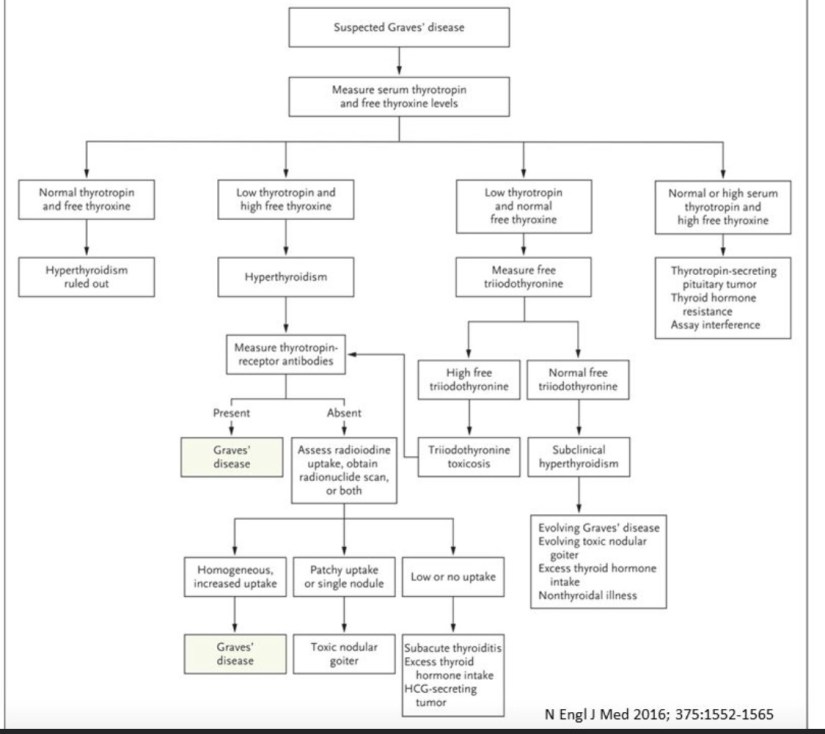
In the absence of extra-thyroidal symptoms or diffuse goiter, measurement of thyrotropin-receptor antibodies is performed and has a sensitivity and specificity of over 99%
Several studies have reported that microscopic extrathyroidal extension (m-ETE) does not increase disease-related mortality in patients with papillary thyroid cancer (PTC); however, the literature is scarce with regard to the impact of macroscopic (gross) extrathyroidal extension invading only strap muscles (T3b-ETE) on outcomes that are important to patients
This study was performed to evaluate the association between T3b-ETE tumors and disease-specific survival (DSS) in patients with PTC
Methods:
This hospital-based single-institution study included adults who underwent initial surgery for PTC, with or without local or distant metastasis, between 1986 and 2015
The cohort was classified into three groups:
Mo macro-ETE:
No gross intra-operative evidence of extrathyroidal extension
T3b-ETE:
Gross intraoperative evidence of extra-thyroidal extension invading only strap muscles
A Cox proportional-hazards model was used to investigate the association of ETE categories and 10-year disease-specific survival (DSS, defined as the interval between initial surgery and last appointment or death with evidence of local or distant disease)
This model was adjusted for pathologic nodal stage, distant metastasis stage, and age
A subgroup analysis by age (< 55 vs. ≥ 55 years) was planned
Results:
A total of 5880 patients with a median follow-up of 64 months were included
Most were female (72.2%), were < 55 years of age (68.2%); had a tumor size between 0 and 4 cm (94.6%); were classified as T1 (71.3%), N0/Nx (68.1%), and M0 (98.9%); had ATA intermediate-risk disease (37.6%); and had AJCC stage I disease (89.4%)
Overall, 5485 patients had macro-ETE (93.3%), 179 had T3b-ETE (3.0%), and 216 had T4-ETE (3.7%)
In the overall adjusted multivariate analysis and compared with the no macro-ETE group, the T3b-ETE group had a similar risk of DSS (HR, 2.11; 95% CI, 0.72–6.15) and the T4-ETE group had a higher risk of DSS (HR, 5.22; 95% CI, 2.90–9.40)
In the subgroup analysis, patients ≥ 55 years of age with T3b-ETE had a higher risk of DSS as compared with patients with no macro-ETE (HR, 3.29; 95% CI, 1.07–10.08), similar to the higher risk also seen in the T4-ETE group (HR, 9.39; 95% CI, 4.68–18.81)
There were 26 patients with residual disease after initial surgery (none from the T3b-ETE group), and there were only 60 DSS events
Conclusions:
Macroscopic extrathyroidal extension invading only the strap muscles (T3b-ETE) increases disease-specific death in patients with PTC who are ≥55 years of age,as compared with patients with no macro-ET
This retrospective study found no increased disease-specific mortality in patients with T3b-ETE overall and increased disease-specific mortality only in those ≥55 years
The strength of the Harries et al. study is the meticulous record review and histologic confirmation of the intraoperative T3b-ETE findings
Nevertheless, the small number of DDS events limited the analysis of other prognostic factors in the multivariate model, including the tumor size and impact of postoperative radioactive iodine ablation
The literature about the impact of extrathyroidal extension (ETE) on disease outcomes provides inconsistent conclusions
Factors contributing to different findings are the lack of a standard definition and reporting of ETE
For instance, some studies defined ETE and its severity by the direction of invasion (perithyroid tissue, strap muscle, and beyond strap muscle), while others defined ETE based on pathology reports and operative findings
Therefore, it is expected that different definitions of the disease may lead to different outcomes and conclusions
Macroscopic ETE is defined as an operative or gross examination finding noted when cancer extends out of the thyroid into adjacent structures
In contrast, microscopic ETE is defined as when the tumor invasion is observed under a microscope
It is expected that all macroscopic ETE will have evidence of microscopic ETE
These definitions imply that clinicians taking care of patients with thyroid cancer should carefully review the pathological report and the operative report to classify ETE correctly
We have also found that frequent communication with our surgical colleagues can help clarify the operative and histopathologic findings
Future studies using standardized definitions will elucidate the impact of macroscopic disease on recurrence and mortality in PTC
In the meantime, we agree with the authors of this study that it is prudent to consider T3b-ETE as a prognostic adverse risk factor between microscopic ETE and macroscopic ETE with invasion into adjacent tissues
The incidence of papillary thyroid cancer (PTC) is increasing at a rapid rate:
Probably related to thyroid nodules being detected incidentally by more frequent radiologic studies being performed, and
Also likely due to a change in the molecular oncogenes:
