Asthma
- In asthma:
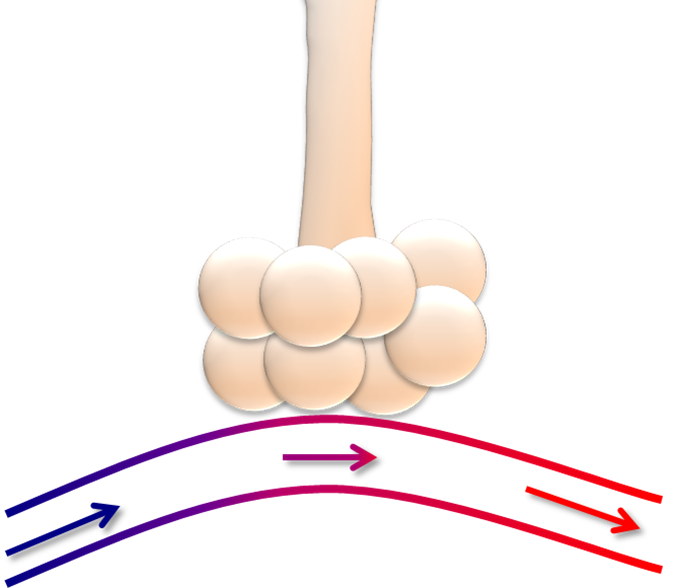
- The patient has a constriction of the bronchial smooth muscles in the airways:
- Leading to reversible air trapping:
- This is indicated in the picture:
- Note that the bronchial muscles do not extend into the small airways
- This is indicated in the picture:
- Leading to reversible air trapping:
- The patient has a constriction of the bronchial smooth muscles in the airways:
- Intubation of an asthmatic is a dreaded complication of this illness:
- As asthmatics can deteriorate rapidly on the ventilator:
- Without close monitoring and active management
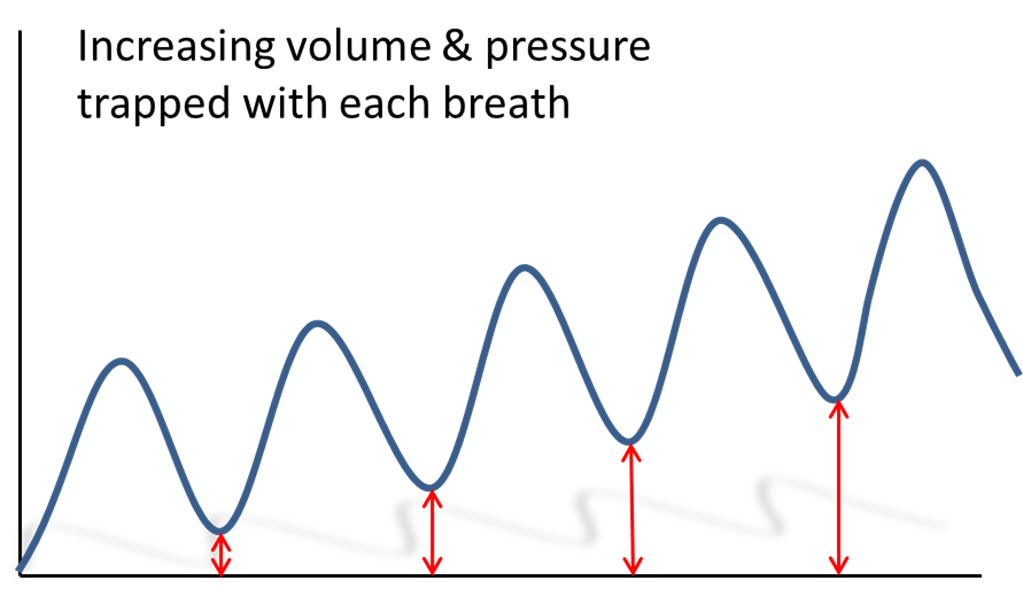
- The goal with a ventilated asthmatic:
- Is to prevent breath-stacking or autoPEEP:
- And the hemodynamic instability that can result
- Is to prevent breath-stacking or autoPEEP:
- As asthmatics can deteriorate rapidly on the ventilator:
- Clinicians should note that intubation of an asthmatic:
- Should trigger even more active management with medications, rather than less
- Intubated asthmatic patients should continue to receive aggressive treatment with:
- Bronchodilators
- Steroids
- Magnesium
- As well as deep sedation:
- Possibly even neuromuscular blockade in the initial hours after intubation:
- In an effort to relax the chest wall musculature and gain control of the situation
- Please note that neuromuscular blockade:
- Only works on skeletal muscle and therefore:
- Will not bronchodilate smooth muscle in the airways
- Only works on skeletal muscle and therefore:
- Possibly even neuromuscular blockade in the initial hours after intubation:
- In addition:
- It is very critical to be aware of the patient’s intravascular volume status:
- As the excess positive pressure:
- Can lead to hemodynamic collapse
- As the excess positive pressure:
- Moreover, the excess pressure, including the auto-PEEP:
- Can result in barotrauma:
- Such as the development of a pneumothorax very quickly in this patient population
