- Just as important as knowing when and how to put a patient on a ventilator:
- It is important to know when and how to remove them from this support:
- Also known as “weaning
- It is important to know when and how to remove them from this support:
- An adage from Critical Care is that preparation for extubation:
- Starts as soon as the patient is intubated
- With COVID-19:
- The patients are generally requiring prolonged periods of intubation:
- With many reports quoting 10 to 14 days
- The patients are generally requiring prolonged periods of intubation:
- Regardless, the onus falls on the clinicians caring for any mechanically ventilated patient to assess the patient’s daily for signs of stability or improvement:
- With any signs of improvement, assessment for extubation readiness should begin
- Patients’ conditions should be assessed continually:
- And once gas exchange and compliance improve:
- The level of support can be reduced
- And once gas exchange and compliance improve:
- For most patients, the first step in moving towards extubation readiness is:
- To move from assist control ventilation to pressure support ventilation:
- Pressure support ventilation:
- Allows for spontaneous ventilation
- The patient engages their diaphragm and sets their own respiratory rate, flow, and tidal volume
- Allows for spontaneous ventilation
- Pressure support ventilation:
- To move from assist control ventilation to pressure support ventilation:
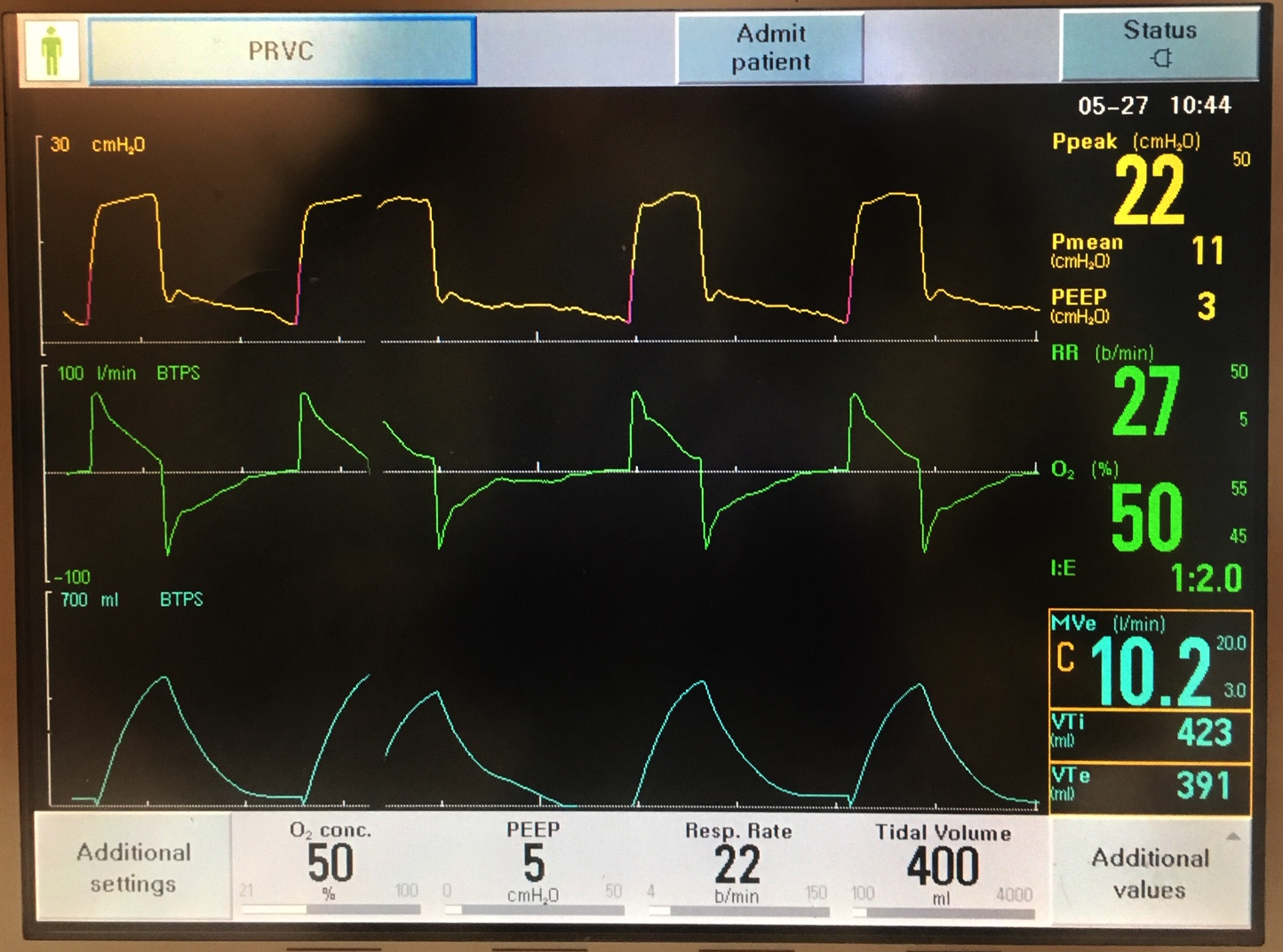
- The following ventilator screen illustrates a patient who is ready to be changed to pressure support:
- The patient was arousable with:
- Lightening sedationhas
- Has good pulmonary mechanics as indicated by:
- The low PIP of only 22 with a TV of 400, has a low PEEP requirement, and is only on 50% FiO2
- On these settings, the patient’s ABG was also reassuring, at 7.37/38/110:
- Note:
- In addition to changing to pressure support, the FiO2 could also be decreased to 40% given the more than adequate PaO
- Note:
- The patient was arousable with:
- Once the patient has been placed on pressure support:
- Physiological measurements including:
- MIP (maximal inspiratory pressure),
- frVt (respiratory frequency to tidal volume ratio, or
- Rapid shallow breathing index
- and others can be used to assess a patient’s readiness to wean
- Physiological measurements including:
- If the following criteria are met:
- The patient should undergo a spontaneous breathing trial (SBT) to determine if they are ready to attempt extubation
- Criteria for Performing Spontaneous Breathing Trial:
- Improvement of underlying condition that led to intubation
- Relative hemodynamic stability
- HR < 130 beast per minute
- Mean arterial pressure (MAP):
- Adequately supported on a stable dose of vasopressors
- Presence of a cough reflex:
- Often elicited by suctioning
- Burden of secretions that can be handled by cough strength:
- Patients with a robust cough will be able to clear more secretions
- Adequate oxygenation:
- Usually SpO2 > 90% on 40% FiO2 and PEEP ≤ 8
- Ability to maintain the current oxygenation status once extubated