Driving its development and progression
The standard initial treatments include:
Thyroidectomy and, in some instances, radioactive iodine therapy
The factors that assist in the decision for a particular treatment are multiple, but include:
Patient age
Gender
Histologic characteristics
Findings on radiologic and nuclear medicine studies
Postoperative serum thyroglobulin levels
One particular histologic finding:
Minor extra-thyroidal invasion:
Has been controversial regarding its relevance to recurrence and prognosis
Diker-Cohen et al performed a meta-analysis and noted that:
Minimal extrathyroidal extension:
Did increase the risk of recurrence, but not of mortality
Castagna et al also reported:
An increased risk of recurrence in patients with minimal extrathyroidal extension when compared to intrathyroidal tumors
In contrast, Ahmaddy et al and Raruenrom et al:
Did not find that minimal extrathyroidal extension was associated with a worse prognosis
In the current study, Forleo et al have investigated this issue, adding further understanding to the interpretation of minimal extrathyroidal invasion in patients with PTC
Methods:
The authors used the Italian Thyroid Cancer Observatory database to identify patients with PTC with minimal extrathyroidal extension and excluded patients who had local lymph node involvement with cancer
This database includes patient information prospectively collected from multiple medical centers
The authors identified 2,237 patients who fulfilled the study eligibility criteria and had at least 1 year of follow up
Multiple factors were evaluated, including the type of initial thyroid surgery, histologic variants of PTC, tumor diameter, risk stratification using the American Thyroid Association system, use and dose of radioactive iodine therapy and disease response
Results:
There were 1831 patients (81.8%) who had an excellent response, 296 (13.2%) an indeterminate response, 55 (2.5%) a biochemically incomplete response, and 55 (2.5%) a structurally incomplete response
Detailed evaluation indicate that, as individual factors:
Minimal extrathyroidal extension, tumor size larger than 2 cm,aggressive PTC histology, and age at diagnosis:
Were not found to be associated with a worse initial therapy response:
However, the combination of:
Minimal extrathyroidal extension and tumor size greater than 2 cm:
Was associated with a significantly worse outcome
Radioactive iodine therapy did not appear to improve prognosis
Conclusions:
Minimal extrathyroidal extension alone did not predict a worse prognosis in PTC patients who did not have cervical lymph node involvement in a large study cohort
However, it appears that the combination of tumor diameter larger than 2 cm and the presence of minimal extrathyroidal extension:
May help predict low-to-intermediate risk of recurrent or persistent disease
This study by Forleo et al helps further our understanding of the possible role of minimal extrathyroidal extension in PTC in predicting recurrent or persistent disease
The study has the attributes of analyzing a large group of patients, obtaining data from multiple medical centers at the time of initial surgery, of examining patients with no known cervical lymphadenopathy, and they used the ATA risk stratification system
However, there are also several aspects that should also be noted
There were multiple surgeons and pathologists, and there was not an independent pathologic review board that analyzed all of the samples
The study analyzed only the response at 1 year, but is apparently monitoring these patients over a longer duration
The definition of minimal extrathyroidal extension and its application in every case is not substantiated
In summary, I think it clinically relevant that this analysis of a large cohort of PTC patients found that minimal extrathyroidal extension alone is not a significant risk factor for recurrence, but when it is combined with tumor size > 2 cm, there appears to be a higher risk of recurrence
Radioactive iodine therapy did not seem to be beneficial, although there was a relatively low percentage of patients who received radioactive iodine and the statistical evaluation of this treatment was complex
I think it reasonable to consider all relevant laboratory, histology, radiologic and clinical factors on an individual basis to help decide whether radioactive iodine therapy may be warranted
In addition, performing a radioactive iodine scan with baseline and stimulated serum thyroglobulin levels may help in making this decision
References
Diker-Cohen T, Hirsch D, Shimon I, Bachar G, Akirov A, Duskin-Bitan H, Robenshtok E 2018 Impact of minimal extra-thyroid extension in differentiated thyroid cancer: systematic review and meta-analysis. J Clin Endocrinol Metab 103:2100–2106.
Castagna MG, Forleo R, Maino F, Fralassi N, Barbato F, Palmitesta P, Pilli T, Capezzone M, Brilli L, Ciuoli C, Cantara S, Formichi C, Pacini F 2018 Small papillary thyroid carcinoma with minimal extrathyroidal extension should be managed as ATA low-risk tumor. J Endocrinol Invest 41:1029–1035.
