-
The modern head and neck surgeon / endocrine surgeon / thyroid surgeon should have a complete understanding of the basic science behind the development of the thyroid and parathyroid glands as well as knowledge of the possible congenital abnormalities arising out of these glands, as they may impact the completeness of surgery as well as the complications of surgery:
- The thyroid gland is the first of the body’s endocrine glands to develop appearing as an outpouching of the primitive foregut around the third week of gestation (roughly the 24th day):
- The thyroid gland forms as a proliferation (thickening) of the endodermal epithelial cells found on the median surface of the developing pharyngeal floor:
- The site of this development lies between two key structures:
- The tuberculum impar and the copula, and is recognized as the foramen cecum.
- The site of this development lies between two key structures:
- The thyroid gland forms as a proliferation (thickening) of the endodermal epithelial cells found on the median surface of the developing pharyngeal floor:
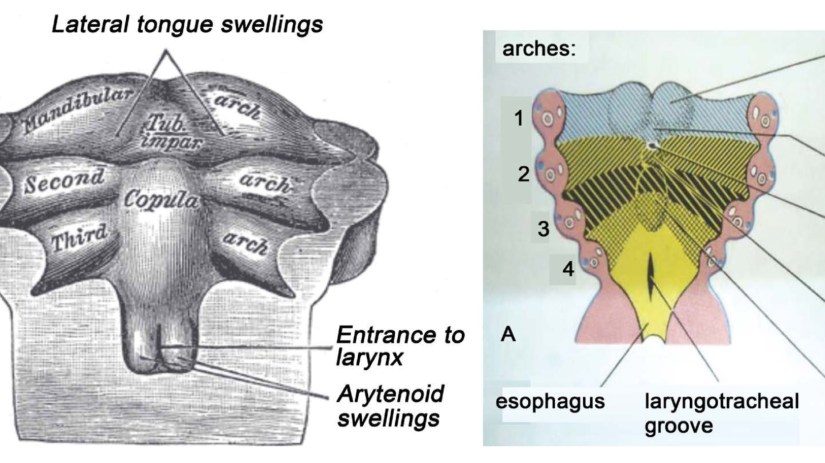
- The foramen cecum located at the base of the tongue is the site of origin of the thyroid gland at the junction between the first and second branchial (pharyngeal) pouches, immediately dorsal to the aortic sac:
- The thyroid gland has a double embryologic origin:
- The primitive pharynx and the neuroectodermal / neural crest.
- The thyroid gland initially arises caudal to the tuberculum impar, which is also known as the median tongue bud:
- This embryonic swelling develops from the first branchial arch and occurs on the mid-line of the floor of the developing pharynx:
- Eventually helping form the tongue as the two lateral lingual swellings overgrow it.
- This embryonic swelling develops from the first branchial arch and occurs on the mid-line of the floor of the developing pharynx:
- The foramen cecum begins rostral to the copula:
- Also known as the hypobranchial (hypopharyngeal) emi- nence:
- This median embryologic swelling consists of mesoderm that arises from the second branchial pouch (although the third and fourth branchial pouches are also involved):
- The thyroid gland, therefore, originates between the first and second branchial pouches.
- This median embryologic swelling consists of mesoderm that arises from the second branchial pouch (although the third and fourth branchial pouches are also involved):
- Also known as the hypobranchial (hypopharyngeal) emi- nence:
- The initial thyroid precursor, the thyroid primordium, starts as a simple mid-line thickening (endoderm) and develops to form the thyroid diverticulum or thyroid anlage (this median anlage forms the bulk of the thyroid gland):
- This structure at the outset is initially hollow:
- Though it later solidifies (forming the follicular elements of the thyroid gland) and becomes bilobed.
- This structure at the outset is initially hollow:
- Division of the thyroid gland into lateral lobes, if not present from the beginning, takes place so early that it is impossible to establish whether the thyroid arises as a single unit or as a paired organ.
- The stalk usually has a lumen, the thyroglossal duct, that does not descend into the lateral lobes.
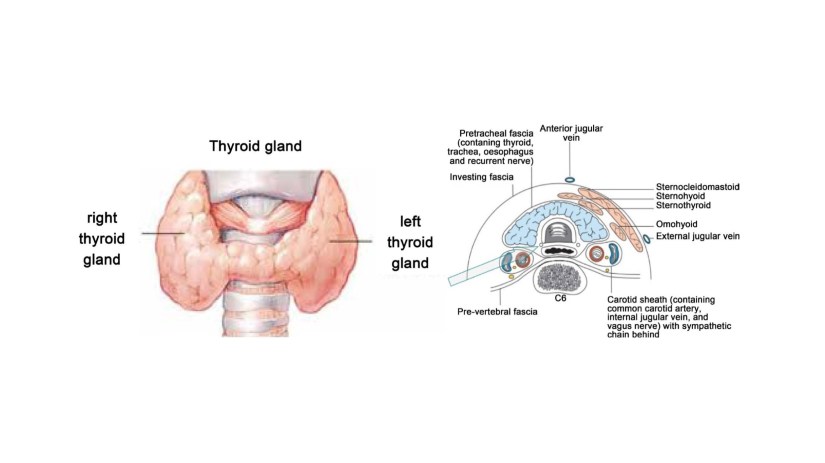
- The two lobes are located on either side of the midline and are connected via an isthmus.