- Adequate ventilation:
- pH > 7.3 with a PCO2 near baseline
- Minute ventilation that a patient can maintain after extubated:
- Usually < 12 L/min
- Minimal ventilator settings:
- On pressure support ≤ 10 cmH2O
- On PEEP ≤ 8 cmH2O
- Maintaining tidal volumes ≥ 5 mL/kg PBW
- Respiratory rate < 35
- FiO2 ≤ 50%
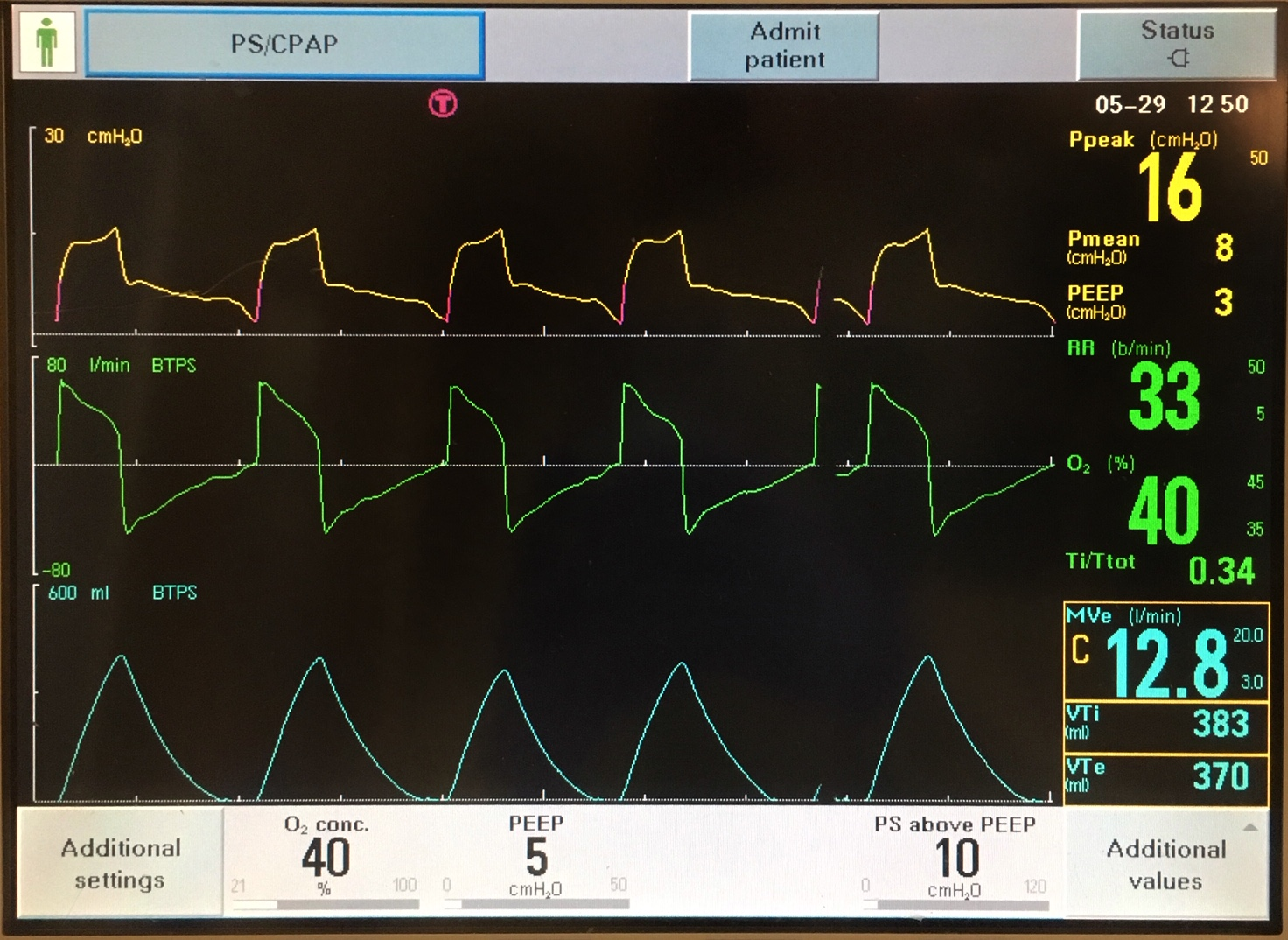
- The following screen shows a patient on pressure support, 10/5 (10 cm H20 driving pressure over 5 cm H2O of PEEP):
- This patient is marginal, as the tidal volume with 10 cm H2O of driving pressure is 400, which is acceptable, but the respiratory rate is 30:
- The patient should be assessed for non-pulmonary causes of tachypnea:
- Such as pain, anxiety/agitation, fever, etc
- It is reasonable to decrease the pressure support of 10 cm H2O and reassess both the tidal volumes and respiratory rate
- It is difficult to predict how patients will do; often the best course is to give them a trial and assess
- The patient should be assessed for non-pulmonary causes of tachypnea:
- This patient is marginal, as the tidal volume with 10 cm H2O of driving pressure is 400, which is acceptable, but the respiratory rate is 30:
- Spontaneous breathing trials are used to:
- Assess a patient’s readiness to wean by removing ventilation support for 30 minutes and evaluating the patient’s ability to breathe on their own during this time
- There are many ways to perform SBTs, including:
- Pressure support of 5/5, 0/5, and 0/0, as well as “T-piece trials” in which the patient is taken off the ventilator and supported with blow-by humidified oxygen