Graves’ disease (GD) is an autoimmune thyroid disorder that is the leading cause of hyperthyroidism
Understanding whether GD predisposes patients to thyroid cancer has been of interest for a long time
Previous research on the link between GD and the risk of concurrent thyroid cancer was based mostly on surgically treated GD patients, and the results were inconsistent
Furthermore, there are still controversies about the impact of GD on the clinical features and outcomes of thyroid cancer
Therefore, in the current study, Yoon and colleagues aimed to investigate the overall prevalence of thyroid cancer in patients with GD, as well as the clinicopathologic characteristics, prognosis, and predictive factors of its development
Methods:
This retrospective multicenter study collected data on all patients with GD treated at three tertiary referral hospitals in South Korea between January 2010 and December 2019
During their follow-up for GD, all participants in the study underwent at least one high-resolution neck ultrasound
All included patients were followed-up for at least one year
Demographic information, status of GD, antithyroid medications for the treatment of GD, as well as clinicopathologic characteristics, surgical and postoperative management, and prevalence and clinical outcomes of concomitant thyroid cancer in patients with GD were described
In the subgroup analysis, patients were divided into nodular GD and non-nodular GD groups based on the presence of thyroid nodules other than the primary thyroid cancer lesion(s)
Clinicopathologic features and thyroid cancer prognosis were compared between the two subgroups
Using binary logistic-regression analysis, risk factors for thyroid cancer recurrence / persistence were further investigated
Results:
The current study was composed of 15,159 patients with GD, including 262 (1.7%) with coexisting thyroid cancer
The majority of the patients (251 [95.8%]) had undergone cytologic assessment of thyroid tissue prior to surgery, while the remaining patients (11 [4.2%]) were diagnosed with occult thyroid cancer after thyroid surgery was performed for other indications, such as compression symptoms caused by a large goiter and / or uncontrolled hyperthyroidism
In 245 (93.5%) and 17 (6.5%) of the patients, total thyroidectomy and lobectomy, respectively, were performed
Micro–thyroid carcinomas were found in 182 GD patients (69.5%), which was comparable to the proportion of those in without GD (19,397 of 30,231 [64.2%])
The mean (±SD) age of patients with GD and coexisting thyroid cancer was 55.1±13.9 years
Active GD, defined as newly diagnosed GD or the use of anti-thyroid drugs, was found in 229 patients (87.4%)
Papillary thyroid cancer (PTC) accounted for nearly all (260 [99.2%]) of the histologic thyroid cancer subtypes
Extrathyroidal extension and lymph node metastases were identified in 65 (24.8%) and 89 (34.0%) of the patients, respectively
None of the patients had distant metastases
In 113 (43.1%) of the patients, radioiodine ablation was administered after surgery
There was no evidence of thyroid cancer in 242 (92.4%) of patients at a median follow-up of 59.1 months, while 20 (7.6%) had recurrent / persistent thyroid cancer
In the subgroup analysis, thyroid cancer patients with nodular GD were older (61.9±12.8 vs. 52.1±13.3 years, P = 0.001) and more were female (86.3% vs. 75.3%, P = 0.046) than those with non-nodular GD
There was no difference in thyroid cancer aggressiveness, according to preoperative cytologic and ultrasonographic assessments, between the groups
However, there was a substantial difference in the non-classic PTC subtypes between the two groups: patients in the nodular GD group had only follicular variant PTC,whereas the non-nodular GD group had seven patients with non–follicular variant, non-classic PTC subtypes
Although thyroid cancer recurrence was detected only in patients with non-nodular GD, the difference was not considered to be significant
Furthermore, multivariate analysis revealed that only lymph node metastasis (odd ratio, 4.359; 95% confidential interval, 1.267–14.944; P = 0.020) was independently associated with recurrent / persistent thyroid cancer
Conclusions:
This multicenter retrospective study of GD patients, including those without surgical intervention for GD, showed that the proportion of coexisting thyroid cancer was substantially lower than previously reported
The small proportion of thyroid cancer patients with concomitant GD had a generally favorable prognosis for their thyroid cancer, but those with lymph node metastases may need to be monitored more closely
The possible association between thyroid cancer and autoimmune thyroid diseases, mainly GD and Hashimoto’s thyroiditis (HT):
Has been of considerable interest for a long time
Although an underlying autoimmune pathology exists in both conditions, HT features chronic inflammatory infiltration in the thyroid gland, whereas GD involves the critical presence of thyroid stimulating antibody (TSAb)
As growing evidence suggests that there is an increased risk of thyroid cancer in patients with HT, interest has also focused on the role of GD in the development and prognosis of thyroid cancer
However, data from available studies have provided conflicting information
A large-scale cohort study conducted in Taiwan has suggested a higher risk of thyroid cancer in GD patients:
In 5025 newly diagnosed GD patients, 52 thyroid cancer events were identified (1.0%), as compared with 20 events recorded in 20,100 non-GD subjects (0.1%)
However, there was little information on how these thyroid cancers were diagnosed
Given that patients with GD are more likely to undergo thyroid examination, including ultrasonography, than those without GD, we should not easily attribute a possible increased prevalence of thyroid cancers to GD per se, but rather to the attentive surveillance of the thyroid provided to GD patients
The current study was based on all ultrasound-screened GD patients, including nonsurgically treated patients, in contrast to many previous studies in which only surgery-treated patients were included
Hence, this study avoided selection bias generated from indications toward surgical management
The rate of coexisting thyroid cancer in GD patients was higher than that in the above-mentioned Taiwan cohort (1.7% vs. 1.0%, P<0.001).;
Again, this suggests that routinely performing ultrasound screening leads to more cancer cases being found
Although the authors could not directly compare the prevalence of thyroid cancer between GD patients and non-GD patients in their study, another population-based study performed at Health Promotion Center of Asan Medical Center, South Korea, provides some insight:
In 15,000 subjects who were ultrasound-screened and underwent fine-needle aspiration of suspicious thyroid nodules, 267 patients (1.8%) were identified with a coexisting thyroid cancer
Here, we notice that once ultrasound screening is uniformly applied on the population level, the prevalence of thyroid cancer in the general population and in GD patients is comparable
Taken together, these studies suggest that GD may not increase the risk for thyroid cancer
To avoid overdiagnosis of thyroid cancer, universal screening for thyroid cancer among GD patients should not be encouraged
The current study also reported favorable thyroid cancer outcomes in patients with coexisting GD and thyroid cancer, although a comparison could not be made directly with non-GD patients
There remain some questions to be answered;
First, in vitro studies have linked TSAb to mitogenic, antiapoptotic and angiogenic effects probably mediated through its binding to the TSH receptor and stimulation of various signaling pathways:
Would changing TSAb status over time (e.g., persistently high titers vs. rapidly declining titers) impact the clinical features and prognosis of thyroid cancer in GD patients differently?
