The Society of Surgical Oncology-American Society for Radiation Oncology (SSO-ASTRO) 2014 Consensus Guidelines:
Regarding margins of resection for invasive carcinoma of the breast:
Recommend the use of “no ink on tumor” as the standard of care:
For patients with invasive cancer:
Even with associated ductal carcinoma in situ (DCIS), are treated according to these guidelines
In a meta-analysis of 33 studies including 32,363 patients:
Odds of local recurrence were associated with margin status of positive vs. negative:
But not decreased with increasing margin distance for patients with invasive carcinoma
The study reported that rates of in-breast tumor recurrence are twice as high with positive margins:
Regardless of tumor biology, radiation boost, or endocrine therapy
There was no evidence that wide margins reduce recurrence:
Even in patients with extensive intraductal component
The American Society of Clinical Oncology (ASCO) guidelines:
Recommend consideration of post-excision mammography to document adequate resection in patients with microcalcifications
References
Moran MS, Schnitt SJ, Giuliano AE, et al. SSO-ASTRO consensus guideline on margins for breast-conserving surgery with whole breast irradiation in stage I and II invasive breast cancer. Int J Radiat Oncol Biol Phys. 2014;88(3):553-564.
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21(3):717-730.
Buchholz TA, Somerfield MR, Griggs JJ, et al. Margins for breast-conserving surgery with whole-breast irradiation in stage I and II invasive breast cancer: American Society of Clinical Oncology endorsement of the Society of Surgical Oncology/American Society for Radiation Oncology consensus guideline. J Clin Oncol.2014;32(14):1502-1506.
After a median follow-up of 25.3 months continues to show a significant PFS benefit for the nivolumab / relatlimab combination over nivolumab alone in the first-line treatment of patients with unresectable or metastatic melanoma:
While no new safety findings were noted
Although investigators observed improvements in melanoma-specific survival and OS:
These did not meet the prespecified bar of significance
Analyses of outcomes with subsequent therapy suggested a continued benefit with nivolumab and relatlimab beyond initial treatment and first progression
The dual-checkpoint inhibitor combination of nivolumab and relatlimab continues to provide a significant efficacy benefit over nivolumab alone in patients with previously untreated unresectable or metastatic melanoma:
According to an update from the randomized, double-blind, phase 2/3 RELATIVITY-047 trial presented during the 2023 ASCO Annual Meeting
After a median follow-up of 25.3 months:
Nivolumab and relatlimab continued to demonstrate a consistent, significant improvement over nivolumab in progression-free survival (PFS; HR 0.81, 95% CI [0.67, 0.97]) and a trend toward improved overall survival (OS; HR 0.82, 95% CI [0.67, 1.02])
An exploratory analysis found a numerical improvement in melanoma-specific survival with nivolumab and relatlimab versus nivolumab (HR 0.77, 95% CI [0.61, 0.97])
This updated analysis confirms previous efficacy and safety data reported in the trial
Papillary thyroid carcinoma (PTC) is the most common subtype of thyroid cancer, and its genetics have been extensively studied. Here are some key genetic features and alterations associated with papillary thyroid carcinoma:
BRAF V600E mutation:
The BRAF V600E mutation is the most prevalent genetic alteration in PTC, occurring in approximately 40% to 60% of cases. This mutation leads to the activation of the MAPK signaling pathway, which plays a role in cell growth and proliferation. The presence of BRAF V600E mutation may be associated with a higher risk of disease recurrence and more aggressive tumor behavior.
RAS mutations:
RAS mutations, including NRAS and HRAS, are found in approximately 10% to 20% of PTC cases. These mutations also activate the MAPK signaling pathway, promoting cell growth and proliferation. RAS mutations are more common in older patients and are associated with a lower risk of disease recurrence compared to BRAF mutations.
RET/PTC rearrangements:
Rearrangements involving the RET gene, particularly RET/PTC1 and RET/PTC3, are found in a subset of PTC cases. These rearrangements result in the fusion of RET with other genes, leading to the constitutive activation of the RET tyrosine kinase. RET/PTC rearrangements are more commonly seen in radiation-induced PTC and are associated with a favorable prognosis.