- Each approach has its proponents, and institutional guidelines vary
- The most important concept to consider is the available respiratory support options once the patient is intubated, and ensure they are able to pass with that level of support
- Criteria for Passing Spontaneous Breathing Trials:
- Clinical Appearance:
- No evidence of respiratory distress:
- Cyanosis
- Diaphoresis
- Accessory muscle use
- Grimacing
- No evidence of respiratory distress:
- Pulmonary mechanics
- Ratio of respiratory rate : tidal volume:
- Less than 105
- Respiratory rate less than 30 breaths per minute
- Tidal volume less than 5 mL/kg PBW
- Ratio of respiratory rate : tidal volume:
- Oxygenation and ventilation:
- SpO2 ≤ 50%
- PaC02 ≤ 50mmHg or a
- pH ≥ 7.3 or decrease in pH of ≤ 0.07
- Hemodynamics:
- Change in SBP to > 90 or < 180 mmHg
- HR < 130 beats per minute
- New dysrhythmias
- Clinical Appearance:
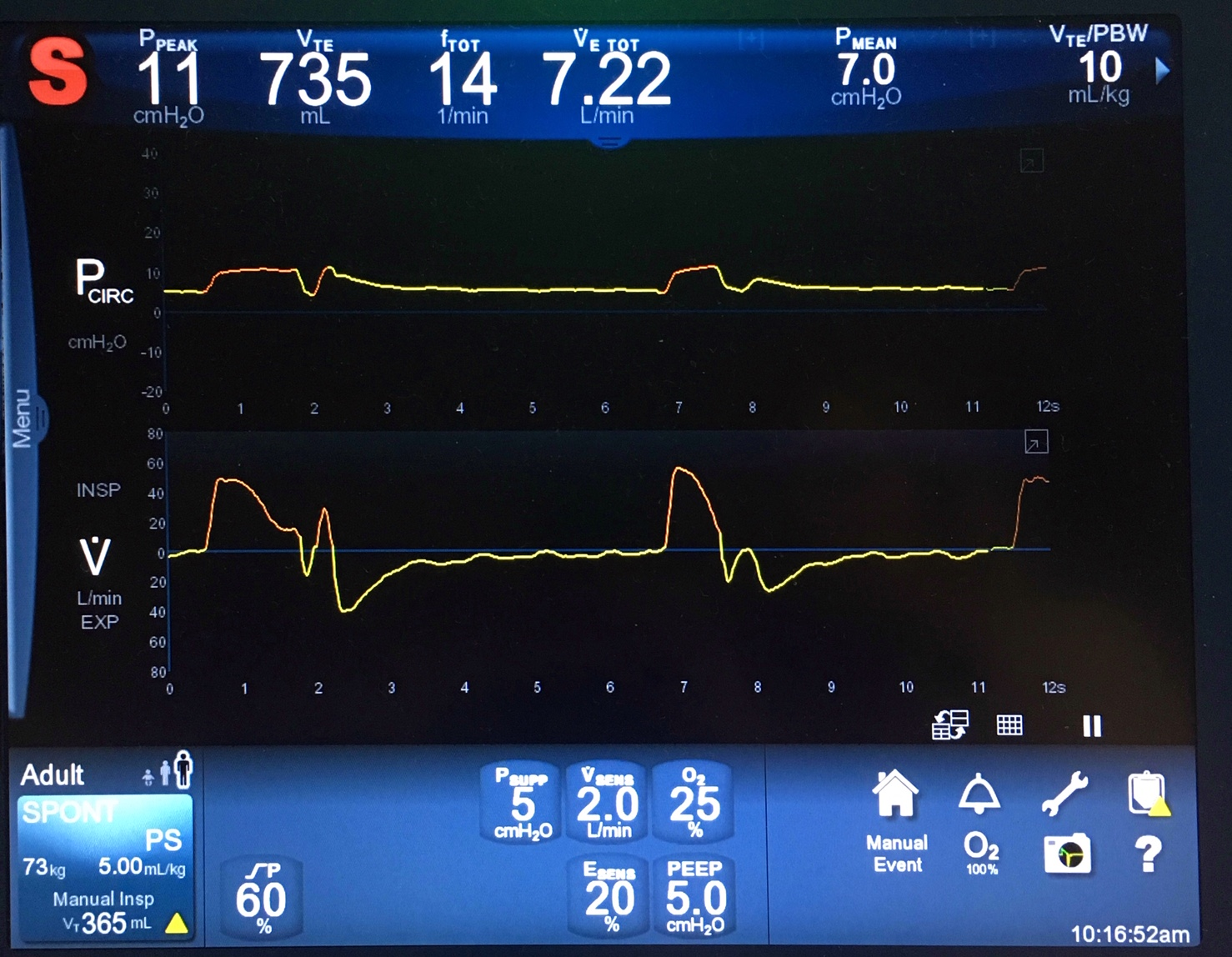
- The screen below demonstrates a patient who is doing well on an SBT:
- They are on pressure support, 5/5, and have large tidal volumes of 735 mL, indicating good compliance
- They are breathing at a slow rate of 14, and they are on a low FiO2 of 25%
- This patient would be an excellent candidate for extubation, assuming there are no other barriers
- If a patient’s spontaneous breathing trial is successful, the next step is to assess for other barriers to extubation
- A helpful approach is to go head to toe:
- Head:
- Is the patient awake, following commands?