Second, nearly 70% of the thyroid cancer patients found in this cohort had papillary microcarcinomas (<1 cm), which is the most indolent type of thyroid cancer:
Is it possible that the effects of GD on thyroid cancer outcomes might be more pronounced in more clinically relevant cases (i.e., larger or more aggressive thyroid cancers)?
This hypothesis is supported by a multicenter study in Italy, which indicated that GD was associated with a worse outcome of coexisting thyroid cancer only if the cancer was larger than 1 cm
Third, for patients with GD who have surgical indications, current American Thyroid Association guidelines recommend near-total or total thyroidectomy:
However, for GD patients whose thyroid function and TSAb titers are well controlled by antithyroid drugs, yet elect to have their coexisting low-risk PTC resected, what would be the optimal procedure to avoid overtreatment of these two diagnoses?
These important questions await further investigation
In the period immediately following thyroidectomy for differentiated thyroid cancer, there is a need to determine the extent of persistent disease and the likelihood of cancer recurrence
Predicting the mortality from thyroid cancer is performed using the AJCC/UICC TNM system
In order to assess the risk for disease persistence and recurrence, the American Thyroid Association (ATA) guidelines for differentiated thyroid cancer use a variety of indicators that are determined primarily from the surgical pathology
In the initial postoperative assessment, the ATA guidelines state that postoperative thyroglobulin (Tg) values suggestive of distant metastases are considered high risk, though the levels that are useful to guide risk determination are not entirely clear
The current study is a single-center, retrospective analysis aimed at determining the prognostic significance of pre-ablation stimulated Tg (ps-Tg) levels on prediction of disease persistence / recurrence and its use as a component of the ATA risk-stratification system
Methods:
Electronic records were collected from 2006 to 2018 at a tertiary care center in China
Patients were included in this analysis if they had undergone total thyroidectomy with postoperative radioactive iodine (RAI) ablation therapy and if their surgical pathology results were available
All patients were prepared for RAI using thyroid hormone withdrawal
Serum thyroid stimulating hormone (TSH), Tg, and thyroglobulin antibody (TgAb) levels were determined immediately prior to RAI administration
Patients with TgAb levels greater than 40 IU/ml were excluded
Patients were followed for an average of 5 years
The initial interaction was 6 to 12 months following RAI therapy
Patients with an excellent response to initial therapy (defined using criteria from the 2015 ATA differentiated thyroid cancer guidelines) were seen annually and followed with Tg measurements while taking levothyroxine (LT4) and with neck ultrasonography
Additional imaging studies were used if Tg levels were > 1 ng/ml
Anything other than an excellent response to initial therapy was counted as disease persistence
A receiver operating characteristic (ROC) curve was used to determine the most sensitive and specific levels of ps-Tg that predicted persistent/recurrent disease versus long-term remission
Results:
Of the 2524 patients included in this analysis, over 26% were classified as high risk for recurrence by ATA criteria, indicating a cohort that included many patients with advanced disease
Of the 2524 patients, 69% were women and over 96% had classic variant papillary thyroid cancer (PTC)
The average primary tumor size was 1.4 cm, and 85% of patients had documented lymph node metastases
Approximately 85% of patients had an excellent response and 15% had persistent or recurrent disease at the end of the study
The median ps-Tg level was 2.42 ng/ml (1.87 for those with excellent response and 35.66 for those with persistent/recurrent disease). Based on ROC analysis, a ps-Tg level of 10.1 ng/ml correlated with a sensitivity of 76% and a specificity of 88%, yielding a positive predictive value (PPV) of 53% and a negative predictive value (NPV) of 95%. This NPV remained >90% in all ATA risk categories.When analyzed by ATA risk categories, a ps-Tg cutoff of 10.1 ng/ml was predictive of outcomes. When below this cutoff, the risk of persistent disease decreased from 9.9% to 4.1% in intermediate-risk patients and from 33.1% to 8.5% in high-risk patients. Similarly, a value above the cutoff significantly increased the risk of persistent/recurrent disease even in low-risk patients (3.5–26.7%). The risk increased in high-risk patients, from 33.1% to 69.5%.ConclusionsIn this retrospective institutional analysis, a single preablation stimulated Tg cutoff level of 10.1 ng/ml significantly improved the prediction of disease recurrence/persistence in differentiated thyroid cancer. The use of this cutoff significantly enhanced prediction when incorporated into the 2015 ATA risk stratification model for differentiated thyroid cancer.COMMENTARYAssessing the likelihood of disease persistence and recurrence is extremely important to patients and providers after a diagnosis of cancer. Notwithstand-ing a recent cancer diagnosis, there is a significant amount of anxiety for patients receiving RAI, as many of those selected to receive it typically have lymph node involvement or larger tumor sizes.Disease predictors lack predictive power in the immediate postoperative assessment of intermedi-ate- and high-risk scenarios based on the surgical pathology alone. Several studies have reported that delayed evaluation (i.e., up to a year following RAI ablation) utilizing biomarkers and neck ultrasonog-raphy have better prognostic capabilities (3-5). For a patient, waiting this long can be nerve-wracking. A test to improve the ability to predict recurrence earlier in the postoperative period is desirable.Often, we measure stimulated Tg prior to giving RAI, though there is no clear guidance as to the value above which higher risk for disease persistence is indicated. Moreover, where does this information fit in regard to what is already estimated based on the risk stratification from the 2015 ATA guide-lines? This study was based on a large sample size and used ROC curve analysis to identify 10.1 ng/ml as a preablation Tg level with an NPV of >90%. This study adds to the literature identifying a preablation stimulated Tg <10 ng/ml as a predictor of excellent response to initial treatment (i.e., surgery and RAI ablation) in intermediate- to high-risk patients (6). This is helpful, as prior studies have investigated lower-risk patients or used various Tg cutoff values (7-9). Additionally, the authors determined that the use of preablation Tg values helped to “refine” recurrence estimates within risk categories. Inter-THYROID CANCER Preablation Stimulated Thyroglobulin as a A l e x Te s s n owPredictor of Persistent/Recurrent Differentiated Thyroid Cancer
Thyroid nodules and thyroid cancer are common clinical problems