Other genetic alterations:
Other less common genetic alterations found in PTC include NTRK rearrangements, EIF1AX mutations, and TERT promoter mutations. These alterations are present in a small proportion of PTC cases and may have implications for prognosis and targeted treatment strategies.
Adjuvant pembrolizumab continued to demonstrate significant improvements over placebo in DMFS and RFS:
After a median follow-up of 39.4 months
Whereas an earlier analysis suggested that there may be a lesser benefit with pembrolizumab in patients with stage IIC disease:
This was not observed with additional follow-up
The 3-year RFS rates were:
76.2% with pembrolizumab and 63.4% with placebo
In patients with stage IIB / IIC melanoma, adjuvant pembrolizumab provides a:
41% reduction in the risk of distant metastasis or death
38% reduction in the risk of recurrence or death:
According to an update from the KEYNOTE-716 trial presented at the 2023 ASCO Annual Meeting
KEYNOTE-716:
Was the first study to demonstrate a benefit for relapse-free survival [RFS] as well as distant metastasis-free survival [DMFS]:
Using anti–PD-1 immunotherapy (pembrolizumab) in patients with high-risk, non-nodal, stage IIB / IIC melanoma:
This updated analysis support[s] the durability of these findings over time
After a median follow-up of 39.4 months:
Adjuvant pembrolizumab continued to demonstrate significant improvements over placebo in DMFS (HR 0.59, 95% CI [0.44, 0.79]) and RFS (HR 0.62, 95% CI [0.49, 0.79]), consistent with prior reports
The investigators concluded that the results of this analysis support the use of pembrolizumab as adjuvant therapy in patients with resected stage IIB or IIC melanoma:
The effect of adjuvant anti–PD-1 antibodies is similar across stages of melanoma from stage IIB through stage IV resected disease
Having therapeutic options now validated in this setting is a big step forward for our patients and that the results of this final DMFS analysis confirm the important benefit observed in the previous DMFS report and further consolidate the role of pembrolizumab in this setting
Stage IIB / IIC disease is associated with a high risk of relapse
5-year melanoma-specific survival outcomes are similar to those for patients with stage IIIB disease:
Highlighting a need for additional treatment strategies for these patients
The randomized, phase 3 KEYNOTE-716 trial:
Was undertaken to evaluate the efficacy and safety of adjuvant pembrolizumab in patients with:
Newly diagnosed resected stage IIB / IIC melanoma with a negative sentinel lymph node biopsy
A total of 967 patients were randomly assigned to pembrolizumab or placebo:
Administered every 3 weeks for up to 17 cycles
In previous analyses, pembrolizumab demonstrated significant efficacy improvements in RFS and DMFS over placebo
In the last update, after a median follow-up of 27.4 months, median DMFS was not reached in either arm (HR 0.64, 95% CI [0.47, 0.88]; P = .0029)
In the current update:
After a median follow-up of 39.4 months, median DMFS was still not reached in either arm, and there was a consistent benefit with pembrolizumab (HR 0.59, 95% CI [0.44, 0.79];)
The RFS benefit with pembrolizumab was also maintained in the current follow-up:
The 3-year RFS rates were 76.2% with pembrolizumab and 63.4% with placebo, and median RFS was not reached in either arm (HR 0.62, 95% CI [0.49, 0.79])
The DMFS and RFS benefit with pembrolizumab was observed in both stage IIB / IIC melanoma:
An earlier analysis suggested that there may be a lesser benefit with pembrolizumab in patients with stage IIC disease:
This was no longer observed with additional follow-up
We now see that this discrepancy has been resolved with longer follow-up:
The overall impact of pembrolizumab as adjuvant therapy appears to be similar across stages
Safety outcomes were similar to those reported in the previous analyses
Grade 3/4 treatment-related adverse events (AEs) occurred in 17.2% of patients receiving pembrolizumab and 5.1% of those receiving placebo; grade 3/4 immune-related AEs and infusion reactions occurred in 11.0% and 1.2% of patients, respectively.