- Can result in barotrauma:
- It is very critical to be aware of the patient’s intravascular volume status:
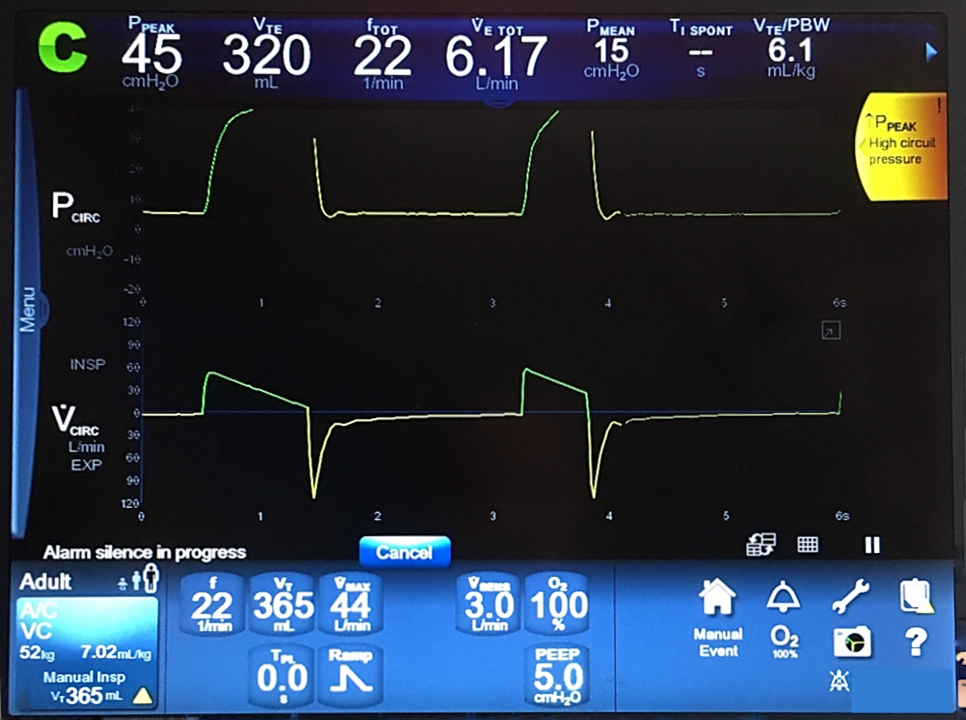
- The ventilator screen below demonstrates the effects of reactive airways disease on pulmonary mechanics:
- This patient had unexpected bronchospasm after being intubated:
- Note the elevated peak inspiratory pressure (PIP) of 45 despite the relatively low tidal volume of 365:
- The patient’s resistance was too high for her to even receive the full tidal volume, as the ventilator was only able to deliver 320 ml before stopping
- Note the elevated peak inspiratory pressure (PIP) of 45 despite the relatively low tidal volume of 365:
- This patient had unexpected bronchospasm after being intubated:
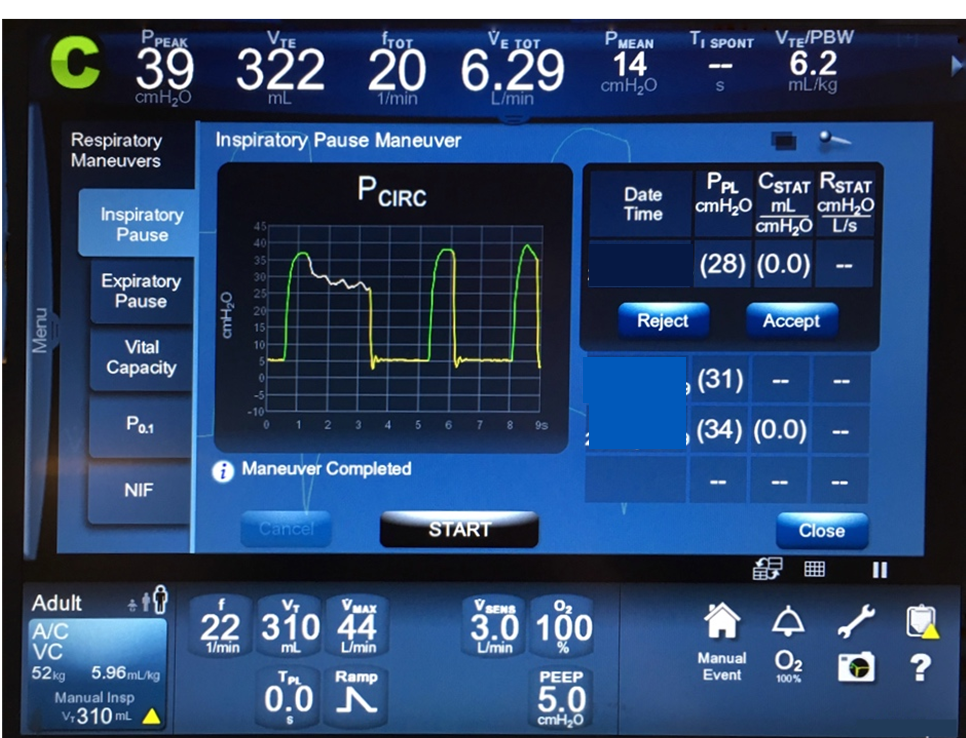
- Checking the plateau pressure (Pplat):
- Confirmed that this was a resistance problem, rather than a pure compliance problem:
- Her PIP was 39 at the time the inspiratory hold was performed:
- But her Pplat was only 28:
- The delta between 39 and 28 indicates a significant resistance component
- But her Pplat was only 28:
- Her PIP was 39 at the time the inspiratory hold was performed:
- Confirmed that this was a resistance problem, rather than a pure compliance problem:
- This patient was treated with continuous bronchodilators with rapid improvement in the bronchospasm:
- Her PIP returned to normal within minutes
- Four ventilator maneuvers:
- Increase expiratory time:
- Decreasing the respiratory rate
- Decreasing the I:E ratio
- Decreasing the inspiratory time
- Increasing the inspiratory flow
- Of these, decreasing the respiratory rate is the most effective means:
- To allow more time to exhale
- Of these, decreasing the respiratory rate is the most effective means:
- Increase expiratory time:
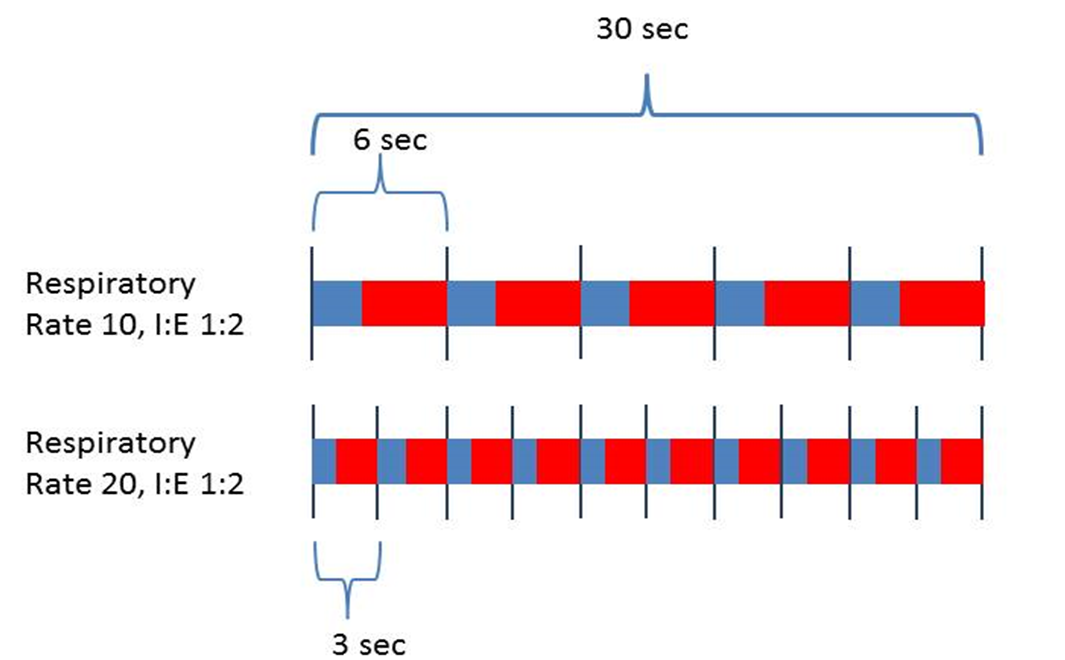
- The figure shows a picture of 30 seconds with two patients, set with the same I:E ratio of 1:2:
- The first patient:
- Has a rate of 10 breaths per minute:
- Allowing 6 seconds per breath cycle
- Has a rate of 10 breaths per minute:
- The second patient:
- Has only 3 seconds per breath cycle:
- Given the respiratory rate of 20
- The blue represents inspiration, the red the time for exhalation:
- Note that even with the same I:E ratio:
- The lower rate offers a substantially longer time to exhale
- Note that even with the same I:E ratio:
- The first patient:
- In looking further at this diagram:
- One can imagine the effects of changing the I:E ratio, the inspiratory flow, or the I time:
- The following figure shows a hypothetical example of the effects of these changes in a patient on volume control:
- In a given patient, the exact values will vary, but the purpose of the illustration is to show the relationship among the parameters of:
- I:E ratio, inspiratory time, and inspiratory flow
- In a given patient, the exact values will vary, but the purpose of the illustration is to show the relationship among the parameters of:
- The following figure shows a hypothetical example of the effects of these changes in a patient on volume control:
- One can imagine the effects of changing the I:E ratio, the inspiratory flow, or the I time:
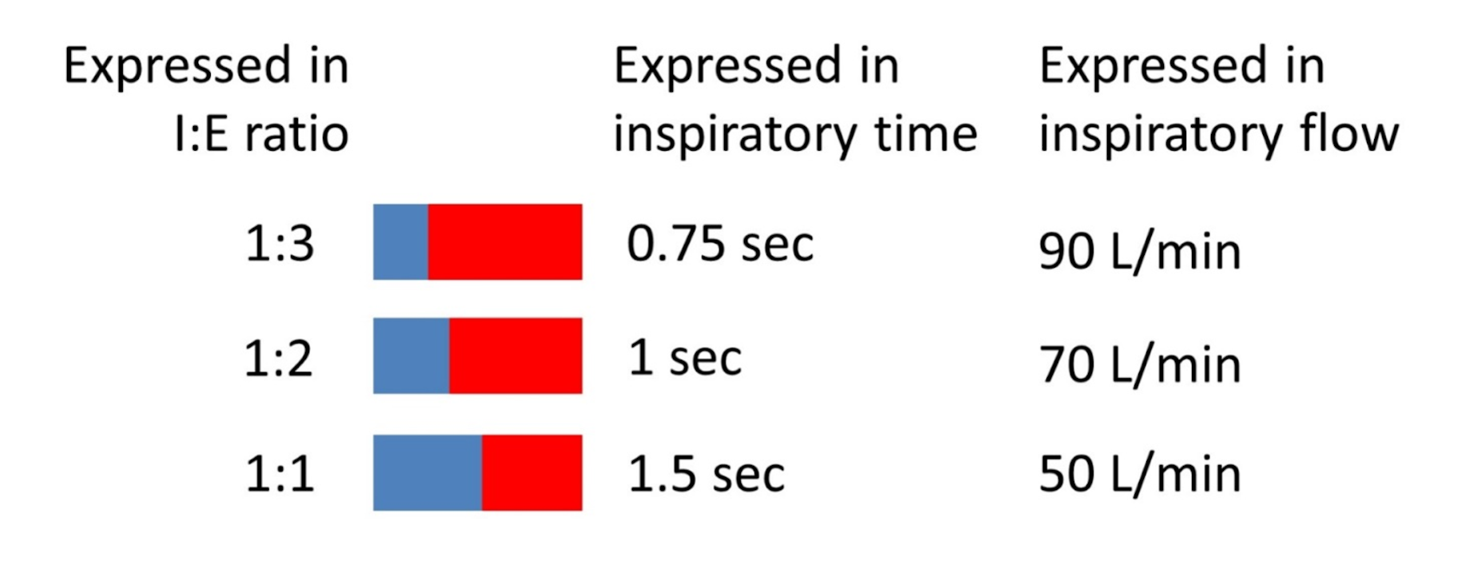
- In addition to a slow respiratory rate, a low I:E ratio, a short inspiratory time and/or a fast inspiratory flow rate:
- Asthmatics should also be ventilated with:
- Low tidal volumes:
- Considering that the larger the tidal volume:
- The more the patient has to exhale
- Considering that the larger the tidal volume:
- Low tidal volumes:
- Asthmatics should also be ventilated with:
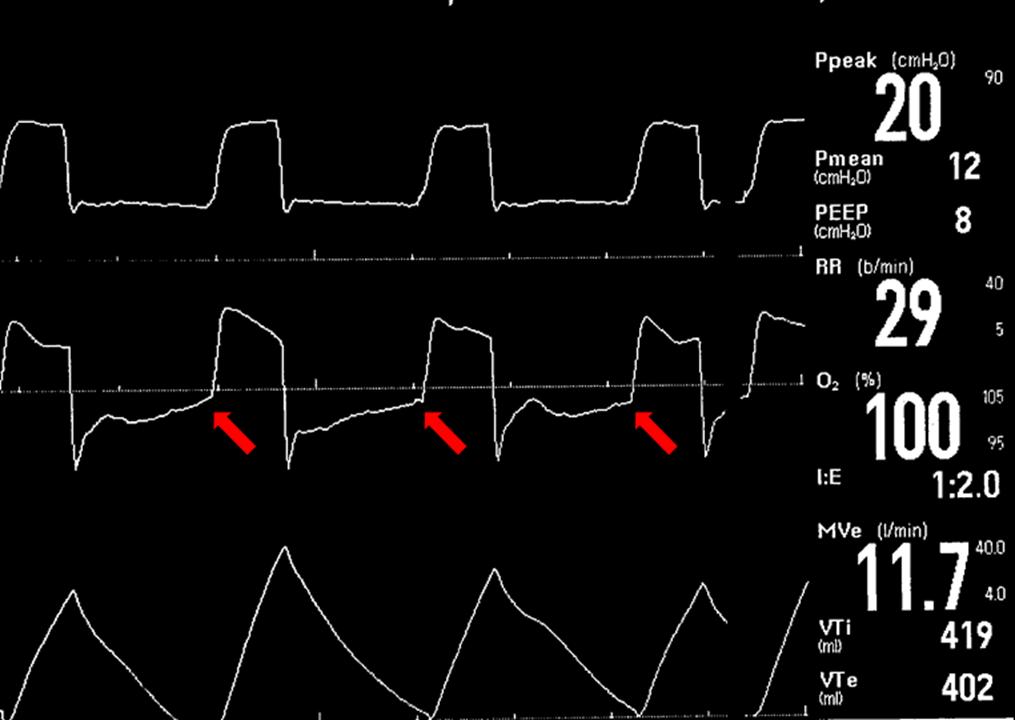
- In monitoring an intubated asthmatic, looking for air trapping is key:
- In the ventilator tracing below, note that the flow tracing, in the middle, does not return to the baseline before the next breath. (Red arrows):
- This represents that the patient is still exhaling when the next breath is given:
- Leading to air trapping:
- Seeing this pattern on the ventilator can be an early clue that the patient is air trapping
- Leading to air trapping:
- This represents that the patient is still exhaling when the next breath is given:
- In the ventilator tracing below, note that the flow tracing, in the middle, does not return to the baseline before the next breath. (Red arrows):
- In this patient:
- You could first decrease the respiratory rate, or increase sedation if the patient is over-breathing
- The I:E ratio is only 1:2:
- So changing the I time to make a ratio of 1:3 or 1:4 is also appropriate
- Also continued treatment with bronchodilators:
- To decrease the bronchospasm associated with this disease:
- Will also mitigate the excess auto-PEEP
- To decrease the bronchospasm associated with this disease:
- Recall that to quantify the pressure exerted by air trapping:
- One should check for autoPEEP:
- B y checking an expiratory hold button on the mechanical ventilator
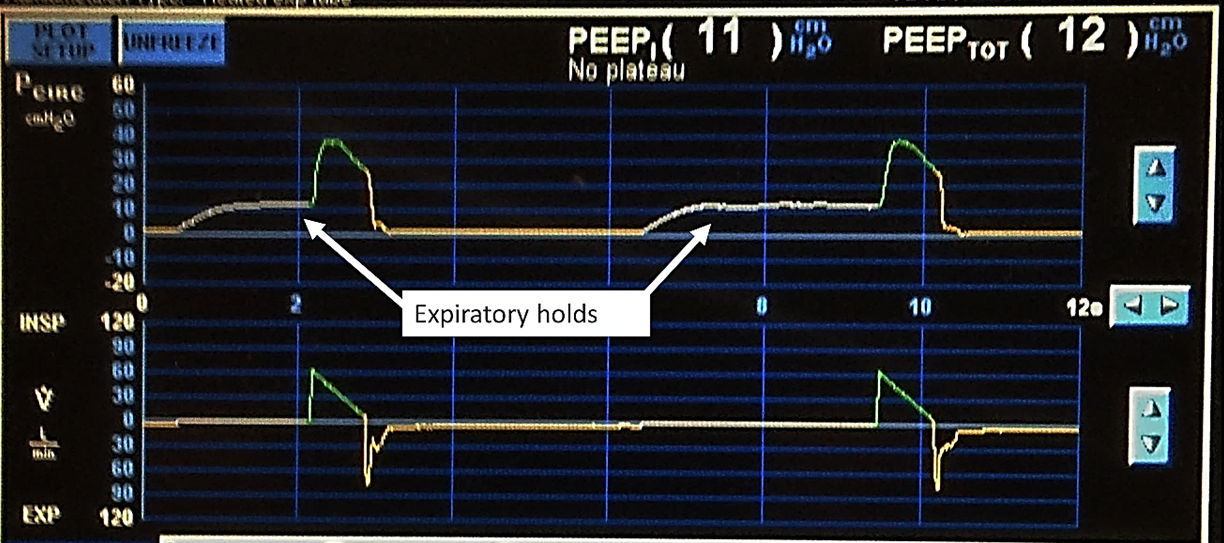
- The intrinsic PEEP is 11, and the total PEEP is 12:
- This indicates that the patient was only set on 1 of PEEP (an unusual – and not recommended – setting, used in this circumstance for demonstration purposes only.)
- Thus, to set the ventilator for an asthmatic, select:
- A low tidal volume:
- 6 to 8 mL/kg of predicted body weight
- The respiratory rate should be low:
- Less than 20 breaths per minute:
- Oten around 10 breaths per minute
- Less than 20 breaths per minute:
- The I:E ratio should be changed to:
- 1:3 or less
- PEEP should be set at:
- 5 cmH2O
- The FiO2 should be down-titrated as tolerated
- These patients continue to receive:
- Heavy sedation
- Possibly NMB if required
- Continuous bronchodilators
- Close monitoring for breath stacking and autoPEEP:
- AutoPEEP should be monitored periodically or after any ventilator change:
- With an expiratory hold
- AutoPEEP should be monitored periodically or after any ventilator change:
- Arterial blood gases (ABGs) should be checked:
- To ensure that the patient is being adequately ventilated
- Heavy sedation
- A low tidal volume:
- Permissive hypercapnia:
- Is the concept of tolerating a PaCO2 greater than 40mmHg and a pH greater than 7.20 to 7.25:
- For the sake of achieving another goal:
- In the case of asthma:
- The goal is to allow time to exhale and prevent air-trapping:
- Permissive hypercapnia is a reasonable strategy:
- Especially early in ventilating the asthmatic
- Permissive hypercapnia is a reasonable strategy:
- The goal is to allow time to exhale and prevent air-trapping:
- In the case of asthma:
- For the sake of achieving another goal:
- Is the concept of tolerating a PaCO2 greater than 40mmHg and a pH greater than 7.20 to 7.25:
- Initial Ventilator Settings in Asthma:
- Tidal Volume:
- 6 to 8 ml/kg PBW
- Respiratory Rate:
- 6 to 14 breaths/minute:
- Allowing for permissive hypercapnia
- 6 to 14 breaths/minute:
- PEEP:
- ~ 5 cmH2O
- FiO2:
- Decrease as tolerated
- SpO2 ≥ 92%
- Tidal Volume:
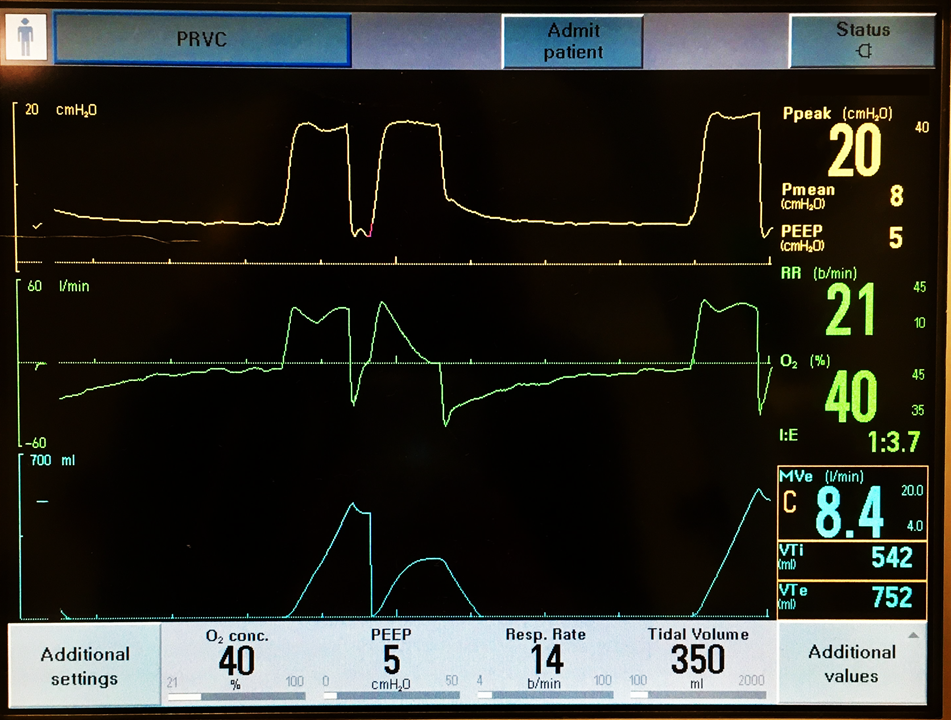
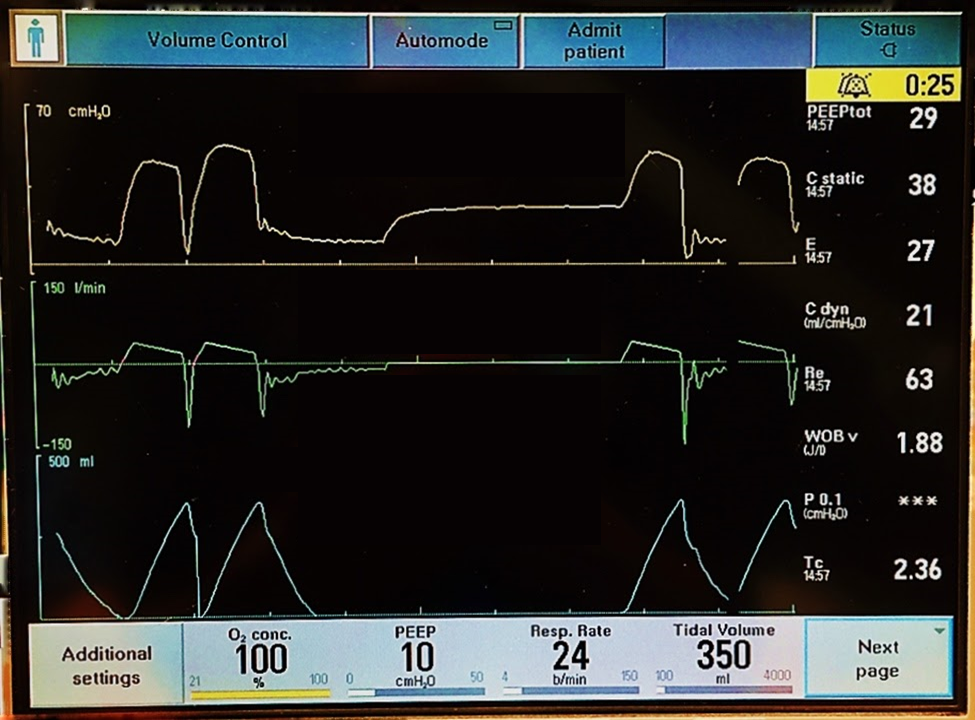
- The following ventilator screen demonstrates these settings:
- The patient is set at 6ml/kg at 350 mls, with a respiratory rate of 14, a PEEP of 5, and a FiO2 40%:
- Note, however, that the patient is not synchronous with the ventilator and is taking large tidal volumes:
- This can be a very dangerous situation, leading to worsening air-trapping and possibly hemodynamic compromise:
- This patient needs to be deeply sedated and neuromuscular blockade administered if needed:
- Additionally, the patient should continue to receive bronchodilators and all other appropriate medical treatments
- This can be a very dangerous situation, leading to worsening air-trapping and possibly hemodynamic compromise:
- Note, however, that the patient is not synchronous with the ventilator and is taking large tidal volumes:
- The patient is set at 6ml/kg at 350 mls, with a respiratory rate of 14, a PEEP of 5, and a FiO2 40%:
COPD
- There are two types of obstructive lung disease falling under the umbrella of COPD:
- Namely:
- Chronic bronchitis
- Emphysema
- While some patients may have one or the other:
- Many will exist on the continuum
- Namely:
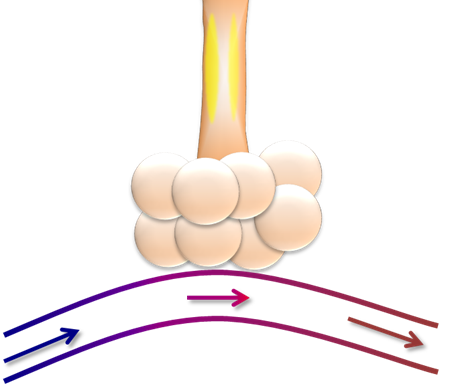
- Chronic bronchitis can resemble the asthmatic schematic above:
- With the notable exception that:
- Muscles hypertrophy and are not entirely reversible
- Additionally, chronic bronchitis is associated with:
- Increased mucous production
- With the notable exception that:
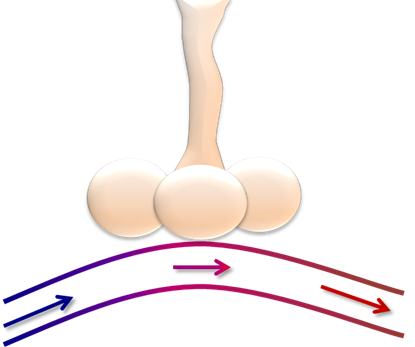
- Emphysema:
- Is a disease of parenchymal destruction:
- Not only is there loss of alveoli:
- Resulting in decreased surface area, or decreased diffusion area (leading to an increased DLCO):
- But the small airways:
- Can become floppy:
- Due to the loss of other tissues holding them open
- Can become floppy:
- But the small airways:
- Resulting in decreased surface area, or decreased diffusion area (leading to an increased DLCO):
- Not only is there loss of alveoli:
- Is a disease of parenchymal destruction:
- Understanding the pathophysiology of COPD is important for considering how to best ventilate these patients:
- It should be noted, however:
- That most patients with COPD have:
- Some mixing of elements of chronic bronchitis and emphysema:
- These conditions exist on a spectrum rather than a dichotomy
- Some mixing of elements of chronic bronchitis and emphysema:
- That most patients with COPD have:
- It should be noted, however:
- Most patients with COPD are now managed:
- With BPAP:
- With improved outcomes over intubation:
- However, on occasion:
- A patient with COPD is not a candidate for BPAP or fails to improve with a trial of BPAP:
- Mandating intubation and invasive mechanical ventilation
- A patient with COPD is not a candidate for BPAP or fails to improve with a trial of BPAP:
- However, on occasion:
- With improved outcomes over intubation:
- Many of the principles that apply in mechanical ventilation for asthma also apply in COPD:
- Both are obstructive diseases, and in both processes:
- The patients require adequate time to exhale:
- Therefore:
- Low tidal volumes
- Low respiratory rates
- Low I:E ratios:
- Are appropriate:
- However, a key difference involves the role of PEEP
- Are appropriate:
- Therefore:
- The patients require adequate time to exhale:
- Both are obstructive diseases, and in both processes:
- Patients with COPD:
- Are at high risk of developing autoPEEP:
- Due to their obstructive disease:
- They require additional time to exhale
- Due to their obstructive disease:
- However, the mechanism of obstruction can differ between asthma and COPD:
- Especially COPD with emphysematous changes as illustrated above:
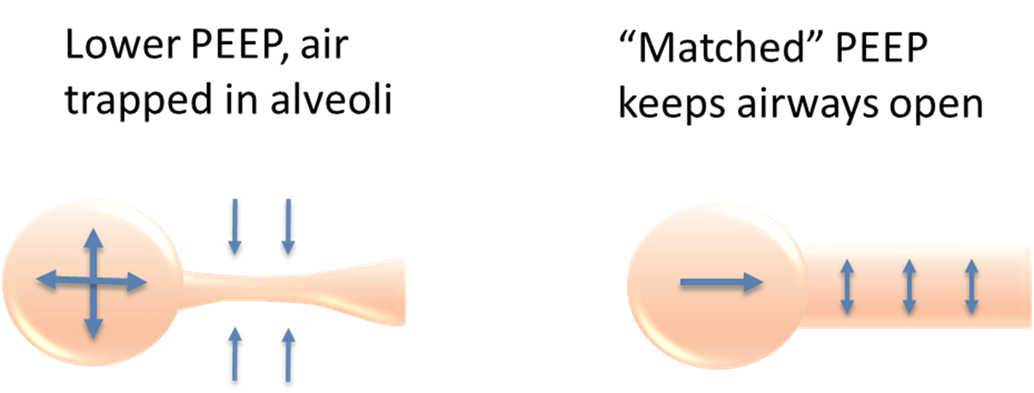
- With the destruction of parenchyma, the small airways can collapse with exhalation:
- Trapping air behind:
- In this circumstance, this trapped air leads to autoPEEP
- Increasing the set PEEP, to match the autoPEEP, is not necessarily an intuitive solution:
- However, as illustrated by the diagram below, increasing the PEEP to prevent collapse of these small airways:
- Can allow the patient to exhale more fully
- However, as illustrated by the diagram below, increasing the PEEP to prevent collapse of these small airways:
- Increasing the set PEEP, to match the autoPEEP, is not necessarily an intuitive solution:
- In this circumstance, this trapped air leads to autoPEEP
- Trapping air behind:
- With the destruction of parenchyma, the small airways can collapse with exhalation:
- Especially COPD with emphysematous changes as illustrated above:
- Are at high risk of developing autoPEEP:
- With BPAP:
- Reexamine the tracing of the figure from the Asthma section:
- Imaging that this patient has COPD:
- If this patient has 11 of autoPEEP, or intrinsic PEEP, what PEEP would you select?