The primary initial treatment of thyroid cancer is surgery:
Either thyroid lobectomy or total thyroidectomy
Experts have debated the extent of thyroid surgery and its impact on patient outcomes for many years
The 2015 ATA guidelines:
Endorsed thyroid lobectomy for low-risk differentiated thyroid cancers (DTCs):
Measuring 1 to 4 cm without extra-thyroidal extension (ETE) and clinical lymph node metastasis, in the absence of a family history of thyroid cancer and a personal history of radiation exposure to the head and neck
Subsequent literature has suggested that there has been a significant shift away from more extensive thyroid surgeries:
In managing benign and malignant thyroid disease
One study showed that the use of thyroid lobectomy in patients with thyroid cancer:
Increased from 17% in 2015 to 28% by the end of 2018
The current study was performed to further understand this surgical trend in patients with low-risk DTCs
Methods:
This was a retrospective study of patients with well-differentiated thyroid cancer who underwent thyroid surgery at Memorial Sloan Kettering Cancer Center between 1986 and 2015
Patients were staged according to the American Joint Committee on Cancer 8th edition and classified as being at low, intermediate, or high risk for recurrence according to the 2015 ATA guidelines
The 2015 ATA dynamic risk-stratification system was used to assess the initial response to therapy within the first year
Patients with distant metastases; positive lymph nodes; stage T3, T4, or Tx; and ATA high risk of recurrence and who had undergone surgery other than total thyroidectomy (TT) or thyroid lobectomy (TL) were excluded
Propensity matching to create matched sets of TL and TT patients was used
Age, sex, histology, I-131 therapy, ATA risk, and pathologic T and N stage were used as propensity-matching criteria
Pearson’s test or Fisher’s exact test and the t-test were used to compare categorical and continuous variables, respectively
After propensity matching, multivariate analysis of the cohort using Cox proportional-hazards regression was performed
The primary outcomes were overall survival (OS), disease-specific survival (DSS), and recurrence-free survival (RFS)
The Kaplan–Meier method was used to compare the primary outcome, and a log-rank test was used to compare the two groups
Results:
A total of 3756 patients were included in the initial cohort (943 TL and 2813 TT)
The cohort used for analysis was then restricted to 1836 patients (918 patients in each group after propensity matching)
There were no differences in age, sex, histology, T stage, and ATA risk classification
The mean follow-up periods for TL and TT patients were 56.34 and 56.85 months, respectively
When comparing TL with TT, overall survival (10-year OS, 92.2% vs. 91.3%; P = 0.967), disease-specific survival (10-year DSS, 100% vs. 99.1%; P = 0.197), and recurrence-free survival (10-year RFS, 99.5% vs. 98.3%; P = 0.079) were not significantly different
Multivariate analysis showed that between variables of age, vascular invasion, microscopic ETE, margins, and extent of surgery, only age greater than 55 years was a predictor of OS (HR, 5.773; P<0.0001)
There were 67 and 45 deaths in the TL and TT groups, respectively:
Only 1 death was related to thyroid cancer, and it was in the TT group
There were 15 patients with recurrence, 10 (1.08%) in the TT group and 5 (0.05%) in the TL group
The median times from surgery to recurrence were 44.2 and 44.1 months for the TL and TT groups, respectively
There was no statistical difference between the two groups regarding the site of recurrence
Conclusions:
Thyroid lobectomy is associated with mortality outcomes similar to those for total thyroidectomy in selected DTC patients with ATA low and intermediate risk for recurrence
It is reasonable to consider lobectomy in patients with:
Intrathyroidal DTCs less than 4 cm, no nodules in the contralateral lobe, and no suspicious lymph nodes on either preoperative imaging or intraoperative palpation
Thyroid lobectomy is associated with fewer complications such as hypoparathyroidism, recurrent laryngeal nerve injury, and hypothyroidism
However, the extent of thyroid surgery remains the subject of debate between experts despite the reported excellent outcomes in patients with low-risk thyroid cancers <4 cm treated with thyroid lobectomy
This study also supports findings from these other studies in examining the extent of thyroid surgery on the long-term mortality outcomes of patients with low-risk thyroid cancer
Also included in this study were 402 patients with ATA intermediate risk of recurrence:
There were 212 total thyroidectomies and 190 thyroid lobectomies, and no significant differences were identified between the two groups regarding overall survival, disease-specific survival, and recurrence-free survival
Because intermediate-risk features on histology are identified only postoperatively, these patients would usually be advised to undergo completion thyroidectomy
The likelihood of requiring completion thyroidectomy based on intermediate-risk disease has been reported to be around 30% to 60%
However, it has not been proven that completion thyroidectomy has a survival advantage over thyroid lobectomy in all patients with an intermediate risk of recurrence
A study of 341 patients with papillary thyroid cancer (PTC) and intermediate risk of recurrence showed no benefit of total thyroidectomy in recurrence-free survival and disease-specific survival, as compared with thyroid lobectomy
Another study of 129 patients with unilateral micro-PTC and ipsilateral lateral lymph node metastases without gross ETE showed non statistically significant recurrence-free survival between the group of patients treated with thyroid lobectomy plus lymph node dissection and that treated with total thyroidectomy plus lymph node dissection, with 60 months of follow-up
The current study also concludes that thyroid lobectomy has an outcome equivalent to that for total thyroidectomy in selected patients with intermediate risk of recurrence
Additional studies and long-term follow-up are warranted to examine the extent of thyroid surgery in thyroid cancer patients with an intermediate risk of recurrence
It is essential to remember that many of these studies were carried out in a tertiary care center with experienced sonographers and experienced thyroid surgeons
This recommendation may not translate to institutions where there is lower surgical volume and where radiologists may have less expertise in identifying suspicious findings related to thyroid cancer
Patients’ preferences and financial status and ability to attend follow-up visits are also essential factors to consider
Thus, the findings of this study are reassuring to show that selected patients even in this latter group (intermediate risk DTC patients) have similar long-term outcomes after thyroid lobectomy
References
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2016 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 26:1–133.