Treatment-related AEs led to discontinuation in 15.9% of patients receiving pembrolizumab and 2.5% receiving placebo
Investigators noted that the overall survival analyses are forthcoming
Next Steps
Looking ahead, one related area of discussion revolves around the role of sentinel lymph node biopsy for patients with melanoma:
If the patient has a deep primary melanoma, adjuvant pembrolizumab should be discussed with the patient whether the nodes are involved or not:
However, this remains an area of debate
Patient selection beyond the current AJCC classification will be key for the future:
To identify patients with a particularly favorable prognosis for whom treatment could be spared and to identify those patients with a poor prognosis who would benefit from additional therapy:
Biomarker studies are underway to guide us in this important next step
Another area of ongoing research is the potential use of combination immunotherapy regimens in the adjuvant setting:
Among the ongoing trials are:
KEYVIBE-010:
Evaluating pembrolizumab plus the anti-TIGIT antibody vibostolimab in patients with high-risk resected stage IIB, IIC, III, and IV melanoma
KEYNOTE-942:
Evaluating pembrolizumab plus a personalized neoantigen therapy (V940) for high-risk melanoma
References
Luke JJ, Rutkowski P, Queirolo P, et al. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet. 2022;399(10336):1718-1729.
Long GV, Luke JJ, Khattak MA, et al. Pembrolizumab versus placebo as adjuvant therapy in resected stage IIB or IIC melanoma (KEYNOTE-716): distant metastasis-free survival results of a multicentre, double-blind, randomised, phase 3 trial. Lancet Oncol. 2022;23(11):1378-1388.
Gershenwald JE, Scolyer RA, Hess KR, et al. Melanoma staging: evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(6):472-492.
Egger ME, Bhutiani N, Farmer RW, et al. Prognostic factors in melanoma patients with tumor-negative sentinel lymph nodes. Surgery. 2016;159(5):1412-1421.
Patients diagnosed with estrogen receptor (ER)-positive breast cancer receive standard-of-care adjuvant treatment:
However, patients can experience disease recurrence:
With many recurrences occurring within the first 5 years
When disease recurrence does occur, it is often at a more advanced stage when the disease may be incurable:
Therefore, it is critical to prevent recurrences to better reach the original curative intent of treatment
Prior research demonstrated that ribociclib plus endocrine therapy:
Yielded significant improvements in overall and progression-free survival in patients with HR-positive / HER2-negative advanced breast cancer:
Based on that, NATALEE was designed to evaluate the combination in patients with early-stage disease
Another CDK4/6 inhibitor, abemaciclib, is U.S. Food and Drug Administration (FDA) approved for adjuvant treatment of adult patients with HR-positive / HER2-negative, node-positive early breast cancer at high risk of recurrence
What NATALEE now does:
If the FDA acknowledges the data for registration:
It enlarges the patient population who will have access to a CDK4/6 inhibitor
NATALEE was designed to evaluate the combination of ribociclib plus endocrine therapy in patients with early breast cancer
There was a trend toward improved OS with ribociclib plus endocrine therapy, and a 3-year treatment duration of ribociclib 400 mg showed a predictable safety profile that was more favorable than the 600 mg dose of ribociclib used in the metastatic setting
Follow-up data is still being collected, and further quality-of-life results will be provided later in the year
The combination of CDK 4 / 6 inhibitor ribociclib plus endocrine therapy significantly improved invasive disease-free survival (iDFS) compared with endocrine therapy alone in a broad population of patients with stage II or III HR-positive /HER2-negative early breast cancer:
According to results of the second interim efficacy analysis of the phase 3 NATALEE study
With a median follow-up for iDFS of 27.7 months:
The risk for invasive disease was reduced by 25.2% with ribociclib plus endocrine therapy compared with endocrine therapy alone (HR 0.748, 95% CI [0.618, 0.906]; P = .0014)
The 3-year iDFS rate was 90.4% for the combination therapy compared with 87.1% for endocrine therapy alone:
Which is an absolute difference of 3.3%
These results support ribociclib plus endocrine therapy as a new and effective treatment of choice for a broad population of at-risk patients with stage II or III HR-positive / HER2-negative early breast cancer, which is easy to identify in clinical practice
Understanding the genetic mutations associated with thyroid cancer has become increasingly important. The most common genetic mutations found in thyroid cancer include BRAF, RAS, RET/PTC, and PAX8/PPARγ. These mutations can provide valuable information for diagnosis, prognosis, and targeted treatment approaches.