- This thyroid anlage follows the primitive heart as it descends caudally.
- Early during the fifth week of gestation, the attenuated duct loses its lumen and subsequently breaks into fragments:
- The proximal part retracts and vanishes, leaving only the foramen cecum at the base of the tongue to mark its origin, and the caudal end develops as the bilobed encapsulated thyroid gland and reaches its final adult position by the 7th week of gestation.
- The thyroid gland initially arises caudal to the tuberculum impar, which is also known as the median tongue bud:
- The primitive pharynx and the neuroectodermal / neural crest.
- The thyroid gland has a double embryologic origin:
- The paired lateral anlages originate from the ventral portions of the fourth and fifth branchial pouches and fuse with the median thyroid anlage at approximately the fifth week of gestation:
- Contributing up to 30% of the thyroid gland weight.
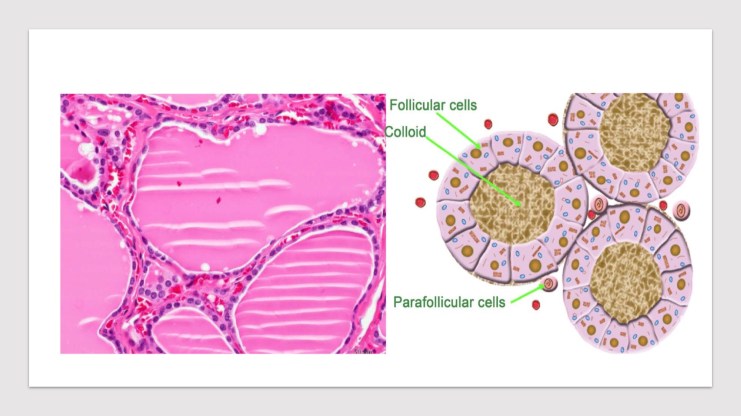
- The lateral anlages are neuroectodermal / neural crest in origin (ultimobranchial bodies) and produce the calcitonin producing parafolicullar or C cells (from the neural crest these the C-cells migrate to the ultimobranchial bodies), which come to lie in the superior posterior region of the thyroid gland.
- The fusion of the median thyroid anlage and the ultimobranchial bodies explains why the parafollicular cells or C cells are not scattered throughout the entire thyroid but are limited to a region deep within the middle to upper thirds of the lateral lobes along an imaginary central lobar axis:
- The bases for the fusion of the median and lateral thyroid anlages is unclear, but the site of the fusion of these two structures is stated to occur at the tubercle of Zuckerkandl.
- The parafolicullar or C cells belong to a group of neural crest derivatives known as the amine precursor uptake and decarboxylation cells (APUD) .
- The fusion of the median thyroid anlage and the ultimobranchial bodies explains why the parafollicular cells or C cells are not scattered throughout the entire thyroid but are limited to a region deep within the middle to upper thirds of the lateral lobes along an imaginary central lobar axis:
-
The thyroid follicular cells develop from the median thyroid anlage and become apparent around the 8th week of gestation and start producing colloid and take up radioactive iodine around the 11th week of gestation:
-
Evidence of thyroxine comes with the appearance of colloid.
-
The development of the thyroid follicle is heralded by the appearance of an intracellular periodic acid-Schiff (PAS)-positive material:
-
Which leads to follicle formation by budding or division of the primary follicles:
-
The histologic differentiation of the thyroid gland can be conceptualized into three stages:
-
Pre-colloid (7 to 13 weeks)
-
Colloid (13 to 14 weeks)
-
Follicular (after 14 weeks)
-
-
-
-

Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
-
He is an expert in the management thyroid diseases.
-
Publication on thyroid embryology and anatomy:
-
Comprehensive Review of Thyroid Embryology, Anatomy, Histology, and Physiology for Surgeons:
-
Arrangoiz, R., Cordera, F., Caba, D., Muñoz, M., Moreno, E. and de León, E.L. (2018) Comprehensive Review of Thyroid Embryology, Anatomy, Histology, and Physiology for Surgeons. International Journal of Otolaryngology and Head & Neck Surgery, 7, 160-188.https://doi.org/10.4236/ijohns.2018.74019
-
-
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

#Arrangoiz#Teacher
#Surgeon
#Cirujano
#ThyroidExpert
#ThyroidSurgeon
#CirujanodeTiroides
#ExpertoenTiroides
#ExpertoenParatiroides
#Paratiroides
#Hiperparatiroidismo
#CancerdeTiroides
#ThyroidCancer
#PapillaryThyroidCancer