Toumi A, DiGennaro C, Vahdat V, Jalali MS, Gazelle GS, Chhatwal J, Kelz RR, Lubitz CC 2021 Trends in thyroid surgery and guideline-concordant care in the United States, 2007-2018. Thyroid 31:941–949.
Matsuura D, Yuan A, Harries V, Shaha AR, Tuttle RM, Patel SG, Shah JP, Ganly I 2021 Surgical management of low-/intermediate-risk node negative thyroid cancer: A single-institution study using propensity matching analysis to compare thyroid lobectomy and total thyroidectomy. Thyroid 32:28-36.
The American Thyroid Association (ATA) guidelines recommend that:
Thyroid lobectomy is sufficient:
In low-risk patients with differentiated thyroid cancer (DTC):
However, the corresponding optimal serum TSH level, and thus whether replacement therapy with levothyroxine (LT4) might be advised, in low-risk patients after lobectomy is still a controversial issue
In this study Clin Thyroidol 2022;34:67–70, Xu and coworkers:
Examined the association between post-surgical TSH levels in patients with papillary thyroid carcinoma (PTC):
Who were given LT4 therapy after lobectomy and their risk of structural recurrence
Methods:
This study included adult patients (ages 18 to 75) who underwent thyroid lobectomy for PTC:
At the National Cancer Institute and Hospital at the Chinese Academy of Medical Sciences from January 2000 to December 2014
Patients without advanced tumors or preoperative evidence of distant metastasis, high-risk aggressive variants, and positive surgical margins were included
Staging was assigned according to the American Joint Committee on Cancer staging system (8th edition)
The post-surgical risk stratification was assessed according to the 2015 ATA differentiated thyroid cancer guidelines
All included patients received thyroid hormone replacement therapy as LT4:
Targeting an optimal serum TSH range of 0.5 to 1 mU/L
Serum TSH concentrations were determined by electrochemiluminescence immunoassay with a functional sensitivity of at least 0.01 mU/L and a reference range of 0.5 to 4.0 mU/L
Physical examination, neck ultrasonography, computed tomography or chest radiography, and serum thyroid tests (TSH, thyroglobulin, and antithyroglobulin antibodies) were assessed every 6 months during the first 5 years and every 12 months thereafter
Recurrence-free survival was estimated from the time of surgery for PTC until there was evidence of a structural recurrence
The association of mean TSH and structural recurrence was assessed using univar-iate and multivariate Cox regression models with restricted cubic spline
Results:
The study sample included 2297 patients (median age, 42 years; 76.2% women)
The mean (±SD) tumor size was 1.23 ±0.98 cm, with 59.2% of patients having a tumor < 1 cm
Central neck dissection was performed in 70.9% and lateral neck dissection in 22.6%, respectively
At the initial evaluation, 41.2% patients had low-risk of recurrence, 42.4% had intermediate-risk, and 16.4% high-risk of recurrence, according to the 2015 ATA risk stratification guidelines
The mean post-surgical TSH level in the cohort was 1.456 ± 2.224 mIU/L
Serum TSH values were 0.5 mU/L in 29.1%, in the lower half of the reference range (0.5 to < 2) in 50.6%, in the upper half of the reference range (2.1 to ≤4) in 15%, and above the reference range (>4) in 5.3%
During a median follow-up period of 70 months:
167 (7.3%) patients had structural recurrences and 26 died (11 from PTC)
Local or regional recurrences developed in 84.4% of patients (37 local, 66 regional, and 38 both), whereas distant metastases developed in 26 (isolated in 12 cases and combined with local or regional recurrences in 14)
Recurrences were detected in the:
Residual lobe (n = 71)
Thyroid bed (n = 6)
Central neck (n = 60)
Lateral neck (n = 90)
Recurrence-free survival rates at 5 and 10 years were 94.7% and 84.7%, respectively
81.4% of the recurrences occurred in patients in the intermediate-to-high-risk group
No associations were observed between mean TSH levels and recurrence-free survival in the combined cohort of low-risk and intermediate-to-high-risk groups
The only recurrence-free survival difference observed in the stratified univariate analysis was between patients with mean TSH levels in the lower half of the reference range (0.6–2 mU/L, n = 659) versus those above the reference range (>4 mU/L, n = 68) in the intermediate-to-high-risk group (10-year recurrence-free survival by Kaplan–Meier analysis, 84.4% vs. 69.4%, log-rank P = 0.011)
Conclusions:
In this retrospective cohort study, no associations were observed between the mean postoperative serum TSH levels and tumor recurrence among PTC patients who underwent thyroid lobectomy
The recurrence-free survival rates were similar between patients whose TSH levels were within the reference range and those with suppressed TSH levels
Optimal management of DTC includes:
The avoidance of overdiagnosis and overtreatment in patients with a low risk of disease recurrence
Papillary micro-carcinoma represents a very-low-risk tumor and one for which the ATA supports the possibility of active surveillance as a management option
Furthermore, the ATA recommends thyroid lobectomy for differentiated thyroid cancer:
Greater than 1 cm and less than 4 cm with unifocal and intrathyroidal carcinoma without extra-thyroidal extension and clinical evidence of any lymph-node metastases (cN0), in the absence of prior head and neck radiation, familial thyroid carcinoma or clinically detectable cervical node metastases
This approach has been associated with a favorable outcome and had no negative impact on overall survival according to a systematic literature review
The advantages of lobectomy include:
Fewer surgical complications (less risk of hypocalcemia and recurrent laryngeal-nerve injury) and a lower risk of postoperative hypothyroidism:
A large meta-analasis of 32 studies reported an estimated risk of 12% for subclinical hypothyroidism and 4% for clinical hypothyroidism in patients who undergo lobectomy
For patients with DTC, the ATA guidelines recommend a postoperative TSH level in the mid to lower reference range (0.5–2 mU/L):
Therefore, treatment with LT4 in this group is not necessary when the postoperative serum TSH remains below 2 mIU/L