Molecular testing, such as next-generation sequencing (NGS), has gained prominence in thyroid cancer diagnosis and management. It allows for the identification of specific genetic alterations and can guide treatment decisions. Testing for specific genetic mutations, such as BRAF V600E, may help determine the use of targeted therapies like BRAF inhibitors.
Advances in understanding the molecular alterations in thyroid cancer have led to the development of targeted therapies. Tyrosine kinase inhibitors (TKIs) have shown promise in treating advanced or metastatic thyroid cancer, particularly those with RET rearrangements, BRAF mutations, or vascular endothelial growth factor receptor (VEGFR) mutations.
Immune checkpoint inhibitors, such as pembrolizumab and nivolumab, have shown effectiveness in a subset of patients with advanced or refractory thyroid cancer. These therapies work by unleashing the immune system to target cancer cells. However, response rates can vary, and not all patients will benefit from immunotherapy.
Molecular testing can help refine risk stratification in thyroid cancer. Genetic profiling of the tumor can aid in distinguishing low-risk from high-risk thyroid cancers, allowing for tailored treatment plans and surveillance strategies.
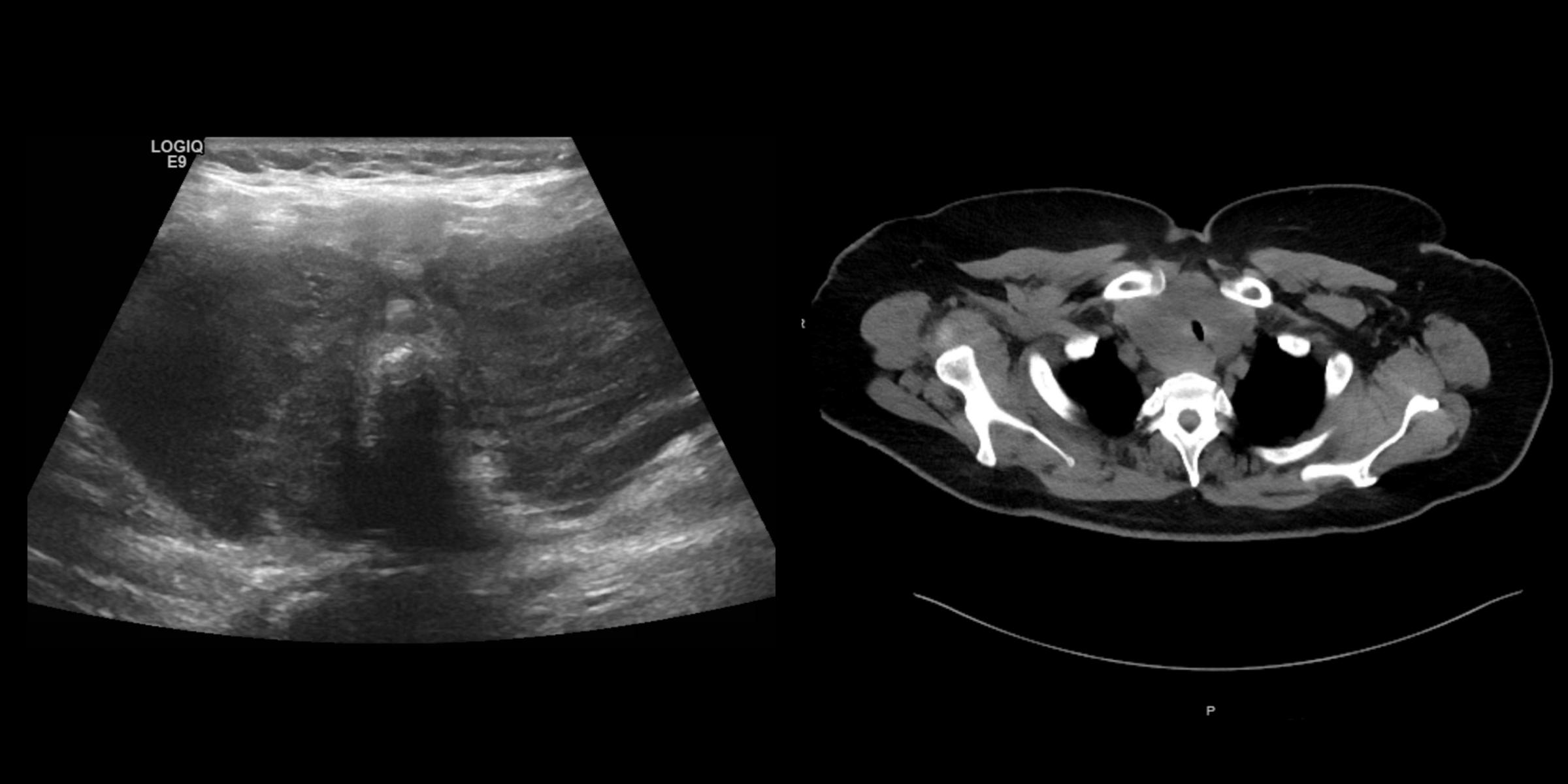
A 61-year-old woman presented to the hospital with dysphagia to solid foods and dyspnea on exertion that has been worsening over the last 1-2 months. Past medical history includes hypothyroidism from Hashimoto’s thyroiditis on levothyroxine, and T2DM on metformin (well-controlled). Physical exam is notable for significant diffuse thyroid enlargement, not rock hard or tender thyroid, positive Pemberton’s sign, hoarse voice (but she is able to speak in full sentences). Biochemical testing revealed normal CBC, CMP, and a TSH of 5.02 uIU/mL (normal 0.5-5.7). Thyroid ultrasound and neck CT are shown below.
What Is the Most Likely Cause for This Finding?
Anaplastic thyroid carcinoma