- If not, does the clinician believe s/he will be able to cough and protect the airway?
- Is the patient calm or agitated?
- If agitated, does it seem related to the ETT?
- Is there a plan for agitation management?
- Is pain adequately controlled without inducing somnolence or apnea?
- Is the patient awake, following commands?
- Head:
- Face/Neck:
- Any facial trauma?
- Tongue or lip swelling?
- Note:
- This may be seen in a patient who was previously proned
- Note:
- Tongue or lip swelling?
- Was the patient a difficult intubation?
- Note:
- Does not preclude extubation, but all clinicians should be aware
- Note:
- Does the patient have a cuff leak?
- Any facial trauma?
- Chest:
- Does the patient have any chest trauma/other pathology (eg, rib fractures, etc) that may preclude adequate breathing?
- Abdomen:
- Any planned procedures or diagnostics that should happen before extubation?
- What is the nutrition plan after extubation?
- Should an NG tube be placed for tube feeds before extubation?
- Note:
- Most patients with prolonged intubations have oropharyngeal muscle weakness for days after extubation, precluding normal feeding
- Note:
- If there are no barriers to extubation, the patient may be extubated:
- In preparation, gather supplies that would be needed for oxygenation post-extubation (nasal cannula, oxygen mask, CPAP or BPAP, etc.), as well as supplies that would be needed to intubate the patient again if extubation fails:
- Endotrachial tubes (ETTs) of appropriate sizes
- Bag mask with positive end expiratory-pressure (PEEP) valve
- Airway bougies
- Tube exchangers
- Traditional direct laryngoscope
- Video laryngoscope
- Flexible bronchoscope
- Drugs needed for induction
- Suction catheter
- In preparation, gather supplies that would be needed for oxygenation post-extubation (nasal cannula, oxygen mask, CPAP or BPAP, etc.), as well as supplies that would be needed to intubate the patient again if extubation fails:
- For extubation:
- Put the patient in an upright, seated position
- Suction the ETT and oral cavity
- Remove all secretions above the ETT cuff using subglottic suction, if available, or insert a small bore catheter on the side of the ETT for removal of secretions above the ETT cuff
- Remove the ETT from the holder
- Ask the patient to take a deep breath and exhale
- During exhalation, deflate the cuff and smoothly remove the ETT
- Note:
- If an orogastric tube is present, it will be removed alongside the ETT and may need to be replaced by a nasogastric tube, if the patient is not ready for oral intake of medications and nutrition
- Note:
- Suction the oral cavity
- Ask the patient to take a deep breath and cough out all secretions
- Provide supplemental oxygen through a nasal cannula, oxygen mask, etc., as appropriate
- After extubation, it is important to monitor the patient carefully:
- Make sure they have adequate oxygenation and provide supplemental oxygen as appropriate
- If necessary, consider CPAP/BPAP if a patient requires additional support
- Use bronchodilators as needed, provide secretion management, maintain airway hydration and patent central airway, and encourage patient behaviors that reduce the potential for re-intubation:
- Coughing
- Deep breathing
- Sitting up
- Moving around if appropriate
- Risk factors that suggest a patient will need to be re-intubated include:
- Pneumonia
- Weak cough
- Frequent suctioning
- Rapid shallow breathing index > 58 breaths per minute per liter
- Positive fluid balance in the 24 hours prior to extubation
Extubation process and post-extubation recommendations modified from Saeed F, Lasrado S. Extubation. [Updated 2019 Jul 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539804/
#Arrangoiz #Surgeon #Teacher