It should be noted that patients with high pre-operative TSH levels and positive for antithyroid peroxidase antibodies:
Might have an increased risk of developing hypothyroidism after lobectomy
In addition, high postoperative TSH levels (after 1 year):
May identify patients with persistent postoperative hypothyroidism after lobectomy
The disadvantage of lobectomy is:
The need for completion thyroidectomy in patients with:
A high risk for recurrence, worrisome histologic features, malignant new nodules in the contralateral lobe, or evidence of structural disease on imaging during follow-up
In this large retrospective study by Xu et al. that included 2297 patients who underwent lobectomy for thyroid cancer, the surgical pathology revealed that 42.4% of patients had an intermediate risk and 16.4% a high risk for recurrence (defined by the 2015 ATA DTC guidelines), despite the preoperative exclusion of high-risk variants, distant metastases, and positive surgical margins
The fact that a relatively large proportion of patients were at intermediate or high risk and yet did not undergo completion thyroidectomy could explain why structural recurrence developed in 7.3% and thyroid cancer–specific mortality was observed in 11 patients over a follow-up of 70 months
However, despite the inclusion of these patients, serum TSH levels were not associated with recurrence risks, even in the adjusted model restricted to patients with intermediate or high risk for recurrent disease
The risk of thyroid malignancy increases with serum TSH, and higher TSH values (even within the normal range), have been associated with a higher frequency of thyroid cancer in patients with nodular thyroid disease
However, there are conflicting data in the literature concerning the potential role of postsurgical TSH levels regarding the prognosis of low-risk DTC patients
In a retrospective, propensity score–matched cohort study by Park et al:
TSH suppression did not improve clinical outcomes, and serum TSH levels were not associated with recurrence in patients with low-risk DTC who underwent lobectomy
In addition, no difference in the rate of recurrences was reported among patients with TSH values ranging from less than 0.5 to 4.5 mIU/L in a study by Lee et al:
Their analysis showed that there were no differences in recurrence when comparing those with and those without thyroid hormone replacement therapy
These results suggest the necessity of large prospective studies with rigorous criteria to determine the optimal range of serum TSH levels in low-risk DTC patients, including those who undergo lobectomy:
These future studies should consider the risks and benefits of LT4 therapy with regard to thyroid cancer recurrence risks, survival and quality of life measures
The results of these studies could be of significant clinical and psychological importance when recommending the extent of surgery in patients with low-risk DTC
References:
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2016 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 26:1–133
Xu S, Huang Y, Huang H, Zhang X, Qian J, Wang X, Xu Z, Liu S, Liu J 2021 Optimal serum thyroid-stimulating hormone level for patients with papillary thyroid carcinoma after lobectomy. Thyroid. Epub 2021 Dec 31.
Merten MM, Foster T, Lyden M, Henry M, Castro MR 2021 Favorable early outcomes with thyroid lobectomy for low-risk papillary thyroid cancer: the Mayo Clinic experience. Am Surg 87:1374–1378.
Vargas-Pinto S, Romeri-Arenas MA 2019 Lobectomy compared to total thyroidectomy for low-risk papillary thyroid cancer: A systematic review J Surg Res 242:244–251.
Verloop M, Louwerens M, Schoones JW, Kievit SJ, Smit JWA, Dekkers OM 2012 Risk of hypothyroidism following hemithyroidectomy: Systematic review and meta-analysis of prognostic studies. J Clin Endocrinol Metab 97:2243–2455.
Park S, Jeon MJ, Song E, Oh H-S, Kim M, Kwon H, et al. 2017 Clinical features of early and late postoperative hypothyroidism after lobectomy. J Clin Endocrinol Metab 102:1317–1324.7. Fiore E, Vitti P 2012 Serum TSH and risk of papillary thyroid cancer in nodular thyroid disease J Clin Endocrinol Metab 97:1134–1145.
Park JH, Lee YM, Lee YH, Hong SJ, Yoon JH 2018 The prognostic value of serum thyroid-stimulating hormone level post-lobectomy in low- and intermediate-risk papillary thyroid carcinoma. J Surg Oncol 118:390–396.
Park S, Kim WG, Han M, Jeon MJ, Kwon H, Kim M, et al. 2017 Thyrotropin suppressive therapy for low-risk small thyroid cancer: A propensity score-matched cohort study. Thyroid 27:1164–1170.
Lee MC, Kim MJ, Choi HS, Cho SW, Lee GH, Park YJ, Park DJ 2019 Postoperative thyroid-stimulating hormone levels did not affect recurrence after thyroid lobectomy in patients with papillary thyroid cancer. Endocrinol Metab (Seoul) 34:150–157.
Relate to the balance between operative complications and the risk of recurrence
Some suggest total thyroidectomy for goiter:
Others recommend a more conservative initial surgical plan
Some, such as Kraimps, support a selectively aggressive surgical treatment plan based on extent of disease
Complication rates must be kept extremely low in the setting of treatment of benign thyroid disease:
Therefore, I suggest a conservative philosophy:
Tailoring the extent of surgery to the initial disease with the minimum procedure being:
A total unilateral lobar resection:
Reserving bilateral surgery for significant bilateral goiter
Studies looking at the extent of surgery and benign multinodular goiter recurrence are confounded by several factors:
Variability in the initial extent of thyroid gland nodularity
Variability in the extent of recognition of contralateral nodularity at first surgery
Insufficient follow-up periods in many studies
Variable definitions of recurrence:
Some studies, for example, diagnose recurrence based on an asymptomatic, ultrasonographic identification of thyroid nodularity
A more reasonable definition of recurrence is the development of:
Clinical, palpable thyroid enlargement:
Which again meets surgical criteria for goiter treatment
The question is, can less than total thyroidectomy and even hemithyroidectomy:
Be performed if anodular normal tissue is left?