Fibrous thyroiditis
Subacute thyroiditis
Diffuse large B-cell lymphoma
Mucosa-associated lymphoid tissue (MALT) lymphoma
Correct Answer: Diffuse large B-cell lymphoma
This patient, with a history of Hashimoto’s thyroiditis, presents with a rapidly enlarging thyroid mass that has caused dysphagia and dyspnea on exertion. In that clinical context, the most likely etiology of her symptoms is thyroid lymphoma, and the most common type of primary thyroid lymphoma is diffuse large B-cell lymphoma (DLBCL). Thyroid lymphoma is a rare malignancy representing less than 5% of all thyroid cancers. Hashimoto’s thyroiditis is a well-established risk factor, as patients with Hashimoto’s thyroiditis have a 60 times higher risk of developing primary thyroid lymphoma, compared to the general population. On ultrasound, thyroid lymphoma will appear with diffuse enlargement of the thyroid in a uniform and very hypoechoic pattern, like the one presented here. Usually cross-sectional imaging will be needed, and in this case, there was the apparent narrowing of the upper trachea.
DLBCL usually appears malignant on cytology, while MALT lymphoma can be more subtle, which might result in an Atypia of Undetermined Significance (AUS) by the Bethesda classification. If lymphoma is clinically suspected, it is very important to obtain material for flow cytometry with the biopsy. Treatment of thyroid lymphomas depends on the subtype and staging of the tumor. Usually R-CHOP (rituximab- cyclophosphamide, doxorubicin, vincristine, prednisolone) is used, and no thyroidectomy is recommended.
This patient did not appear to demonstrate hyperthyroidism, nor had a tender thyroid gland, so subacute thyroiditis is unlikely. Fibrous thyroiditis (or Riedel’s thyroiditis) will present with a very hard, fixed goiter. Anaplastic thyroid carcinoma would usually present with asymmetric enlargement of the thyroid, as there is usually a dominant nodule that does not involve the thyroid gland in its entirety