- Imaging that this patient has COPD:
- To match the autoPEEP:
- 11 cmH2O would be an appropriate PEEP selection
- Lastly:
- Patients with COPD are often chronically hypoxemic:
- Indications of chronic hypoxemia physical exam findings of chronic hypoxemia can be demonstrated with nail clubbing
- Additionally, can include an elevated hemoglobin level on the CBC:
- Indicating the patient’s compensation for their chronic lung disease
- Because these patients are baseline hypoxemic, and ventilation is often a relatively greater issue for them than hypoxemia:
- The oxygen saturation for a patient with COPD should be targeted at 88% to 92% in most circumstances:
- This is increasingly important as more data demonstrating the risks of hyperoxia continue to accumulate
- The oxygen saturation for a patient with COPD should be targeted at 88% to 92% in most circumstances:
- Patients with COPD are often chronically hypoxemic:
- Initial Ventilator Settings in COPD:
- Tidal Volume:
- 6 to 8 ml/kg PBW
- Respiratory Rate
- 6 – 20 breaths/minute:
- Allowing for permissive hypercapnia
- 6 – 20 breaths/minute:
- PEEP
- 5 to 15 cmH2O:
- May need to match autoPEEP:
- For patients with significant emphysematous physiology
- May need to match autoPEEP:
- 5 to 15 cmH2O:
- Fi02:
- Decrease as tolerated
- SpO2 target:
- 88% to 92%
- Tidal Volume:
- This ventilator screen demonstrates a patient with COPD with severe dyssynchrony:
- The PIP is 54:
- Indicating severe pathology
- The irregular waveforms:
- Indicate the dyssynchrony
- The patient is set at a respiratory rate of 16 but is breathing at 24
- The PIP is 54:
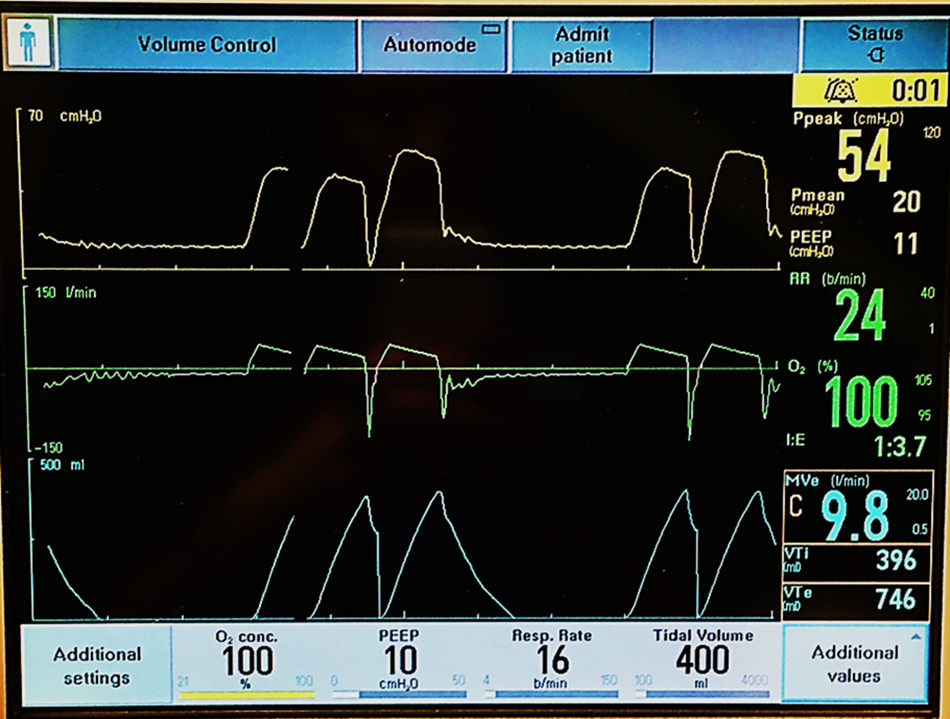
- An expiratory hold was performed and demonstrated a:
- Total PEEP of 29, with a set PEEP of 10
- This indicates a high autoPEEP of 19:
- Therefore, this is a very high-risk situation:
- This patient was deeply sedated, NMB administered, and the ETT was disconnected from the ventilator to allow the patient to exhale
- Therefore, this is a very high-risk situation:
- This indicates a high autoPEEP of 19:
- Total PEEP of 29, with a set PEEP of 10
- Once sedated and relaxed, the patient was placed back on the ventilator at a rate of 12, with frequent expiratory holds to check the autoPEEP
#Arrangoiz #Surgeon #Teacher #CancerSurgeon #MechanicalVentilation