Complication rates of bilateral surgery are expected to be higher than unilateral
Conservative initial surgery also allows a patient to avoid a lifetime of replacement therapy
However, long-term studies show the overall recurrence rate after surgery for goiter:
Is in the range of 15% to 42%
When recurrence occurs and requires revision goiter surgery:
The complication rates are significantly higher than for first-time surgery:
With RLN rates of paralysis ranging from:
3% to 18%
Permanent hyperparathyroidism ranging from:
0% to 25%
The literature offers conflicting conclusions on factors associated with recurrence of goiter:
The duration of postoperative follow-up is important to consider when examining recurrence of goiter
The data offered by Delbridge, Guinea, and Reeve suggest recurrences:
May require 10 to 13 years to manifest
Rojdmark and Jarhult found that the overall recurrence rate rose to:
42% with 30-year postoperative follow-up
Bistrup et al., in a randomized, prospective, non-placebo, controlled study, showed rates of recurrence for nontoxic goiter between:
14% and 22%
They found the extent of surgery did not relate to the likelihood of recurrence
Hegedus, Nygaard, and Hansen found that the weight of thyroid tissue resected was actually greater in those patients who developed subsequent recurrence
However, Berghout et al., with a 7-year follow-up:
Found that unilateral surgery was associated with higher recurrence rates than bilateral surgery
Australian workers have shown that in patients with unilateral disease:
Hemithyroidectomy results in a 12% recurrence rate in the contralateral lobe
Other workers have supported a philosophy of total thyroidectomy or bilateral subtotal thyroidectomy in most patients with goiter
Subtotal thyroidectomy is defined as:
Total lobectomy with a contralateral remnant approximately equivalent to a small normal lobe
Near total thyroidectomy is defined as:
A remnant of several grams is maintained in the contralateral bed typically adjacent to the RLN entry point
In patients who require bilateral surgery:
The technique of subtotal lobectomy has been both recommended and condemned:
Cohen-Kerem, in a study of 124 patients with a follow-up of 7.6 years, noted that with bilateral subtotal technique:
Only 4% of patients required additional surgery
Pappalardo found similar rates of recurrence in 69 patients treated for benign goiter randomized to total versus subtotal procedures
Reeve et al., however, found subtotal thyroidectomy was associated with a 23% recurrence rate
Clearly, less than lobectomy as a minimum procedure is unwise:
Cohen-Kerem et al. found a recurrence rate after unilateral subtotal resection was 60%
Kocher noted an 18% recurrence rate with nodule enucleation
Kraimps, using a selectively aggressive surgical treatment plan based on the extent of disease, noted very low recurrence rates of 1% with lobectomy and 3% with bilateral surgery:
Others have supported such a selectively aggressive approach to surgery based on extent of disease
Modern series show that in skilled hands:
Total thyroidectomy for goiter can be performed without significant complications, given the work of Reeve et al., Netterville et al., and others
Delbridge, Guinea, and Reeve noted that for patients with bilateral multinodular goiter, total thyroidectomy:
Can be associated with permanent paralysis of the RLN in 0.5% and permanent hypoparathyroidism in 0.4%
They believe the policy of autotransplantation of at least one parathyroid during each total thyroidectomy is in part responsible for the low rate of hypoparathyroidism
Grant, in his commentary of this article, wrote, “to consider total thyroidectomy as the only acceptable alternative would probably risk causing more cases of troublesome hypoparathyroidism than it would prevent cases of goiter recurrence:
Moreover, it seems difficult to assert total thyroidectomy as the only option for benign disease when many surgical authorities strongly disagree with its use, even in thyroid cancer
Some workers have suggested that the likelihood of identifying cancer in goiter specimens justifies total thyroidectomy:
Most studies document an incidence of malignancy in such specimens of between 3% and 17%:
Most are small, occult, incidentally noted malignancies within otherwise benign multinodular goiters and would not normally justify an aggressive surgical approach
Berghout et al., has suggested a greater likelihood of recurrence in females and in patients with a positive family history of thyroid disease:
Overall, females were found to be three times more likely to require revision surgery
Those with a positive family history of thyroid disease were six times more likely to require revision surgery:
Others have found no such increased risk in these populations
I tend to be more aggressive in females and in those with a positive family history:
Especially if they are young
Summary of the extent of Surgery for Goiter:
Complication rates must be low in the setting of surgery for benign thyroid disease
Less than unilateral lobectomy leads to extremely high recurrence rates and difficult reoperations and is to be condemned
The extent of surgery should be rationally tailored to the extent of initial disease
Dominant goitrous enlargement should be treated with total lobectomy on that side
Preoperative assessment with imaging will help to document the extent of surgery necessary on the contralateral side:
With clear-cut unilateral disease, total lobectomy is appropriate
With clear-cut evidence of bilateral goiter, bilateral surgery is appropriate
Consideration should be given for more aggressive surgery in young females and in patients with a positive family history of thyroid disease who may have a higher recurrence rate
In patients who have required multiple thyroid surgeries for benign recurrence and still have some remnant tissue remaining after the last revision surgery, radioactive iodine ablation can be considered
Hashimoto’s Thyroiditis:
Other variables important during surgery are:
The degree of capsular blood vessel engorgement and friability, and goiter consistency
Goiters that are soft and compressible are more easily manipulated during surgery, whereas those that are firm can be challenging even when of small size
Generally, glands affected by Hashimoto’s thyroiditis are more difficult to work on than the more typical benign adenomatous goiter
Hashimoto’s glands, especially those resulting from the fibrotic variant of Hashimoto’s thyroiditis:
Can be firm and less compressible and have a friable, “sticky” surface, which bleeds easily
Such goiters can be associated with multiple perithyroidal lymph nodes that can sometimes make a surgeon consider papillary carcinoma
Such nodes also make parathyroid identification more challenging
The rare fibrous variant of Hashimoto’s thyroiditis is an especially firm variant:
Which makes the performance of less than total lobectomy challenging